
Abstract
PURPOSE:
This study aimed to examine symptom severity, posture, and balance of children with primary monosymptomatic nocturnal enuresis (PMNE) and compare to a healthy control group.
METHODS:
Thirty-five children with PMNE and 34 healthy children were included in this study. Physical and sociodemographic characteristics of the children were recorded. Symptom severity was assessed with a Vancouver Non-Neurogenic Lower Urinary Tract Dysfunction/Dysfunctional Elimination Syndrome Questionnaire (NLUTD/DES), a four-day bladder diary and a seven-day bowel diary. Standing postural alignment was assessed with the Spinal Mouse device, and the sensory integration of static balance and dynamic standing balance was assessed with the Biodex Balance System SD.
RESULTS:
Compared to healthy controls, children with PMNE demonstrated increased symptom severity (p = 0.001), increased upright lumbar lordosis (p = 0.018) and sacral-hip angles (p = 0.029), decreased static balance in the sensory condition of unstable surface with eyes closed (p = 0.001), and decreased mediolateral dynamic balance (p = 0.049).
CONCLUSION:
Children with PMNE demonstrate altered postural alignment, static and dynamic postural instability, and greater symptom severity on the Vancouver NLUTD/DES than age-matched controls.
Introduction
Nocturnal enuresis (NE) is urinary incontinence at night during sleep in children aged five years or older. NE is defined as primary if nocturnal urinary control has never been achieved and secondary if at least six months of nocturnal continence preceded the onset of incontinence. NE with no other lower urinary tract symptoms (nocturia excluded) is defined as monosymptomatic NE (MNE), while NE with any lower urinary tract symptoms is defined as non-monosymptomatic NE (NMNE) [1]. Thus, primary monosymptomatic nocturnal enuresis (PMNE) is involuntary urinary incontinence while sleeping in children five years and older with no other lower urinary tract symptoms [2].
The pathogenesis of NE is multifactorial and may comprise nocturnal polyuria, nocturnal detrusor overactivity, disturbed sleep/arousal function, genetic factors, and maturational delay [3, 4]. Children with NE have been reported to exhibit abnormal fine and gross motor skills, speech and coordination deficits, attention deficit disorders, sleep architecture changes, academic inadequacy, neuromotor delay, minor neurological dysfunctions, short-term memory dysfunctions, and potential cognitive dysfunctions [2, 5]. It has been reported in the literature that upper brain centers are affected in children with NE; these include thalamus, pons, bulbar, and pons reticular formation areas; bilateral inferior frontal gyrus; and right superior and middle frontal gyrus, which play important roles in continence control [6–9]. These central nervous system (CNS) centers are also involved in the control of posture and balance [10, 11]. Maturational delay of the CNS has been proposed to be a causal factor in NE, and the adverse effects on posture and balance control likely contribute to the delays seen in motor performance [12–14]. Pereira et al. were the first to report impaired standing posture and balance as a result of maturational delay in children with NE [14]. A current review of the literature reveals an absence of studies examining the dynamic balance of children with NE.
The aim of this study was to evaluate the symptom severity, posture, and static and dynamic balance of children with PMNE and compare them with healthy children.
Materials and methods
Participants
Thirty-five children with PMNE who attended the Bolu Abant İzzet Baysal University İzzet Baysal Training and Research Hospital Child and Adolescent Psychiatry Department outpatient clinic and 34 healthy child volunteers acquainted with a study researcher were recruited into the study between 2017–2018 (Fig. 1) [15]. Approval was obtained from Bolu Abant İzzet Baysal University Clinical Research Ethics Committee for the study (Protocol No. 2017/68). This research was supported by Bolu Abant İzzet Baysal University Scientific Research Projects Unit with the project number 2018.14.01.1270. Written and verbal consent was obtained from the child and family after being informed about the study protocol.
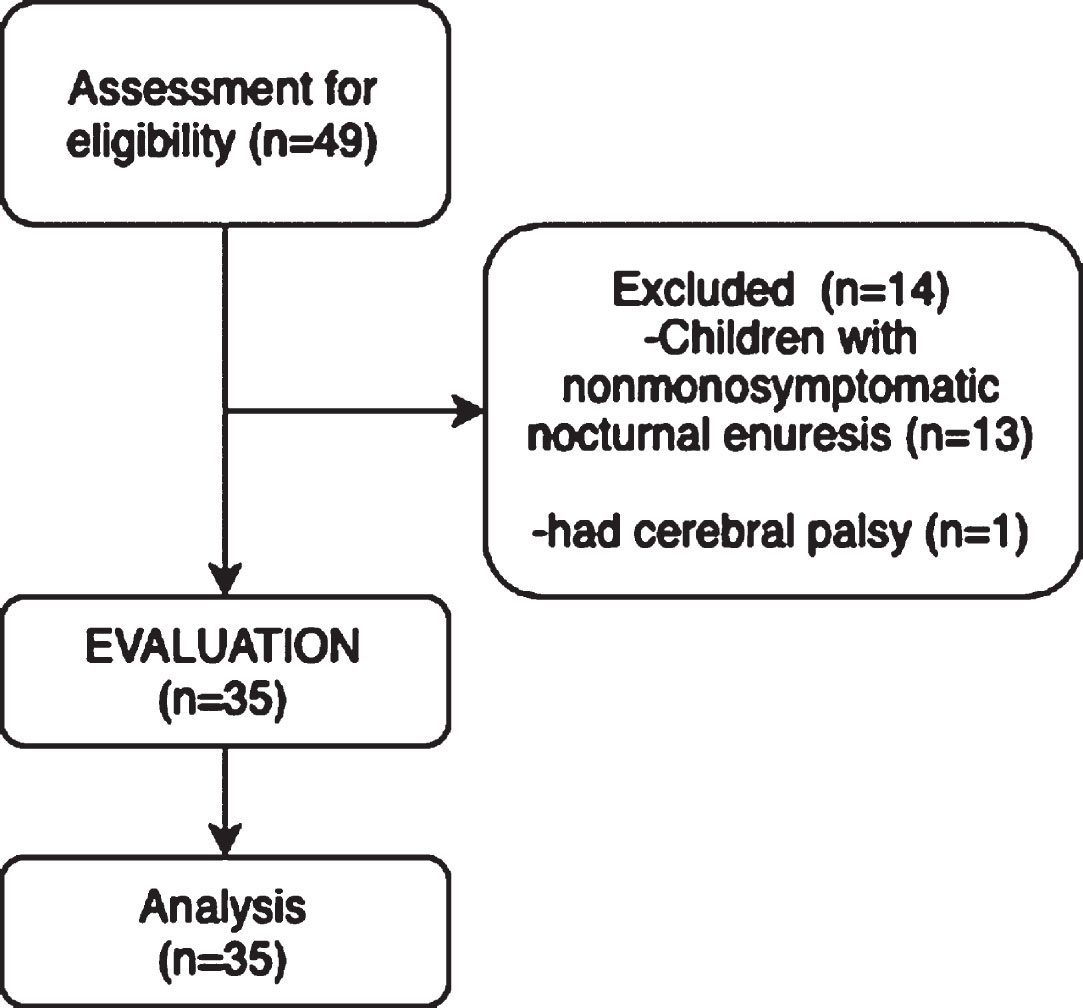
Flow diagram of children with primary monosymptomatic nocturnal enuresis.
Inclusion criteria for children with PMNE were: diagnosed with PMNE, enuresis frequency ≥2 nights per week for ≥3 consecutive months, not being dry for six months after the age of five years, being 6–18 years of age, and voluntary participation in the study. Children who were less than five years old, had anatomical changes in the urinary system, had a neurological disease, chronic disease, cognitive impairment, mental retardation, previous orthopedic surgery, or any lower urinary tract problems were not included in the study.
Assessments
The physical and socio-demographic information of the children (age, height, weight, family structure, type of delivery, gestational age, education time, toilet training age, and duration of breastfeeding) were recorded. The children’s symptom severity, bladder functions, and bowel habits were evaluated with the Vancouver Non-Neurogenic Lower Urinary Tract Dysfunction/Dysfunctional Elimination Syndrome Questionnaire (NLUTD/DES) [16], a four-day bladder diary, and a seven-day bowel diary, respectively. Spinal postures of the children were evaluated with the Spinal Mouse device (Idiag, Volkerswill, Switzerland), and their static and dynamic balance were evaluated with the Biodex Balance System (BBS; Biodex Inc., Shirley, New York).
The Vancouver NLUTD/DES Questionnaire consists of 14 items, scored on a five-point Likert scale ranging from 0 (no complaints exist) to 4 (severe symptoms) [16, 17]. A four-day bladder diary requested children to record daytime urine frequency, nocturia frequency, NE frequency, average urine volume (per day), and daily fluid consumption. A seven-day bowel diary requested children to record daily defecation frequency, duration of defecation, and the feeling of incomplete defecation [1].
The Spinal Mouse, a computer-assisted and non-invasive electromechanical device, was used to evaluate spinal posture in upright standing position. Before the test protocol, the children were informed about the evaluation, then the evaluator palpated the spinous process from C7 to S3 and marked them with a pencil. During the evaluation, the children were asked to be in a relaxed position with the head looking forward, the arms hanging to both sides, the knees straight, and the feet shoulder-width apart. After the evaluation position was assumed, the Spinal Mouse device was moved over each spinous process starting at C7 and continuing down to S3, and one measurement was made in standing upright position [18]. Two rotating wheels of the device followed the spinal curvature. Measurement was made in a quiet and well-lit environment in order not to distract the children and the researcher. The sampling rate of the device was approximately 150 Hz. The time required for measurement was approximately 2–4 seconds [19]. Relevant parameters in standing upright position (thoracic curvature angle [from T1 to T12], lumbar curvature angle [from T12 to S1], sacrum-hip angle [the difference between the sacral angle and the vertical], inclination angle [angle formed by the vertical and a line joining C7 to sacrum]) were recorded by the Spinal Mouse device via Bluetooth and were analyzed. Spinal Mouse assessments in sagittal axis have been shown to be reliable in children, and intrarater intraclass correlation coefficients (ICCs) ranged from 0.61 to 0.96 while the interrater ICCs ranged from 0.70 to 0.93 [18, 20–22].
Static and dynamic balance of the children was evaluated with the BBS device. The BBS is a circular platform designed to evaluate and record the ability of a person to maintain stability in quiet standing and under dynamic stress, when the platform surface tilts up to 20° in anterior/posterior or medial/lateral plane [23]. Platform stability can be changed with the unit at the bottom of the platform (from Level 12 [most stable] to Level 1 [least stable]). Before starting the evaluation, the BBS platform was locked and the children were asked to step onto the platform, stand quietly, and look straight ahead. The monitor of the device was adjusted to the child’s eye level according to the child’s height. The ideal foot positions of the children were determined and placed in the foot coordinates. Before starting the evaluation, the children were informed about the test and were trained for one minute for adaptation to the device [24]. During the evaluation, children were asked to maintain an upright standing position on the BBS platform. The Modified Clinical Test of Sensory Interaction and Balance (m-CTSIB) test was used to evaluate static balance. In the static balance assessment, the platform was locked. During this test, children were assessed in four different ways: eyes open on firm surface, eyes closed on firm surface, eyes open on foam surface, and eyes closed on foam surface. Each test’s duration was 30 seconds, with a 10-second rest period between tests. The “sway index” data generated for each child was analyzed. The Postural Stability Test was used for dynamic balance assessment; testing was initiated with the platform stability at Level 4 and progressed to Level 1. The test was repeated three times for 20 seconds; anterior-posterior stability index (APSI), medial-lateral stability index (MLSI), and overall stability index (OSI) were recorded. A mean score was calculated from the three trials. High values during dynamic and static balance evaluation are indicative of greater instability/balance [24, 25]. The BBS is a valid and reliable device and is an important balance assessment device in children[26, 27].
Physical and sociodemographic characteristics
Physical and sociodemographic characteristics
PMNE: Primary Monosymptomatic Nocturnal Enuresis. BMI: Body Mass Index. a: Variables are shown as Median (Interquartile range). b: Variables are shown as n (%).
Comparison of children’s symptom severity
PMNE: Primary Monosymptomatic Nocturnal Enuresis. Vancouver NLUTD/DES: Vancouver Non-Neurogenic Lower Urinary Tract Dysfunction/Dysfunctional Elimination Syndrome Questionnaire. a: Variables are shown as Median (Interquartile range). *p≤0.05.
Descriptive values (mean, standard deviation [SD], median value, number, and percentage frequencies) of the obtained data were analyzed. Relationships between categorical features and groups were examined using Pearson chi-square or Fisher-Freeman-Halton tests, depending on the number of subjects. Compliance of numerical properties to normal distribution was evaluated by the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare the two groups in terms of numerical properties. Statistical significance level was accepted as p < 0.05. SPSS (ver. 23) was used in calculations.
Results
No significant difference was found between the physical (age, height, weight, BMI, gender, etc.) and sociodemographic characteristics (family structure, type of delivery, gestational age, etc.) of the children with PMNE and the heathy control group in this study (Table 1). The NLUTD/DES questionnaire revealed a significant (p = 0.001) difference between the two groups, with the severity of symptoms greater in the PMNE group (Table 2). When the parameters of the bladder diary were compared, it was found that frequency of nocturia and NE in children with PMNE were significantly (p = 0.001) higher than in the healthy control group. Daytime urine frequency, average urine volume, and the amount of consumed fluid in one day were comparable between groups (Table 3). Bowel diary parameters revealed no significant difference between groups (Table 3). Upright standing alignment as assessed using the Spinal Mouse found that children with PMNE had significantly increased lumbar lordosis (p = 0.018) and sacral-hip angles (p = 0.029) compared to the healthy control group (Table 4). Static balance assessment revealed that the children with PMNE had significantly (p = 0.001) decreased static balance with eyes closed on the foam surface (p = 0.001) only. Dynamic balance assessment revealed children with PMNE had greater medial-lateral (ML) instability (p = 0.049) compared to the healthy control group, while other balance parameters were similar (Table 5).
Comparison of bladder and bowel diary parameters of children
Comparison of bladder and bowel diary parameters of children
PMNE: Primary Monosymptomatic Nocturnal Enuresis. a: Variables are shown as Median (Interquartile range). b: Variables are shown as n (%). *p≤0.05.
Comparison of children’s spinal postures
PMNE: Primary Monosymptomatic Nocturnal Enuresis. UP: Upright Position. a: Variables are shown as Median (Interquartile range). *p≤0.05.
Comparison of the static and dynamic balance of children
PMNE: Primary Monosymptomatic Nocturnal Enuresis. m– CTSIB: The Modified Clinical Test of Sensory Interaction and Balance. EOFiS = Eyes open firm surface. ECFiS = Eyes close firm surface. EOFoS = Eyes open foam surface. ECFoS = Eyes close foam surface. APSI = Anterior-posterior stability index. MLSI = Medial-lateral stability index. OSI = Overall stability index. a: Variables are shown as Median (Interquartile range). *p≤0.05.
In this study, it was found that children with PMNE had greater symptom severity, had increased lumbar lordosis and sacral-hip angles, were less stable in standing with eyes closed on foam surface, and had greater mediolateral dynamic instability when compared to healthy children.
The symptom severity of children with PMNE was worse than that of healthy children, as was the expected result. This finding substantiated that this study was representative of children with PMNE. A score of at least 11 on the Vancouver NLUTD/DES questionnaire indicates the presence of bladder and bowel dysfunction [16]. In this study, children with PMNE received an average score of 13 on the Vancouver NLUTD/DES questionnaire, while healthy children averaged a score of 5.5. In light of these results, it is shown that children with PMNE have bladder and bowel dysfunction symptoms and their symptom severity is worse than healthy children.
The comparison of spinal postures of children with PMNE and healthy children revealed that the lumbar lordosis and sacral angles of children with PMNE were increased. To the authors’ knowledge, there is only one study in the literature that evaluated standing posture of children with NE: Pereira et al. [14] compared the postures of 111 children (7–16 years of age) with NE and 60 healthy children, using retroflective anatomical land markers on the anterior superior iliac spine, the posterior superior iliac spine, the greater trochanter, and lateral malleolus and reported that children with NE had higher pelvic anteversion angles compared to healthy children. While the findings of this study were supportive of Pereira et al.’s findings, that study included all children with NE in monosymptomatic, non-monosymptomatic, primary, and secondary types. It is known that etiology of secondary enuresis includes mostly psychological problems [12]. NMNE, in addition to NE, includes lower urinary tract dysfunctions such as urgency, delayed voiding, and dysfunctional voiding, and also the etiology of each dysfunction is different [28]. Additionally, in the literature it has been reported that children with non-monosymptomatic and/or secondary NE have more psychological and behavioral problems than children with PMNE [29, 30]. The emotional state of the child may affect posture [31]; therefore, it is difficult to determine whether posture is affected by psychological problems or by NE. In this study, to ensure homogeneity among children with NE, children who did not have a history of being dry for six months and who had only NE were included. This method ensured that the posture of a group with a more specific and homogeneous etiology was evaluated. Therefore, to the authors’ knowledge, this is the first study evaluating the posture of children with PMNE in the literature. Pereira et al. [14] evaluated the postures of children with NE using the photogrammetry technique most often used in the literature. In this study, the spinal postures of the children were assessed with a more recent and objectively-proven Spinal Mouse device. In addition to being a popular assessment tool used in spinal posture assessment, the Spinal Mouse has been shown to be reliable for various age groups, especially in recent years [20, 33].
In this study, static and dynamic balances of children with PMNE and healthy children were evaluated. Examination of the sensory integration of static balance control revealed that the static balance of children with PMNE was most impaired when visual input was removed and proprioceptive input decreased (on foam surface with eyes closed). In a previous investigation, Pereira et al. [14] assessed the sensory integration of balance in children with NE and healthy controls using the same paradigm. Children were divided by age (7–11 years and 12–16 years) to allow for control of maturational influences. Children with NE demonstrated decreased stability in all sensory conditions excluding the unstable surface with eyes open for those 12–16 years of age [14]. The differences between this study’s findings and Pereira et al.’s [14] study may reveal differences in the maturation of postural control of children with PMNE versus NE; however, further investigation is needed to substantiate this.
The elimination of vision significantly affects balance and is compensated for by the proprioceptive and vestibular systems [34]. Structures responsible for balance control mature in different stages of childhood. Among the sensory systems, the visual system completes its development first, reaches maximum importance around the age of six, and plays a dominant role in postural control. Then, the somatosensory system development is completed. Children gain the ability to correctly interpret inputs from the visual and somatosensory systems around the age of seven. The ability to interpret inputs from the vestibular system are acquired last. Thus, the functional development of the structures responsible for balance control is completed around the age of nine [35, 36]. In this study, the average ages of children with PMNE and healthy children were similar (nine years). Children with PMNE were found to perform worse than healthy children in the eyes closed foam surface condition, which indicated that the integration of vestibular and somatosensory input was compromised. In this study, it was predicted that maturational delay, which is one of the etiologies of NE, would also impact the development of balance control strategies and result in children with PMNE demonstrating visual dependence for balance control longer than healthy children.
In the evaluation of dynamic balance of children with PMNE and healthy children, it was found that children with PMNE demonstrated ML instability relative to healthy control children. Studies on dynamic balance generally investigate stability in the anterior-posterior (AP) direction. Postural oscillations used in daily life are often in the AP direction. There is very little movement in the ML direction in the ankle and knee. There are some differences in maintaining the balance in AP and ML directions. While the ankle is used primarily to maintain postural control in the AP direction, the hip joint and trunk are mostly used to provide postural control in the ML direction. For example, during the single-stance phase of the execution of the first step, center of mass displaces ML direction, and taking a voluntary step is achieved by the preparatory postural adaptation in the ML direction [10, 37]. In the study by Henry et al. [38] examining the responses of standing children on platforms with perturbations in 12 different directions, it was reported that the muscles that responded best to perturbations in the ML direction were the rectus femoris and tensor fasciae latae. Hong et al. [39] reported that stability in the AP direction developed earlier than stability in the ML direction, as the ability to walk was acquired at an early age. In this study, although the mean age of the two groups was similar, it was found that the stability of children with PMNE was worse in the ML direction, possibly due to delay in the development of proximal muscular strength and postural control strategies about the hip.
A limitation of this study was the use of a four-day bladder diary. In the literature, a seven-day bladder diary has been recommended to evaluate the urinary parameters of NE [1]. Although the aim at the beginning of this study was that the children would complete a seven-day bladder diary, the children and their families reported that they could not follow the bladder diaries regularly and provided incomplete diaries; thus, only a four-day bladder diary was obtained [40]. Another limitation of this study was the evaluation of posture and balance in children of a wide age range (6–18 years). There are many components that affect postural stability, such as muscle strength, coordination, and cognitive status [41]. In future studies, posture and balance assessments can be strengthened by dividing them into age ranges.
In conclusion, delayed maturation of bowel/bladder control is seen in association with poor posture and delayed development of static and dynamic balance strategies in children with PMNE in comparison to healthy children. This study of children with PMNE is among the pioneering studies in this field, and the findings suggest balance and posture exercises may be a beneficial therapeutic intervention for children with NE. Future studies are needed to elucidate the impact of CNS maturational delay in children with NE and promote the development of evidence-based intervention strategies.
Footnotes
Acknowledgments
The authors are grateful to all participating children and their families.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding
This research was supported by Bolu Abant İzzet Baysal University Scientific Research Projects Unit with the project number 2018.14.01.1270.