
Abstract
Objective:
To investigate the prevalence and the related characteristics of oligomenorrhea among women within childbearing age in China.
Study design:
A large-scale community-based investigation was conducted from 2013 to 2015. A total of 12,964 women aged 18–49 years from 9 provinces/municipalities in China were recruited for healthcare screening in local community health centers. Outcome measures include clinical history, ultrasonographic exam, and hormonal and metabolic parameters.
Results:
Among women within childbearing age in China, the prevalence of oligomenorrhea was 12.2% (1,579/12,964). Both sociodemographic factors and medical history were significantly associated with oligomenorrhea (P < 0.05). In such women, the prevalence of obesity, acne, seborrhea, acanthosis, larger ovarian size, and polycystic ovarian morphology was higher when compared with normal women; the prevalence of anti-Mullerian hormone, total testosterone, and androstenedione (P < 0.05) was higher as well. The infertility rates of all women were higher in the oligomenorrhea group (17.2%, 272⁄1,579) than in the non-oligomenorrhea group (9.0%, 1,024⁄11,385), and among women without contraception, for the oligomenorrhea group, the infertility rate was 32.5% (128⁄394), and for the non-oligomenorrhea group, 17.9% (400⁄2,240). In the oligomenorrhea group, 57.4% (156/272) of the women underwent treatments for infertility, which was higher than the non-oligomenorrhea group 36.1% (370/1,024).
Conclusions:
Obesity, acne, seborrhea, acanthosis, larger ovarian size, and polycystic ovarian morphology were significantly associated with oligomenorrhea. The increase of anti-Mullerian hormone, total testosterone, and androstenedione level was also demonstrated in the oligomenorrhea group. Higher prevalence of infertility and medical treatment rate was observed in women with oligomenorrhea.
Introduction
Menstrual cycle disorders are a type of physiological disease which can affect pregnancy in women of reproductive age. Oligomenorrhea is one of the most common types of menstrual bleeding disorders, and an increasing number of patients have sought medical help for this symptom in recent decades. Women with oligomenorrhea have menstruation intervals of more than 35 days and less than 90 days 1 or a total of 5–7 cycles a year. 2 . The prevalence of oligomenorrhea has increased considerably in recent decades, ranging from 12% to 15.3% according to different studies worldwide, 3 with 10%–20% occurring in infertile women. 4 Therefore, diagnosis and treatment of menstrual disorders are of utmost importance.5,6
Menstrual cycle disorders are commonly caused by endocrine disorders like polycystic ovary syndrome (PCOS), 7 thyroid dysfunction, premature ovarian failure, hypothalamic dysfunction, and prolactinomas. 8 Especially, patients with PCOS have reported symptoms of irregular ovulation, 9 and an estimated 75%–85% of them have oligomenorrhea. 10
Hypothalamus–pituitary–ovary axis dysfunctions are the main cause of oligomenorrhea, which could be affected by numerous factors. 11 Moreover, oligomenorrhea can lead to a number of gynecological diseases, such as infertility, hirsutism, and acne vulgaris. 12
After the lifting of the one-child policy gradually in recent years, 13 women with monthly cycle disorders required more reproductive medicines. Since the prevalence of oligomenorrhea and the characteristics of women with oligomenorrhea have never been analyzed in China, a large community-based investigation was conducted among women of childbearing age, which could provide practical guidance and support for these patients.
Materials and methods
Subjects
This cross-sectional epidemiological study was carried out from 2013 to 2015 in China. Study participants were geographically distributed over northeast, north, east, central south, northwest, and southwest areas of China, including Beijing, Zhejiang, Hebei, Anhui, Shaanxi, Tianjin, Hunan, Guizhou, and Henan. We used a multilayer-stratified strategy, with a rural-to-urban ratio of 1:1; full details were similar to the previous reports.14,15 Sample size calculation formula is as follows:
Three stratums were district, province/municipality, town/township, and village/street, and a multistage-stratified cluster sampling strategy was used. First, the districts were categorized into two strata representing high and low prevalence of oligomenorrhea, and then two provinces/municipalities were randomly chosen from each stratum. Based on the number of women of childbearing age, the province/municipality was divided into nine strata in order, and three townships from the highest, moderate, and lowest stratum were chosen randomly. In the selected townships, every village/street was investigated as a unit, and participants aged 18–49 years were recrewed.
This study had all participants sign informed consent and had approval from the relevant ethics committees. Married or cohabitating women, aged between 18 and 49 years, who signed informed consent were included. Postmenopausal and pregnant/breastfeeding women at the time of the investigation were excluded.
Operational definitions and data collection
Women with oligomenorrhea have menstruation intervals of more than 35 days. Infertility is the failure to achieve clinical pregnancy after 1 year or more of unprotected sexual intercourse, despite having a desire to get pregnant. All participants’ data were gathered through questionnaires completed by specialized investigators after a face-to-face interview in the study. Standardized and structured questionnaire was developed before the investigation. The investigators from each hospital were fully trained to standardize the finishing questionnaire and physical examination, with monitoring from prime investigators or on-site supervisors. The questionnaire variables included demographics and socioeconomic factors (age, education, occupation, and income), duration of marriage or cohabitation, menstrual cycle characteristics, contraceptive use, reproductive history, medical history, and family history.
Study protocol
All the participants finished the questionnaire and then underwent physical examination to assess their blood pressure, body mass index (BMI), waist-to-hip ratio (WHR), breast, thyroid, hair distribution, and presence of acne and/or premature alopecia and bimanual pelvic examination and transvaginal ultrasound scan to determine any possible uterine and/or ovarian issues. Polycystic ovarian morphology (PCOM) is defined by ovarian volume (>10 cm3) and/or increased antral follicle count (AFC ⩾12 in 1 ovary) on ultrasonographic examination. Then, 8.84% (1,146/12,964) of the participants were randomly selected to provide blood samples on the 2nd to 4th day of menstruation for determination of hormone indicators like follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), anti-Mullerian hormone (AMH), prolactin (PRL), testosterone (T), thyrotropin (TSH), and other fertility predictors.
Statistical analysis
Data were recorded in EpiData 3.0 (EpiData Association, Odense, Denmark) and analyzed by SPSS 22.0 (SPSS, Inc., Chicago, IL, USA). The Pearson’s chi-square (χ2) test was used to compare the categorical variables. Continuous variables were presented as the mean ± SD after checking for normality and were compared using Student’s t-test or Mann–Whitney U-test or one-way ANOVA for distributions, as was appropriate. Pearson correlation coefficients and the two-tailed method were used to evaluate correlations between variables. Statistical significance was considered if P < 0.05.
Results
Prevalence of oligomenorrhea in the Chinese community population
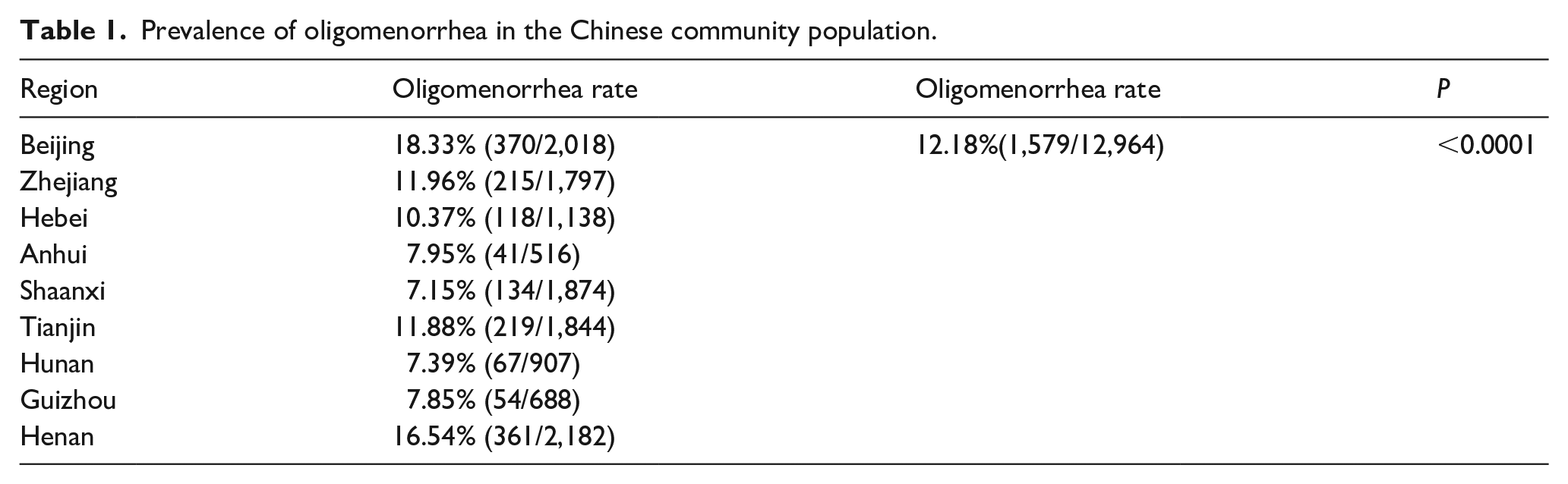
A total of 12,964 participants were selected and invited to participate in this study, of which 1,579 women were diagnosed as having oligomenorrhea. Overall, this large community sample study revealed that the prevalence of oligomenorrhea among Chinese women of childbearing age was 12.18% (1,579/12,964) (Table 1), and the age-standardized prevalence was 12.46% (Table S1). Beijing, Henan, and Zhejiang were the top three areas with high oligomenorrhea rates (Table 1).
Prevalence of oligomenorrhea in the Chinese community population.
The characteristics of Chinese women with and without oligomenorrhea
Results showed that in 1,146 women who completed the questionnaire, physical examination, transvaginal ultrasound, and blood tests, the mean age of women with oligomenorrhea was 35.75 ± 8.27 years (i.e. younger than women without oligomenorrhea, 37.12 ± 7.95 years) (P < 0.001, Table 2). In addition, women with oligomenorrhea were well-educated, living in high-stress situations, working overtime, working in air-conditioned or ill-ventilated room, and had preference for unhealthy food (P < 0.05, Table 3).
The characteristics of women with oligomenorrhea and non-oligomenorrhea.

SD: Standard Deviation; BMI: Body Mass Index; TT: total testosterone; AMH: anti-Mullerian hormone; A: androstenedione.
Distributions were compared using Student’s t-test or Mann–Whitney U-test or one-way ANOVA.
The characteristics of Chinese women with and without oligomenorrhea.

Categorical variables were compared using Pearson’s chi-square (χ2) test.
The medical history, physical examination, and lab results of women with and without oligomenorrhea
Compared with women without oligomenorrhea, women with oligomenorrhea had higher rates of abnormal menstruation duration and had lower chance of gravidity and parity (P < 0.01, Table 4). The medical history of the participants revealed higher prevalence of obesity, gestational diabetes mellitus, ovarian hypofunction, diabetes mellitus, and family history of oligomenorrhea or infertility (P < 0.001, Table 4). In women with oligomenorrhea, physical examination results revealed higher rates BMI, acne, seborrhea, acanthosis, larger ovarian size, and PCOM, whereas laboratory results showed higher AMH, TT, and A levels (P < 0.05, Tables 2 and 4).
The medical history and physical examination of women with and without oligomenorrhea.
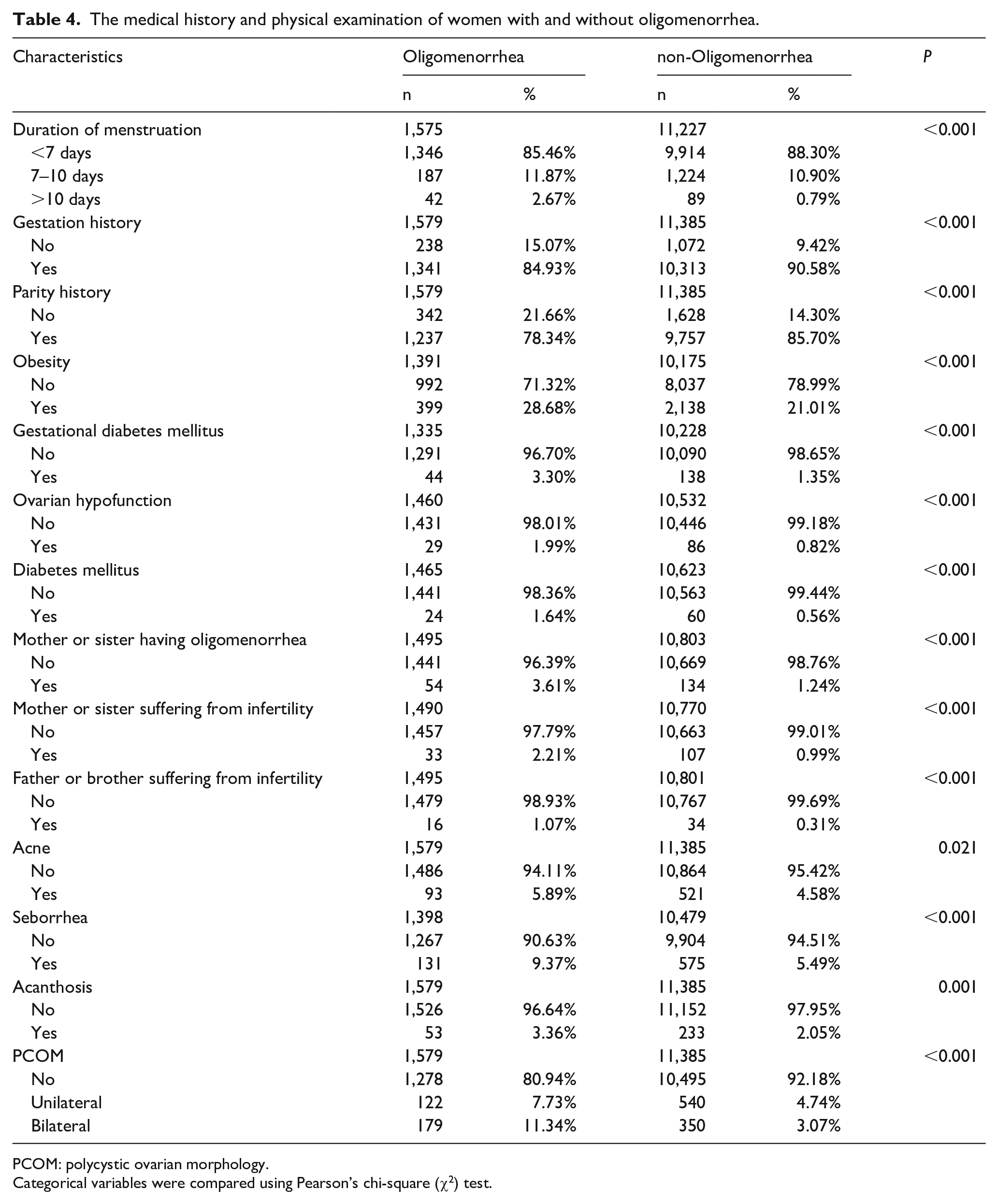
PCOM: polycystic ovarian morphology.
Categorical variables were compared using Pearson’s chi-square (χ2) test.
The infertility rate and treatment-seeking behavior in women with oligomenorrhea
The infertility rate was higher in the oligomenorrhea group (17.23%, 272/1,579) than in the non-oligomenorrhea group (8.99%, 1,024/11,385). The same trend was observed among women without contraception: oligomenorrhea group, 32.49% (128/394); non-oligomenorrhea group: 17.86% (400/2,240) (Table 5). In addition, the infertility rate increased with the length of the monthly cycle (Table 6). There were significant differences in the treatment-seeking behavior between the two groups: in the oligomenorrhea group, 57.35% (156/272) of the women underwent treatments for infertility, which was higher than in the non-oligomenorrhea group (36.13%, 370/1,024). Furthermore, 46.79% (73/156) of the women in the oligomenorrhea group knew the reasons for infertility, with ovulatory dysfunction being the reason in most of the cases (75.34%, 55/73), whereas 47.30% (175/370) of the women in the non-oligomenorrhea group knew the reasons for the infertility, with male factor being the reason in most of the cases (32.00%, 56/175) (Table 5). Among the women who sought treatment for infertility, 51.28% (80/156) had ovulation induction in the oligomenorrhea group, which was higher than the rate of the non-oligomenorrhea group (27.84%, 103/370). In addition, 46.15% (72/156) of the women in the oligomenorrhea group took Chinese herbal medicine, which was lower than in the non-oligomenorrhea group (52.97%, 196/379) (Table 5).
The infertility rate and treatment-seeking behavior between women with and without oligomenorrhea.
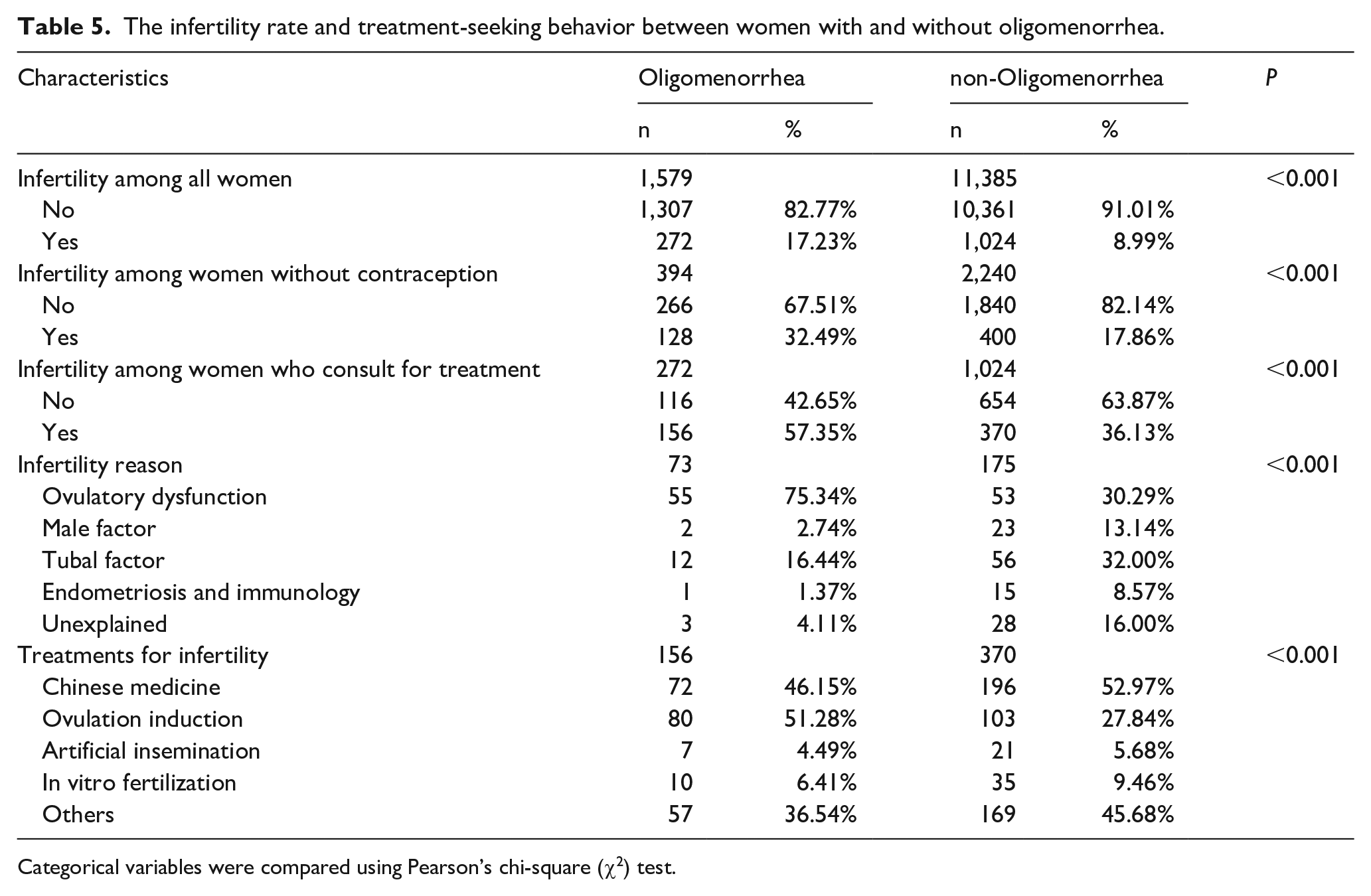
Categorical variables were compared using Pearson’s chi-square (χ2) test.
Infertility rate among women with and without contraception.

P < 0.05 has a significant difference.
Comments
In this study, the prevalence of oligomenorrhea among Chinese women of childbearing age was 12.18% (1,579/12,964). The results of this study also demonstrated the different characteristics between women with and without oligomenorrhea. Our findings underscored that regularity of women’s menstrual cycles was an important potential indicator of infertility, which also influenced their treatment-seeking behaviors. To the best of our knowledge, this is the first study that has investigated the characteristics and association of oligomenorrhea and infertility in a large, well-defined, community-based study of Chinese women.
Our research demonstrates that oligomenorrhea is more common to younger women and in those with larger ovarian size and PCOM. As is known, the follicle number decreases with age, and PCOM is a common age-dependent phenomenon. Johnstone et al. 16 reported a 32% prevalence of PCOM among ovulatory women, with 62% occurring in 25- to 30-year-old women and 7% in the 41- to 45-year-old women. In addition, the ovarian volume measured by transvaginal sonography, which reflects the number of the remaining primordial follicles, also illustrated the phenomenon of ovarian reserve declination with aging. 17 Pavlik et al. 18 demonstrated a stable ovarian volume up to the age of 35 years, which rapidly declines in the ages of 35 and 55 years.
Our research demonstrated that women with oligomenorrhea had higher levels of serum AMH, TT, and A. Furthermore, acne, seborrhea, and acanthosis were more common in women with oligomenorrhea, which was consistent with the findings of previous studies. 19 Eldar-Geva et al. 20 showed that serum AMH levels, prevalence of acne and hirsutism, the mF-G score, 21 and serum dehydroepiandrosterone sulfate (DHEAS) levels decreased with advanced age and that AMH increase was associated with hyperandrogenism. They reported that AMH oversecretion in women with hypothalamic–pituitary dysfunction was induced by the increasing frequency of the GnRH pulse of the hypothalamus, which inhibited follicular growth. Piouka et al. 22 indicated that all serum androgen markers were significantly negatively correlated with age and that oligomenorrhea or amenorrhea occurred more frequently in women with hyperandrogenism than among patients with PCOS.
According to a report, hyperandrogenemia and oligomenorrhea conferred detrimental metabolic risk for metabolic syndrome. 23 . We found that compared with women with regular cycles, more women with oligomenorrhea had medical history of obesity, gestational diabetes mellitus, and higher BMI in the physical examination. Women with irregular menstrual cycles had higher triglyceride levels, higher prevalence of dyslipidemia, type 2 diabetes mellitus, and chronic vascular diseases, 24 thus disrupting follicle genesis.
Consistent with the results of previous studies, 25 our study illustrated that women with oligomenorrhea had higher prevalence of family history of oligomenorrhea and were exposed to stressful environments. Palmfischbacher and Ehlert and other researchers26,27 suggested that women with greater dispositional resilience in the face of low to moderate chronic stress had reduced risk of irregular menstrual cycles. The alterations in hormonal patterns were possibly the underlying mechanisms of lifestyle factors influencing menstrual function. Attarchi et al. 28 indicated that various endocrine profiles were affected, especially estrogen and gonadotropin reduction and corticotropin release activation, which could cause menstrual dysfunction, thus affecting the occurrence and timing of ovulation and growth of the endometrial lining. 29
The results of our study revealed that women with oligomenorrhea had higher prevalence of infertility, which was consistent with the findings of previous studies. 30 This condition has various underlying causes, 31 but our results revealed that anovulation was the prime factor for infertility among women with oligomenorrhea. Furthermore, our results revealed that infertile patients with oligomenorrhea were more likely to choose ovulation induction, which targets anovulation for these oligomenorrhea patients and solves the problem in a short period of time. In addition, infertile women in the non-oligomenorrhea group were more likely to take Chinese herbal medicine because these patients have various underlying causes for infertility, and herbal medicine could be a good choice to assist. Several studies provided evidence that herbal medicines might have beneficial effects on women with oligomenorrhea, hyperandrogenism, and PCOS. 32 Optional treatment like pulsatile gonadotrophin-releasing hormone therapy or clomiphene citrate could be considered appropriate medical treatment. 33 Other attractive treatment option of PCOS like inositols, an insulin second messenger, 34 was found involving in follicular gonadotropin pathways which orchestrate ovulation. 3 . It could be beneficial to some women with oligomenorrhea in improving metabolic and hormonal state and restoring spontaneous ovulation.
The strength of the study was the large-scale investigation aimed at all women of childbearing age, focusing on the prevalence of oligomenorrhea in the general population in order to provide evidence for the improvement and guidance of investigation and clinical medicine. Compared with other studies which recruited participants from the hospital or clinics, which might over-estimate the risk of disease, we eliminated the potential selection bias. In addition, this study randomly selected 1,146 participants, from whom blood samples were collected for valuable hormone level analysis. However, there were also several limitations of this study. Among women with oligomenorrhea with PCOS, particularly the ones with high AMH, it does not seem adequate to access the ovarian reserve. 35 In addition, AMH varies for different ages, so the set of year-by-year age-specific reference ranges of serum AMH levels in Chinese women could be a good reference. 36 The participants need to undergo transvaginal ultrasound in our study, so women who were virgins were not included in our study.
In conclusion, the results of our study indicated that the prevalence of oligomenorrhea in Chinese women of childbearing age was 12.18%, whereas age, sociodemographic features, medical history, specific physical examination, and laboratory results were significantly associated with oligomenorrhea. A higher prevalence of infertility was observed, and the characteristics of treatment-seeking behavior were also revealed in our study. Further studies about symptoms changing with advancing age in various types of oligomenorrhea are recommended. In addition, the effectiveness of various treatments needs to be compared in relation to the different pathogeneses of oligomenorrhea. This study would contribute to the field to improve patients’ health and provide policy implications.
Footnotes
Authors’ note
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. Publishing consent was obtained from all participants. The authors have none to declare.
Author contributions
R.L. obtained data from the Funding program and gave a critical review and comments during the preparation of this manuscript. Y.L.H. and D.N.Z participated in interpretation of data, analysis, and drafting the manuscript. J.Q. assisted with reviewing and revising the manuscript. W.S., X.H.W., S.Y.Z., Z.L.W., X.R.S, X.B.S., Y.M.Z, and S.Y.W. participated in the investigations and collected the data. All authors approved the manuscript as submitted and take full responsibility for the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The investigation was supported by National Key Technology R&D Program in the Twelves Five-Year Plan (2012BAI32B01), National Key Research and Development Program of China (2016YFC1000201), and National Natural Science Foundation of China (81771650, 81471427).
Informed consent
All participants in this cross-section epidemiological study signed the informed consent. The study was approved by the Ethics Committee of each hospital and the National Center for Chronic and Noncomunicable Disease Control and Prevention (NCNCD).