
Abstract
PURPOSE:
The aim of this study was to examine the relationship between gait analysis measures associated with crouch gait, functional health status and daily activity in ambulant cerebral palsy (CP).
METHODS:
Three-dimensional gait analysis was carried out on 35 ambulant participants with
bilateral CP crouch gait (knee flexion at mid-stance (KFMS)
RESULTS:
There were no significant correlations between KFMS and PODCI domains
(
CONCLUSIONS:
Step length and gait speed are more strongly associated with functional health status and daily activity than knee flexion during stance in children and adolescents with CP crouch gait.
Introduction
Cerebral palsy (CP) is the most common cause of motor impairment in children [1]. The associated muscle tightness, weakness and impaired motor control often lead to difficulties during gait. There are numerous gait presentations associated with CP; however, crouch gait, defined as excessive knee flexion in stance phase, is one of the most common pathological patterns associated with bilateral CP [2]. This flexed knee posture during gait has been shown to increase the forces and demands on the knee joint [3, 4] and can potentially lead to joint degeneration and pain [5]. For these reasons, the correction of excessive knee flexion during gait is a significant focus of surgical intervention in those with CP. A number of surgical techniques have been shown to improve knee kinematics in crouch gait [6, 7, 8, 9]. It is recognised that the assessment of surgical outcomes should include outcome measures based on the International Classification of Functioning, Disability and Health (ICF) [10]. The impact of knee crouch, and its treatment on these domains is less clear. A recent long-term follow-up study by Boyer et al. [9] found that while distal femoral extension osteotomy (DFEO) and patellar tendon advancement (PTA) led to superior outcomes in terms of improving knee extension compared to alternative surgical intervention. This did not translate into better outcomes in terms of non-gait function, activity, participation, quality of life or knee pain.
The Pediatric Outcomes Data Collection Instrument (PODCI) is a measure of functional health status which has been found to be valid and reliable in children and adolescents with CP [11, 12]. The PODCI questionnaire yields scores in six domains: upper extremity function, transfers and basic mobility, sports and physical function, pain/comfort, happiness with physical condition and a global function score. A number of studies have reported improvement in the functional PODCI domains (sports and physical function, transfers and basic mobility and global function) following orthopaedic surgery in children with CP but no changes in the psycho-social domains (pain/comfort and happiness with physical condition) [13, 14, 15]. As none of these studies [13, 14, 15] reported on gait kinematics, it is not possible to ascertain if the reported post-operative improvements in PODCI domains were associated with improvement in specific gait kinematic variables post-operatively. In contrast, Stout 2008 [16] compared short-term outcomes in groups who had DFEO-only, DFEO+PTA and PTA-only and found that while stance-phase knee flexion was restored to normal range in the DFEO+PTA and PTA-only groups, none of the three groups demonstrated significant improvement in the transfers and basic mobility, sports and physical function or pain/comfort domains of the PODCI assessment. Thus, is appears that while orthopaedic intervention can potentially lead to improvements in the functional domains of the PODCI assessment. They do not seem to be related to changes in stance phase knee flexion.
Ambulatory children with CP have been shown to have significantly reduced levels
of walking activity compared to typically developing peers [17]. On examining the relationship between gait kinematics and
daily activity, Wilson et al. [18] found a
moderate correlation (
The aim of this study was to examine the relationship between gait parameters
related to knee crouch gait, functional health status and daily activity levels in children
and adolescents (
Method
Participants
The local host institution research ethics committee granted ethical
approval for this study. Potential study participants were identified both prospectively
and retrospectively. Participants were recruited prospectively from those being seen for
routine clinical gait analysis between December 2014 and February 2017. The gait
laboratory database was also used retrospectively to identify participants who met the
inclusion criteria up to two years prior to December 2014. Willing participants were
subsequently invited back to the laboratory for a research-only assessment. Inclusion
criteria were a diagnosis of bilateral cerebral palsy GMFCS level I–III, age 4 to 17 years
at the time of analysis and crouch gait. Crouch was defined as knee flexion greater or
equal to two standard deviations above normal at mid-stance phase in at least one
limb [20]. Based on a review of our laboratory
database, this equated to a mid-stance knee flexion value of greater or equal to
19
Data collection and analysis
Three-dimensional kinematic and kinetic data were captured using a
four-camera Codamotion cx1 active marker system (Charnwood Dynamics, Leicestershire, UK).
Kinematic data were sampled at a rate of 200 Hz while ground reaction forces were captured
using two Kistler force plates at a sampling rate of 400 Hz. Infrared markers were placed
on each participant’s lower limbs as per a modified Helen Hayes protocol [21]. All participants walked barefoot at a
self-selected speed. Participants walked independently where possible. For those who
routinely used a walking aid (
Functional health status was assessed using the Pediatric Outcomes Data Collection Instrument (PODCI). The scores most relevant to gait and lower limb function were analysed in this study, namely: Transfers and Basic Mobility, Sports and Physical Function, Pain/Comfort, Happiness with Physical Condition and Global Function. Parents completed the questionnaire for all participants aged 10 years and under (Pediatric version). Older participants completed the questionnaire themselves where possible or with parent/guardian assistance when needed (Adolescent Self-Reported version). Questionnaires were completed by participants/parents at home in the days following gait analysis. The majority of questions in the PODCI questionnaire are scored using a 1–5 range with 1 indicating the most positive response. The scores for all individual questions comprising a scale are averaged and the mean of the rescaled values is then multiplied by a constant so that each scale has a final range of values between 0–100 [24].
Daily activity levels were assessed using an activPAL (PAL Technologies, Glasgow, UK) uni-axial accelerometer-based activity monitor, which has shown evidence of criterion validity in children, adolescents and young adults with CP [25, 26, 27]. Manufacturer’s recommendations for securing the thigh-mounted device were followed and wearing of the thigh mounted activity monitor was demonstrated to participants and parents/guardians. Participants were asked to remove the device only for night-time and for water-based activities [26]. A simple diary of physical activity was completed by each participant (or guardian) to both confirm appropriate wear time and provide an aid to interpretation of the output. Sedentary time (time sitting/lying) and the number of strides taken were determined. It was determined by the accelerometer based on limb position [25]. The monitor was worn for five consecutive days and the average of three days was used for analysis which has been shown to achieve a reliability coefficient of 0.70 in children with and without CP [28]. It has previously been shown that children with CP take more steps on school days compared to weekend days [29]. Therefore, in the current study, the mean of two weekdays and one weekend day was analysed to account for this difference and to best capture overall activity levels. School term time versus school holidays as well as seasonal variations in weather might also be expected to impact on daily activity levels [30, 31]. Therefore, while the time of year of the assessment (school term or summer) was not controlled in this study, the season (spring, summer, fall, winter) was included in the correlation analysis.
Participant (
35) demographic, gait, quality of life and daily
activity data
Participant (
Data are mean
Shapiro-Wilks test of normality was conducted on all continuous variables
and collinearity was assessed using variance inflation factors (VIF). For the purpose of
statistical analysis, the averaged and rescaled PODCI scores (ranging 0–100) were treated
as continuous variables. Parameters were considered non-collinear for VIF
Results
A total of 35 participants met the inclusion criteria for this study. All had
knee flexion greater or equal to 19
Sports and physical function, sedentary time/day, mean steps/day, knee flexion
at initial contact and age were normally distributed. Transfers and basic mobility,
pain/comfort, happiness with physical condition, global Function, knee flexion at
mid-stance, Normalised speed and normalised step length were not normally distributed
(
The relevant correlation coefficients between gait, PODCI and daily activity variables and associated p-values are summarised in Figs 1 and 2. Analysis of variance inflation factors demonstrated no collinearity between any of the included parameters; values ranged from 1.18 to 5.82.
Correlations between PODCI domains and gait parameters. r- Pearson’s correlation
coefficient. 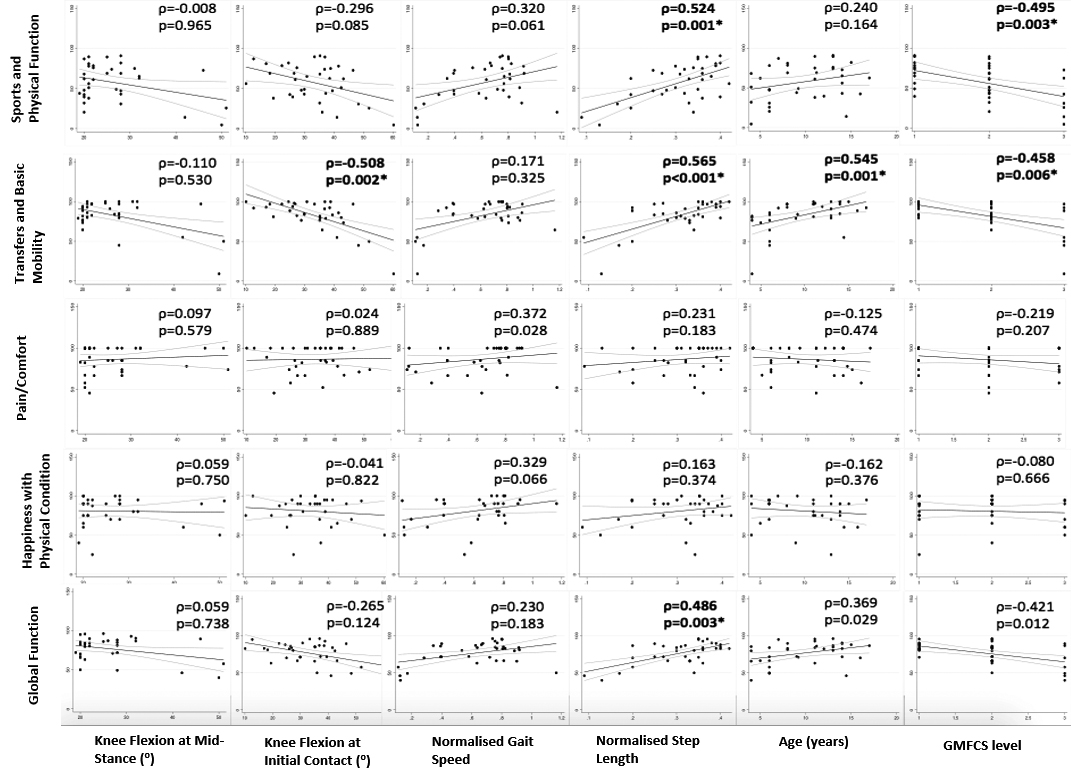
Correlations between ActivPal measures of daily activity and gait parameters. r-
Pearson’s correlation coefficient. 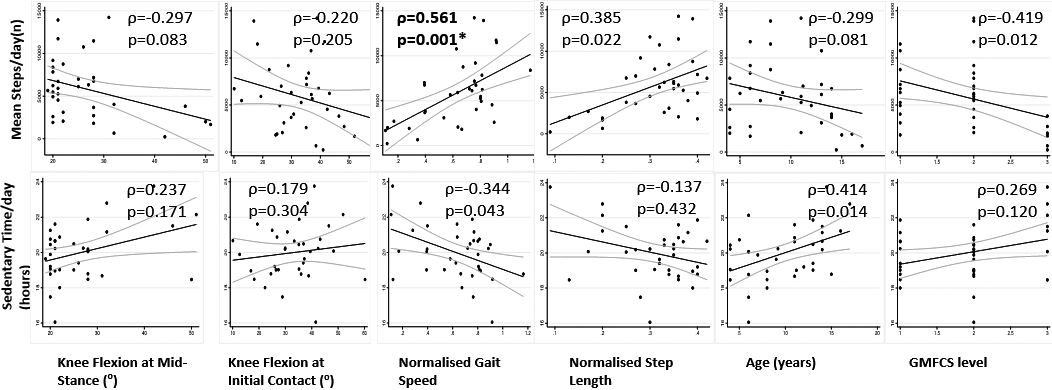
There were no significant correlations (Bonferroni adjusted
Multivariable linear regression analyses of functional health status and daily activity measures
PODCI – Pediatric Outcomes Data Collection Instrument; GMFCS – Gross Motor Function
Classification System.
The separate multivariable linear regression analyses are summarised in Table 2. The analysis found that normalised step-length was independently associated with three PODCI domains (sports and physical function, transfers and basic mobility and global function). Normalised gait speed was significantly associated with steps/day.
Correlations between ActivPal measures of daily activity and PODCI domains. r-
Pearson’s correlation coefficient. 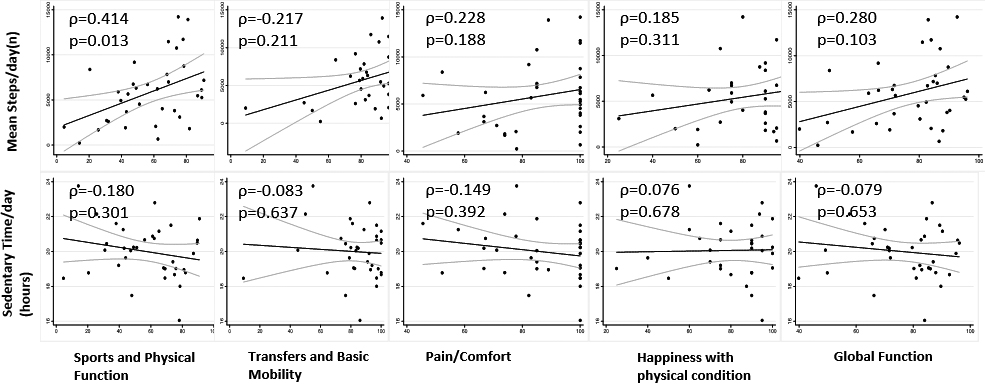
Correlation coefficients between PODCI and daily activity variables and
associated
As crouch gait has been shown to increase the forces and demands on the knee joint [3, 4], our hypothesis was that, as a result, those with more severe crouch would have lower measures of functional health status and reduced daily activity levels. However, our analysis demonstrates that there was no correlation between knee flexion angle at mid-stance and any of the PODCI domains or daily activity measures analysed.
Instead, the current results suggest that step-length is better associated with functional health status rather than the more specific kinematic angle of knee flexion during stance. While knee flexion contributes to step-length, it has also been suggested that factors such as selective motor control also influence step-length [33]. Normalised step-length was found to be independently associated with the three functional PODCI domains (sports and physical function, transfers and basic mobility and global function). Knee flexion in stance was not related to functional health status or daily activity levels. It is consistent with the findings of Steele et al. [34] who recently reported that knee flexion in stance also demonstrated poor correlation with energy expenditure of gait. These authors further noted that oxygen consumption during gait better correlated with knee flexion angle at initial contact which the authors hypothesised may in turn lead to shorter step lengths. The fact that step-length is better associated with functional health status potentially has important implications in treatment planning in children with CP crouch gait. While gait analysis has proven its effectiveness and usefulness in surgical planning in those with CP [35, 36, 37, 38], the current study suggests that surgical interventions targeted at improving specific gait kinematics may not directly influence activity and participation. While correlation does not imply causation, our results suggest that to best improve functional health status, step-length should be considered. This possibly re-enforces the importance of appropriate orthoses where indicated as Ankle Foot Orthoses (AFOs) have been shown to improve spatiotemporal parameters such as speed and step length in addition to the beneficial effects of surgery [39, 40]. The current results suggest that further research is warranted about a potential relationship between improvements in the spatiotemporal parameters of gait with AFOs and potential changes in functional health status.
In terms of daily activity, we found moderate correlations between mean steps/day and both normalised gait speed and sports and physical function. It is probably not surprising that the more functional walkers in terms of speed were also the most active. There was no association between daily activity and any of the specific kinematic values, which differs somewhat from the findings of both Wilson et al. [18] and Nicholson et al. [19]. They both report a moderate correlation between step/stride count and an overall gait kinematic summary score (GDI). This may suggest that kinematic values other than those examined in this study have more of an influence on step counts and daily activity.
There are a number of limitations that should be considered when interpreting
the results of this study. Our population size of 35 potentially limits the wider
interpretation of the results. However, the sample size is broadly in line with, or larger
than, similar studies on participants with CP [23,
41] and in all our regression analyses, the
number of fitted variables is less than one-tenth of the number of observations as
recommended [42]. This study specifically
examined children and adolescents with ambulant bilateral CP and therefore, the
generalizability of the results to older, more involved participants is somewhat limited.
The majority of participants in this study were GMFCS I and II and only a limited number of
GMFCS III participants were included as might be expected in a study of participants with
ambulant CP. Accordingly, Fig. 1
highlights that the knee flexion at mid-stance values are somewhat skewed to the left with a
smaller number of participants in more severe crouch greater than
40
The gait kinematics analysed in this study were collected barefoot as per routine clinical analysis protocols and therefore may not fully reflect community ambulation in this population. As highlighted above, the spatiotemporal parameters of gait would be expected to improve with orthoses [39, 40]. Therefore, future work is warranted to examine step length during community-based assessment to examine their impact on daily activity and functional health status. Additionally, routine walking aids were not used during gait data collection and the five participants who routinely used a walking aid (3 posterior walker, 2 bilateral crutches) were instead assessed with hand-held assistance. Krautwurst et al. [46] have highlighted that gait data collected without a walking aid is likely to be more flexed than gait with routine walking aid. While the hand-held support provided may have mitigated this to some degree, it is still likely that gait data as assessed in the clinical gait laboratory is likely to have differed somewhat compared to routine day to day walking.
A control group, not walking in crouch, might have potentially strengthened the findings and theoretically, as functional PODCI domains and daily activity levels do not appear to be related to knee flexion, the non-crouch group would have demonstrated similar functional health status and daily activity levels. However, as crouch gait has been suggested to progress with age in children with CP [44], a non-crouch control group would potentially be younger which in turn influences both PODCI scores and daily activity levels [12, 29].
Conclusion
The results of this study confirm that functional gait variables are associated with the functional domains of the PODCI assessment (sports and physical function, transfers and basic mobility and global function), although not the psycho-social domains (pain/comfort and happiness with physical condition). Analysis of specific gait parameters suggest that it is step length rather than knee flexion in stance which is best associated with functional health status in children/adolescents with CP crouch gait. This highlights the importance of considering spatiotemporal measures of gait when assessing walking function in CP and examining the potential impact of footwear and orthoses on these parameters.
Footnotes
Acknowledgments
The lead author is a research fellow funded by the Health Research Board of Ireland [HPF-2014-650].
Conflict of interest
The authors have no conflict of interest to report.