
Abstract
PURPOSE:
The study aimed to examine the effects of “Cognitive Orientation to daily Occupational Performance” (CO-OP) approach in terms of performance and satisfaction as well as functional status in children with cerebral palsy (CP) receiving neurodevelopmental treatment (NDT) and determine the parents’ satisfaction level.
METHODS:
Thirty-two children with CP were randomized to experimental (n = 16) or control (n = 16) groups, with n = 2 dropouts. Therapy was applied twice a week for five weeks. The experimental group received a CO-OP plus NDT, while the control group received only NDT.
RESULTS:
No baseline differences existed, except for years of schooling, which was higher in the experimental group. After treatment, there were statistically significant and clinically meaningful improvements in occupational performance and function, favouring children who received 5-weeks of CO-OP plus NDT over NDT alone (p < 0.05).
CONCLUSION:
CO-OP is expected to be beneficial if incorporated into CP rehabilitation.
Introduction
Cerebral Palsy (CP) is described as a group of permanent disorders of the development of movement and posture that causes activity limitation are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication, and behaviour, and by secondary musculoskeletal problems [1]. Symptoms such as spasticity and contracture in CP cause a decrease in functional skill level with limitations in daily living activities such as learning a new skill or self-dressing and handwriting [2]. Alongside the motor-based occupational performance difficulties, Öhrvall et al., [3] states that children with CP often experience difficulties with planning, initiation, and problem solving, even if they function well mentally and with motor skills. The functional and skill level of a child with CP in daily living activities are important in setting the goals for rehabilitation and shaping the rehabilitation program [2].
In children with CP, neurodevelopmental therapy (NDT) is the most widely used treatment approach aimed at maximizing the child’s potential to improve motor functions while preventing musculoskeletal complications [4]. Motor learning theories emphasize the importance of including motivation, purposeful activities, and recreation in therapy programs to support development in their rehabilitation [5].
In terms of occupational therapy (OT), primary goals for those with CP include improvement of functional skills and help them gain the suitable abilities required for daily living [6]. In the last decade, new methods for children with CP have begun to emerge. Many share a common focus on skill acquisition and motor learning as well as participation and activity [7]. Likewise, modern motor performance models point towards the interaction of personal and environmental factors together with duties and the need for task-specific or top-down therapies [8].
Task-specific therapies are top-down approaches commonly used [9]. However, enhancing generalization of the individual’s skills and transferring abilities to other daily activities and objectives is not an intrinsic property of this type of approach [10]. Hence, emphasis is placed on new task-specific therapies, which are necessary to learn any new skill [11].
The Cognitive Orientation to daily Occupational Performance (CO-OP) approach, which is one of the top-down approaches, has been stated to provide strong means of generalization and transfer [10]. Furthermore, the CO-OP approach uses cognitive strategies to ease skill acquisition and adopt a different view compared to other types of therapies, such as using motor learning principles to assist children in exploring how to carry out their activities of daily living [12]. CO-OP is a performance-based treatment approach for children who experience difficulties performing the skills they want to, need to, or are expected to perform. The most important feature of CO-OP is that this approach uses collaborative goal setting, dynamic performance analysis, global and domain-specific cognitive strategies, guided discovery, and enabling principles. These elements, all considered essential to the CO-OP, are situated within the intervention format, and with parent involvement as appropriate, unlike other approaches [13]. The main difference between CO-OP, and other task-specific approaches, is that children are guided to explore strategies that work through trial and error, rather than the therapist guiding the steps to successfully accomplish the goal [14, 15].
Despite the positive findings reported, there has been limited study in the area of the CO-OP approach until now. Also, these studies have underlined the need for studies involving more participants [11, 15–17]. The conventional NDT interventions are widely used in CP treatment programs and are more bottom-up; meanwhile, the problem-solving approach CO-OP is a holistic approach to caring for children’s wishes. It will be important to explore how the addition to NDT will affect children’s occupational performance and functional status levels. Frequent parent observation of the sessions are recommended in the CO-OP approach [18]. With this respect, it would be valuable to determine the level of satisfaction of parents in terms of the achievements of their children in the therapy session. In light of this information, the objective of the study was to explore the effects of the CO-OP approach in terms of occupational performance and satisfaction, as well as functional status in children with CP who received NDT and to determine the parents’ satisfaction levels from the additional treatment their children received.
Materials and methods
The study was carried out at Hacettepe University, Department of Occupational Therapy. To study the effects of CO-OP approach plus NDT, a randomized controlled trial was performed according to the Consolidated Standards of Reporting Trials (CONSORT) checklist. The study is a randomized controlled trial with parallel group assignment using a 1 : 1 allocation ratio. Its protocol was approved by the appropriate ethical committee and was administered in accordance with the Declaration of Helsinki. It was also registered with the clinical trial registry (Trial registration number: NCT04308200). Oral and written information was given to all participants before testing and all gave their written informed consent to participate.
Participants
The inclusion criteria for participants were as follows: (a) being between 5–12 years of age; (b) being diagnosed with CP; (c) being level I, II, or III according to the Gross Motor Function Classification Scale (GMFCS); (d) being level I, or II according to the Manual Ability Classification System (MACS); (e) having encountered motor performance problems in everyday activities as stated by children and/or parents during the meeting; (f) having adequate language abilities to make contact with a therapist and be informed during intervention.
Participants were regarded as ineligible if: (a) they were receiving any treatment other than NDT; (b) they had been diagnosed with mental retardation; (c) they had serious vision or hearing problems.
Design
The sample size was calculated as a result of the power analysis performed with 80% power and 5% error rate. Thirty-six children were screened for eligibility as potential participants. Four children who were not at level I-III GMFCS or 1-2 MACS, diagnosed with mental retardation and unable to communicate, were excluded due to failure to meet the inclusion criteria. As a result, 32 participants were enrolled. All included in the study were evaluated by a single evaluator at pre-test and post-test. The NDT intervention was administered by a pediatric physiotherapist with 25-years of experience who was trained in NDT. CO-OP intervention was applied by the occupational therapist. After pre-tests and completion of the outcome measures, the participants were assigned to separate groups by block randomization. Concealed allocation through permuted block randomization was used to randomly assign the participants to either the experimental group (n = 16) or control group (n = 16). The experimental group received CO-OP plus NDT, while the control group received NDT alone.
Demographics and outcome measures
The children were evaluated in the clinical environment with parent attendance.
Demographic Data: The participants’ age (years), gender, years of schooling, Body Mass Index (BMI) (kg / m2), and duration of diagnosis (months) were recorded.
Gross Motor Function Classification Scale (GMFCS): GMFCS was used to classify children’s gross motor levels. GMFCS is a 5-level categorization system developed to categorize the gross motor functions of children with CP [19]. It aims to provide a practical means to classify children with CP in the clinic. As the motor functions of children vary according to age, the functions are defined for each level under the age of 2, 2–4, 4–6, 6–12, and 12–18 years [20]. The intraclass correlation coefficient for each age group was found to be 0.98, 0.97, 0.94, 0.98, and 0.97 respectively [21].
Manual Ability Classification System (MACS): MACS is used to determine how children with CP aged 4–18 years use their hands to grasp items in daily living activities. It is a functional classification that can be used as a complement to CP diagnosis and subgroups. It is divided into five levels. Levels 1, 2, and 3 involve children with mild restrictions, while those with serious functional restrictions are generally classified with levels 4 and 5 [22]. The Turkish version of MACS is established to be valid, reliable, and in addition, the ICC was found to range from 0.89 to 0.96 [23].
Daily Activity Log (DAL): The children were provided with DAL in the first meeting before using the outcome measures. It was used to get an idea of the child’s typical day and the activities that they had difficulty with and wanted to achieve before the goal setting process. The DAL is a simple tool used to document the activities carried out in the course of a day. The form provides a structured means of recording by listing the times of the day in half-hourly intervals along with a place for recording the major activities done during the relevant half-hourly periods. The therapist uses the log to help initiate the process of goal setting [24].
Canadian Occupational Performance Measure (COPM): COPM is used to help individuals describe occupational performance problems and precedence in the areas of self-care, productivity, and leisure, in which they have difficulty performing [25]. The COPM was used to elicit child-set goals before treatment and then measure change from treatment. In the study, participants chose “treatment goals” by rating on a 10-point Likert scale, which show their goals with regards to satisfaction and performance. Performance and satisfaction scores were specified by dividing the total scores of performance and satisfaction by the number of activities that the children regard as substantial [25, 26]. In the Turkish population, the internal consistency coefficient of COPM was found to be between 0.9 and 1 [27].
Pediatric Evaluation of Disability Inventory (PEDI): PEDI is a measurement tool developed to evaluate the functional status of children. In particular, it is arranged to determine the functions of young children [28]. It also can be used for children over the age of 7 whose functional abilities fall below those of a typical developing child [28, 29]. PEDI comprises of three essential parts: functional skills, caregiver assistance, and modifications. Each section evaluates the areas of self-care, mobility, and social function. Each of the PEDI subsegments can be used one by one. In the Turkish population, both Cronbach’s α coefficients (≥0.98) and ICC values (≥0.96) were detected to be high [30].
Visual Analog Scale (VAS): VAS is a reliable and easily applicable assessment tool that is accepted in the literature. It is used to alter non-measurable values into numerical data. It is a scale on which a person marks their current emotion level with a vertical line on a 10 cm scale. The parents’ satisfaction levels were designated using VAS after the treatment. The following wording was used: ‘Show me your satisfaction level on the line, here is no satisfaction at all (score = 0), and here is very satisfied (score = 10)’. The Cronbach’s alpha coefficients of VAS ranged between 0.73 and 0.93 [31].
As primary outcome measures of COPM and PEDI were applied pre-tests and post-tests to both the study group and the control group at 5-week intervals. In addition, as secondary outcomes, a measure of VAS, was used to rate the parents’ satisfaction levels in the study group with this approach after the therapy.
Intervention
Experimental group
In addition to the NDT program, the experimental group received twelve sessions of CO-OP, including pre-test and post-test sessions. The CO-OP approach was carried out according to the structure of the sessions suggested by Polatajko [10]. Each child was taught a global cognitive strategy during the intervention. Subsequently, they were guided to explore domain-specific strategies to enhance motor-based occupational performance problems. Dynamic Performance Analysis (DPA) began during the first session and continued throughout the intervention. The purpose of DPA is to solve performance problems by identifying where performance breaks down, identifying possible solutions, and testing them out in a trial and error fashion [10]. The child was then encouraged to generalize the abilities learnt to other life situations. Parents were advised to observe sessions as often as possible to promote adaptation and transfer to life. The sessions were carried out individually with all participants. In the last one, COPM and PEDI evaluations were repeated to check whether the selected targets were achieved. In addition, VAS was used to determine the parents’ satisfaction level of the CO-OP approach after the therapy.
Control group
The control group received the NDT alone. Its protocols generally aimed at enhancing muscular tone and movement patterns. NDT program was standardized as much as possible for the participants who had similar motor impairments and severities. Although the therapy activities differed for each participant, the overall goal included providing normal movement experience to minimize motor-sensory disorders. All sessions aimed to change muscle tone during movement and to facilitate anti-gravity, weight-shifting, and postural reactions through various techniques. The control group received NDT twice a week for a period of five weeks, with each session lasting approximately 30 to 45 minutes.
Statistical analysis
Statistical analyses were implemented by the use of the Statistical Package for Social Sciences (SPSS) version 22. One sample Kolmogorov-Smirnov Test was used to assess the distribution of variables before test choice. Group properties and outcome measures were defined using mean and standard deviations for continuous variables, while frequencies and ratios were used for categorical variables. Descriptive statistics were demonstrated in the median for non-normally distributed quantitative and ordinal data, while the categorical variables were demonstrated in numbers (percentage). Since the data is not normally distributed, the Wilcoxon signed-rank test was used to test the mean differences between pre and post-interventions. The Mann-Whitney U test was used to see whether the differences between the scores in the experimental and control groups were statistically significant. Statistical significance level was assumed at p < 0.05.
Clinical significance was calculated by using the Cohen’s d effect size index in independent groups. It was determined according to Cohen’s recommended limit values (i.e. small effect: <0.3, moderate effect: 0.3–0.8 and large effect: >0.8) [32].
Results
Of the 32 participants, 16 were randomly assigned to the control group and 16 to the experimental group. However, one participant in the experimental group could not complete the study due to illness, and one in the control group voluntarily dropped out of the study resulting in 30 individuals, namely 15 in the experimental group and 15 in the control group. The CONSORT flow diagram of the study is provided in detail in Fig. 1.
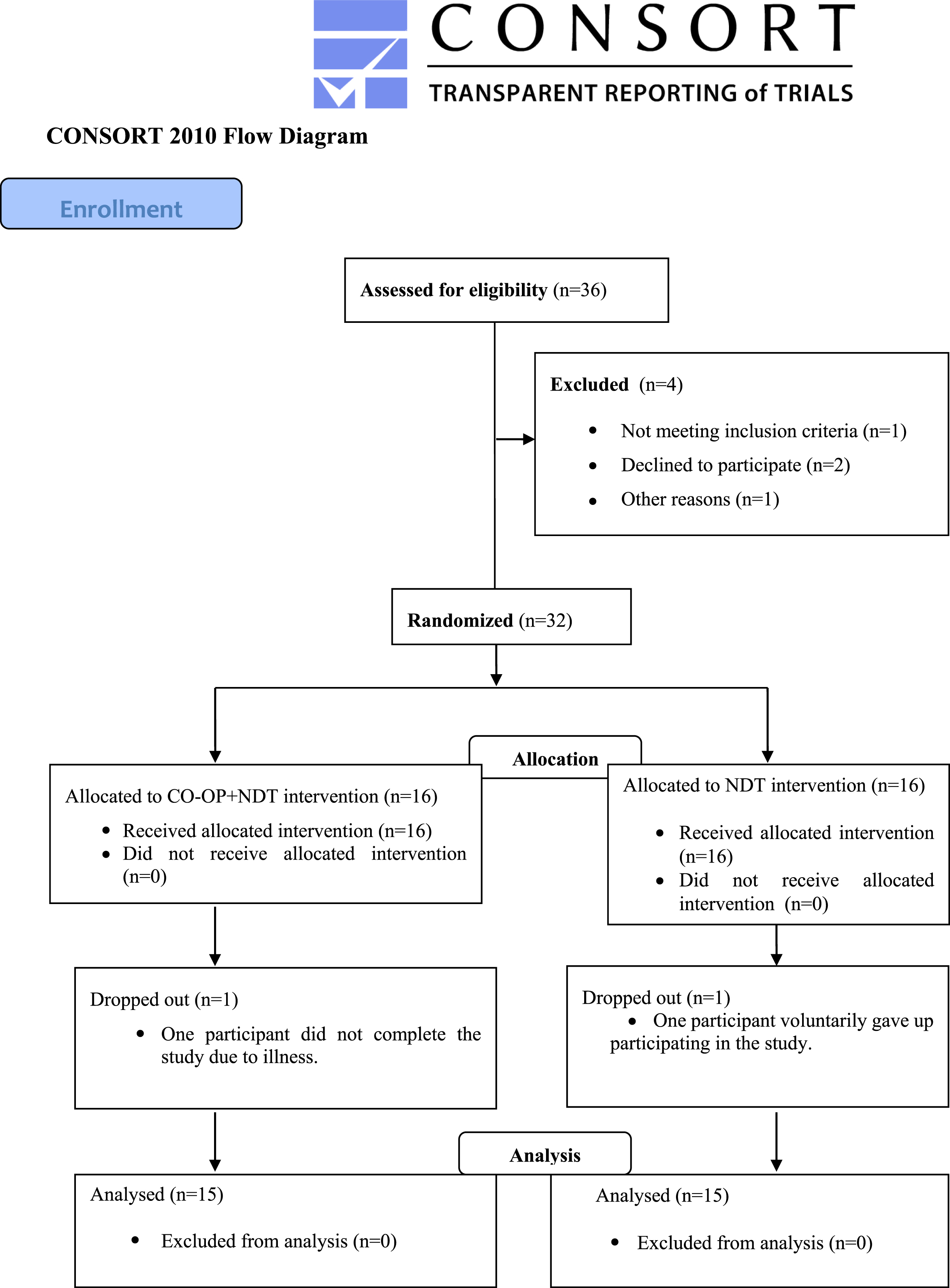
Flow chart.
The data of 30 participants in the experimental group (7 male and 8 female participants) and control group (8 male and 7 female participants) were analyzed. All were at the elementary education level. The age, education (years), BMI (kg / m2), and duration of diagnosis (months) distributions of the participants are demonstrated in Table 1. Pre-test values showed that each group was well-matched in terms of age (year), BMI (kg / m2), and duration of diagnosis (months). However, there was a difference between the groups regarding the years of schooling.
Baseline variables of the sample
BMI: Body Mass Index. Mann-Whitney U test (z-table value) statistics were used to compare the two independent groups without normal distribution. * Statistical significance was accepted as p < 0.05.
All children in the study selected three goals before treatment. The distribution by activity area of the goals determined by the individuals participating in the study is indicated in Table 2.
Summary of the 45 treatment goals (3 per child) and their frequencies
COPM: Canadian Occupational Performance Measure.
The COPM performance and satisfaction scores were compared within groups before and after treatment and are shown in Table 3. The results of COPM indicated a clinically significant increase in both performance (p < 0.05) and satisfaction (p < 0.05) scores in the experimental group. In the control group, COPM performance score improvement was statistically significant (p < 0.05) but not clinically meaningful, as two or more points of changes on the COPM are needed for clinically meaningful difference [25]. There was no statistically significant difference in occupational satisfaction of the control group.
Comparison of baseline and end of treatment values of Canadian Occupational Performance Measurement and Pediatric Evaluation of Disability Inventory scores in the groups
Comparison of baseline and end of treatment values of Canadian Occupational Performance Measurement and Pediatric Evaluation of Disability Inventory scores in the groups
COPM: Canadian Occupational Performance Measure; PEDI: Pediatric Evaluation of Disability Inventory. Wilcoxon Signed rank test (W-table value) statistics were used to compare the baseline and end of treatment values among the groups without normal distribution. *Statistical significance was assumed to be p < 0.05. aeffect size > 0.80.
The effect sizes of the two groups are shown in Table 3. In terms of post-test values, examination of the statistical effect of the difference between the groups’ occupational performance and satisfaction revealed that the experimental group exhibited a larger effect compared to the control group with regard to the COPM occupational performance and satisfaction score (effect size > 0.80). On the other hand, the effect size of performance and satisfaction scores in the control group was below 0.3.
The between-group comparisons of the occupational performance and satisfaction scores of the individuals in the experimental and control groups are shown in Table 4. According to the pre-test values compared between the experimental and control groups, there was a statistically significant difference in occupational performance, while there was no statistical difference in occupational satisfaction. At post-test, there was a statistically significant between-group difference in both performance (p < 0.05) and satisfaction (p < 0.05) levels favouring the CO-OP group.
Between-group comparisons of Canadian Occupational Performance Measurement and Pediatric Evaluation of Disability Inventory scores in the baseline and end of treatment values
COPM: Canadian Occupational Performance Measure; PEDI: Pediatric Evaluation of Disability Inventory. Mann-Whitney U test (z-table value) statistics were used to compare the two independent groups without normal distribution. *Statistical significance was assumed to be p < 0.05.
Functional skills and caregiver assistance subscale scores of PEDI in the pre-test and post-test values of the participants are demonstrated in Table 3. There was a statistically significant increase in the functional skills (p values < 0.05) and caregiver assistance (p values < 0.05) subscale scores of the individuals in the experimental group. In the control group, a statistically significant increase was detected only in the total score of functional skills (p < 0.05), but there was no statistically significant difference in the other areas.
Moderate effect sizes (effect size between 0.30 and 0.80) were detected in the functional skill scores of the experimental group (Table 3). In the caregiver assistance scores, only a small effect size was observed in the mobility area, whereas in other areas, a medium effect size was determined. On the other hand, the effect size of all the scores in the control group was below 0.3.
Between-group comparisons between the pre-test and post-test of functional skills and caregiver subscale scores of the individuals in experimental and control groups are shown in Table 4. According to the pre-test values, there was no statistically significant difference between the individuals of the experimental and control groups in terms of functional skills and caregiver assistance sub-parameters in self-care and social functions.
Parent satisfaction following CO-OP was high (9.80±0.47).
Discussion
The study aimed to evaluate whether the CO-OP plus NDT led to superior improvements in occupational performance and function compared to NDT alone. The findings showed that CO-OP plus NDT improved children’s performance and satisfaction scores as well as their functional status. Furthermore, it was found that the satisfaction levels of the children’s parents with this approach were quite high. All participants in the experimental group were able to learn and practice the global and domain-specific strategies in CO-OP and achieved important advancements in most of their goals. The addition of the CO-OP approach to the routinely applied and disorder-focused NDT approach increases the gains of children after the treatment.
Livingston et al. investigated which issues of participation are important for adolescents with CP. It was observed that the issues were mostly related to leisure time, mobility, school, and socialization [33]. Studies conducted by Lemmens et al. (2014) observed that the activities in which children with CP face problems were connected to upper extremity functions and were mostly related to individual needs and social demands in their activities of daily living, whereas; those between the ages of 6–11 especially preferred dressing and leisure time activities [34]. In another study, the activity preferences of children with hemiparetic CP and their parents were examined as well as their performance and satisfaction levels in these activities. It was found that children reported more problems in the areas of play/productivity, whereas their parents reported more problems in self-care areas [35]. In the present study, most of the preferred targets were self-care and leisure time activities, which is in line with the literature.
In a mixed design study, the CO-OP approach was applied to 5 children with CP. According to the results of that study, both the performance and satisfaction scores increased [11]. In a randomized controlled pilot study, 9 of the 18 children with CP received the CO-OP approach, and 9 received the Current Practice Approach. The CO-OP group was indicated to have achieved positive effects on occupational performance and satisfaction scores [17]. The study explored the individual characteristics of children with CP and brain injury who participated in the CO-OP approach. It was revealed that after therapy, the occupational performance and satisfaction scores had improved with the majority of the participants [15]. In the feasibility study on young adults with spina bifida and CP, it was suggested that the CO-OP approach had positive influences on occupational performance and satisfaction scores [36]. The aforementioned studies included other diagnostic cases alongside CP, whereas in the present study, a wider range of participants who were children with only CP were tested. It was found that the occupational performance and satisfaction scores of the participants who took the CO-OP approach increased significantly compared to the control group which is consistent with the literature. A comparison of post-test COPM performance and satisfaction scores in the control group and experimental group manifested that the experimental group indicated a statistically significant increase compared to the control group. COPM was proposed to be clinically beneficial when a difference of more than 2 points was detected. The experimental group exhibited an increase of more than 2 points in performance and satisfaction. Consequently, a statistically significant and clinically efficient increase was found in the performance and satisfaction of the treatment goals compared to the control group. Therefore, it can be deduced that there was not as much of a clinically efficient difference in occupational performance of the control group. In other words, the CO-OP approach was more efficient.
To the best of the authors knowledge, no studies have been performed to date with the aim of investigating the effects of the CO-OP approach on the functional status of children with CP using PEDI assessment in their daily activities. However, it has been reported that information obtained from PEDI, as one of the scales evaluating the functional situation, is also suitable for goal setting and program planning [37]. This study observed that the CO-OP approach has an improving effect on the PEDI sub-parameters of functional skills and caregiver assistance in all sub-parameters. These findings promote the emphasis that the CO-OP approach has a positive effect on adapting and transferring the acquired skills to life. Compared to the experimental group, there was a lower increase in the functional skills total score in the control group. It is believed that the reason for this increase observed in the control group was due to the participants continuing their NDT treatment.
A study performed with semi-structured interviews explored the experiences of the parents of six CP children participating in the CO-OP approach. It was seen that the parents thought of it as a valuable means of therapy that helped their children reach the goals set and transfer these to future goals [38]. This study also observed similar results: that families were very satisfied with the CO-OP approach and transferred them to their future goals.
As CO-OP provides a cognitive strategy, this approach was shown to be highly useful in the therapeutic environment when included with NDT. Compared to the control group, the experimental group also showed greater advances in occupational performance, occupational satisfaction, and functional status. The CO-OP appears to be more useful in increasing performance, satisfaction, and functional status so that the children can perform the relevant activities successfully.
Limitations/Future adaptations
At baseline, the experimental group had higher educational attainment by chance, which may have affected the outcome of the treatment and provided an alternative explanation for the between-group differences. Moreover, the two groups were not homogenous in terms of years of schooling. Although these may be considered a limitation, it should be noted that the two groups were homogenous in terms of age. When the pre-test findings of the two groups were compared, it was observed that there were differences in the occupational performance of the children, the mobility areas, and the total scores of PEDI. However it was found that the experimental group was more successful when the effectiveness of the treatment was compared in terms of post-tests. PEDI was preferred as it was the only test that evaluates the functional status having Turkish validity and reliability. Since NDT is mandatory in the programs for children with CP, the CO-OP approach was applied in addition to NDT in the study. It would be invaluable to apply the CO-OP approach alone with comparisons of different task-oriented based interventions for the future studies taking into account children with all levels of GFMCS and MACS. Finally, further large studies with follow-up times are warranted to confirm these results.
Conclusion
This study clearly shows that the gains after the treatment increased with the addition of the CO-OP approach in children who take the NDT approach. The study identified whether the performance in children with CP increased in terms of the occupational performance and functional status. A comparison was performed between two groups in this regard. In this study, it was revealed that the CO-OP plus NDT increased the occupational performance and satisfaction levels of the participants and also improved their functional status. Thus, the CO-OP approach supports skill acquisition by improving children’s performance levels, which are necessary to perform their daily occupations. Although their caregivers are also very satisfied with this approach, these findings constitute exciting developments for the available CP therapy programs. Therefore, co-administration of the CO-OP approach to NDT has proven to be an effective training method in the treatment of CP. Therefore, the CO-OP approach is expected to be highly beneficial if incorporated into CP rehabilitation.
Footnotes
Acknowledgments
We would thank to all participants.
Conflict of interest
The authors have no conflicts of interest to report. No funding was received.
Ethical considerations
The study protocol was approved by the Ethics Committee of Hacettepe University (approval no: GO 18/624) and was administered in accordance with the Declaration of Helsinki.