
Abstract
Background:
Late Onset Pompe Disease (LOPD) is a rare myopathy characterized by prevailing weakness of trunk and pelvic girdle muscles that causes motor disabilities. Spinal deformities have been reported unclearly on clinical examination. No study quantitatively assessed upright posture defining specific alterations of LOPD various phenotype.
Objective:
Identify postural abnormalities in a homogeneous group of LOPD patients using 3D Stereophotogrammetry (St) and x-Ray (xR).
Methods:
Seven LOPD siblings were recruited. They were assessed by clinical scales and, in upright posture, using xR and 3D-St with a new marker set protocol. Fourteen healthy individuals, age and sex-matched, were used as controls for St-parameters; normative xR-values were found in literature.
Results:
LOPD patients showed a significant weakness of trunk and tibialis anterior muscles. Statistical analysis of St-parameters showed a larger ankle, knee, elbow, dorsal, S2-C7, heel-S2-C7, heel-S2-nasion angles and a lower sagittal vertical axis (SVA) than controls.
xR-analysis highlighted an absence of scoliosis and a lower occipito-cervical, C2-C7 cervical and Cobb dorsal angles, and a trend to lower lumbar lordosis and SVA compared to normal values. Significant correlation was found in dorsal and lumbar angles calculated using xR-markers placed on spiny apophysis, xR-centre of vertebral bodies, Cobb-method and St-markers.
Conclusion:
This is the first quantitative study of postural abnormalities in LOPD patients using 3D-St and xR, highlighting sagittal standing alignment changes, difficult to assess to direct exam.Our new St-protocol showed a high reliability compared to xR. Further studies on larger population of LOPD might confirm the usefulness of these instrumental methods for monitoring disease course.
Keywords
INTRODUCTION
Pompe Disease is a rare autosomal recessive neuromuscular disorder, due to mutations of the GAA gene codifying the lysosomal acid alpha1-4-glucosidase enzyme (acid maltase, GAA), and characterized by glycogen accumulation primarily in skeletal, cardiac and smooth muscle [1]. Mutations causing reduction of musculoskeletal GAA activity below 1% the normal, lead to very severe infantile form (IOPD) which is incompatible with life if not treated early with enzyme replacement therapy (ERT) [2]. Levels of GAA activity between 1% –25% the normal, cause late onset form (LOPD) which may occur at any age from 2 to 70 years. This mild form has a better prognosis for life expectance than IOPD form, but about 35% of patients is confined to wheelchair and/or requires mechanical ventilation before the age of 65 and all LOPD patients show postural and motor disabilities [3]. Recent clinical trials demonstrated that ERT leads to better functional results if it is established earlier and associated with rehabilitation [4, 5]. Unfortunately, LOPD diagnosis occurs after an average delay of 10 years, owing to the variability of clinical manifestations, the rarity of the condition and the overlap of signs and symptoms with other neuromuscular diseases [6].
The phenotypic spectrum of LOPD is quite broad considering the different age of onset, (varying from early infancy to late adulthood), the heterogeneity of musculoskeletal involvement and the rate of disease progression, even in patients carrying the same mutations of GAA. Despite these differences, arecent systematic review reported that about 80% of LOPD patients showed a clinical triad that consists of a primary involvement of the pelvic girdle, respiratory and trunk musculature [7]. LOPD patients were also classified into three clinical subgroups, the Limb Girdle and Diaphragmatic Weakness (LGDW), the Rigid Spine Syndrome, Scoliosis and Low Body Weight (RSS) and the Cardio-cerebrovascular (Cc) patterns, in relation to their shared prevailing symptoms [8]. MRI studies revealed an involvement of para-spinal lumbar muscles (multifidus, longissimus, iliocostalis muscles) in pre-symptomatic patients with HyperCKemia as the only manifestation, whereas abdominal rectus, psoas, iliacus and posterior muscle of the thigh were further involved in symptomatic patients [9]; the severity of muscle changes at MRI-T1w score strongly correlated with muscle weakness, exercise intolerance, decreased endurance, fatigue, difficulties during transitions between positions, reaching upright standing (Gowers’ maneuver), ambulation, running and climbing stairs [7, 9]. Weakness of trunk muscles is associated to spinal deformities. In particular, a third of LOPD patients has been reported to be affected by scoliosis (235/711) and about half of them had been diagnosed by x-Ray (136/235). In this subgroup, kyphosis and lordosis abnormalities were respectively found in 19/136 and 21/136, even if the type of abnormalities and the age of onset were not specified [10].
To the best of our knowledge, only one study highlighted the alterations in postural control of LOPD patients by stabilometric test using a force platform [11], but no study has ever analysed quantitatively whole-body standing alignment.
Based on these observations, aim of our study was to assess postural abnormalities in a sibship of LOPD adults by gold standard instrumental methods: x-Ray for spinopelvic parameters and 3D Stereophotogrammetry for whole-body upright posture. This quantitative evaluation could clarify the clinical uncertainties about pathological postural pattern, identifying specific parameters potentially useful for diagnostic suspicion of disease and for quantitative monitoring of treatment outcomes.
MATERIAL AND METHODS
Subject populations
Seven LOPD siblings, sharing the same GAA mutation compound, were recruited in Neuromuscular Disease Centre of the University of Campania “L.Vanvitelli” and assessed using clinical scales (Medical Research Council [MRC] and Range Of Movement [ROM]), x-Ray (xR) and 3D Stereo-photogrammetry (St) in upright posture. Fourteen healthy individuals, age and sex-matched, were used as controls for St-parameters.
Data gathering
Quantitative evaluation of upright postural alignment was performed using the SMART stereo-photogrammetric system (BTS Bioengineering-Milano, Italy); a new markers set protocol (titled DB-Total, Fig. 1A) was specifically designed for better studying the spine, the head, the arms on the sagittal plane and the feet on the frontal plane, extending standard Helen Hayes M.M. protocol [12] (Fig. 1A -blue markers). Markers were placed on the following landmarks: nasion (Ns), frontozygomatic suture (FZs), spinous processes of C7 -T7 -T12 -L3 -L5 -S2, acromioclavicular joint (ACj), epicondylus humeri (eH), ulnar styloid (Us), anterior-superior iliac spine (ASIS), greater trochanter (gT), medial (mEF) and lateral (lEF) epicondylus femoris, fibular head (Fh), medial (mM) and lateral (lM) malleolus, I°-III° and V° metatarsal head (MtH), heel (He) bilaterally.
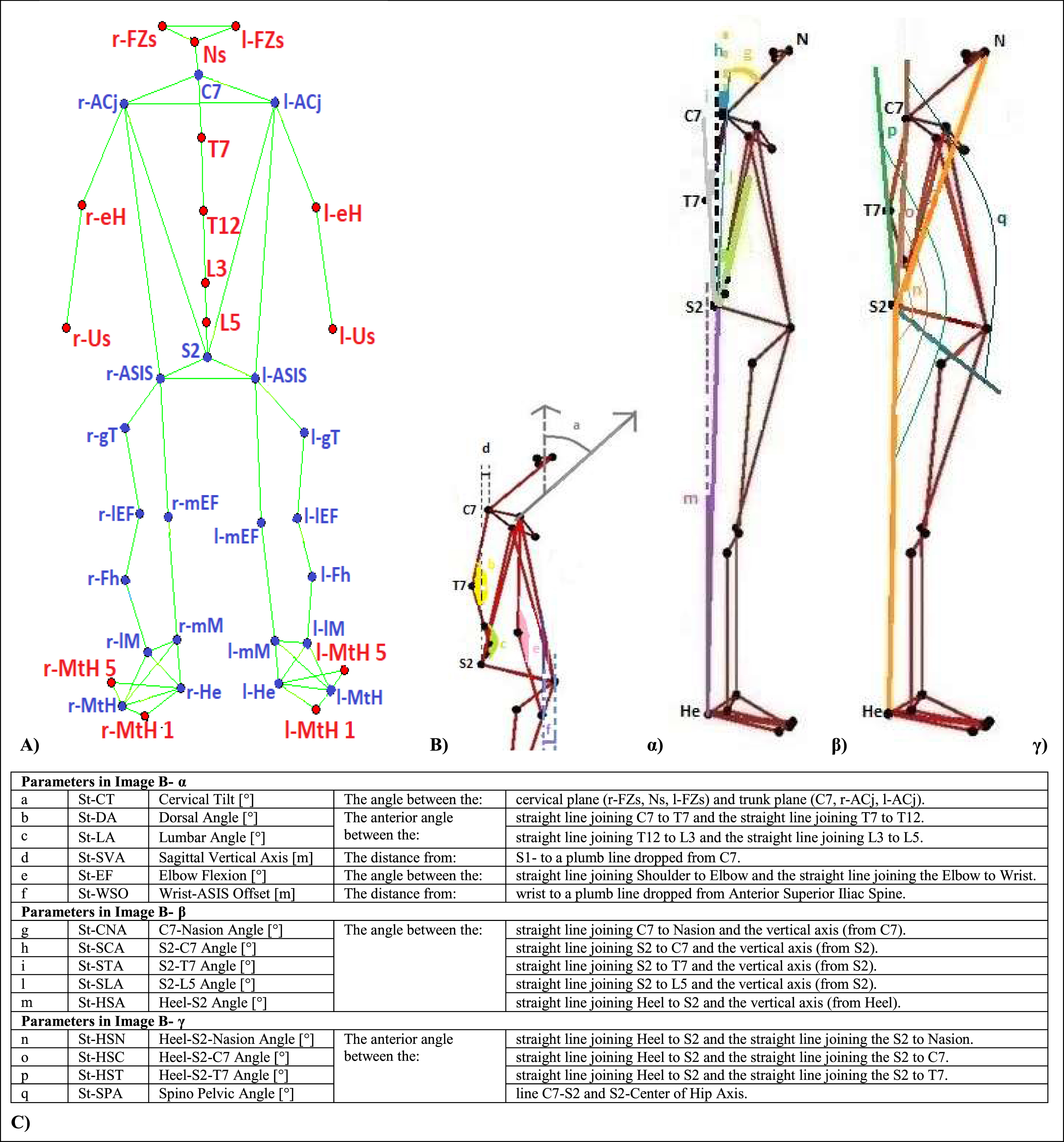
A) DB Total markers placement protocol shown on stick diagram indicating the bodily segments elaborated by tracking of software BTS (label of landmarks);B) DB Total stick diagrams associated to calculated sagittal parameters;C) definitions of stereophotogrammetric parameters. Figure note: Stereofotogrammetric (St). Helen Hayes Medial Markers protocol [12] in blue and additional DB Total markers in red: nasion (Ns), frontozygomatic suture (FZs), spiny apophysis of C7 -T7 -T12 -L3 -L5 -S2, acromioclavicular joint (ACj), epicondylus humeri (eH), ulnar styloid (Us), anterior-superior iliac spine (ASIS), greater trochanter (gT), medial (mEF) and lateral (lEF) epicondylus femoris, fibular head (Fh), medial (mM) and lateral(lM) malleolus, I° -III° and V° metatarsal head (MtH), heel (He). Dashed lines represent vertical axes.
Before 3D-St analysis, spinous processes of interest (Fig. 2, A) were located and marked by an experienced physiatrist using a skin-compatible pen with patient in perfect orthostatic position; radiopaque markers were placed on aforementioned spinal points and radiographic spinopelvic parameters [13–19] (Fig. 2 B, C) were assessed by x-Ray (OperaG80HF –GMM –Seriate (BG) –Italy), acquiring plain film radiograms in a frontal and lateral view. Subsequently, St-markers were always placed by the same expert operator on the previously signed spinal points and other landmarks, in according to DB-Total protocol. Eventually, the participants underwent an upright static measurement for 3 seconds in the motion analysis laboratory.
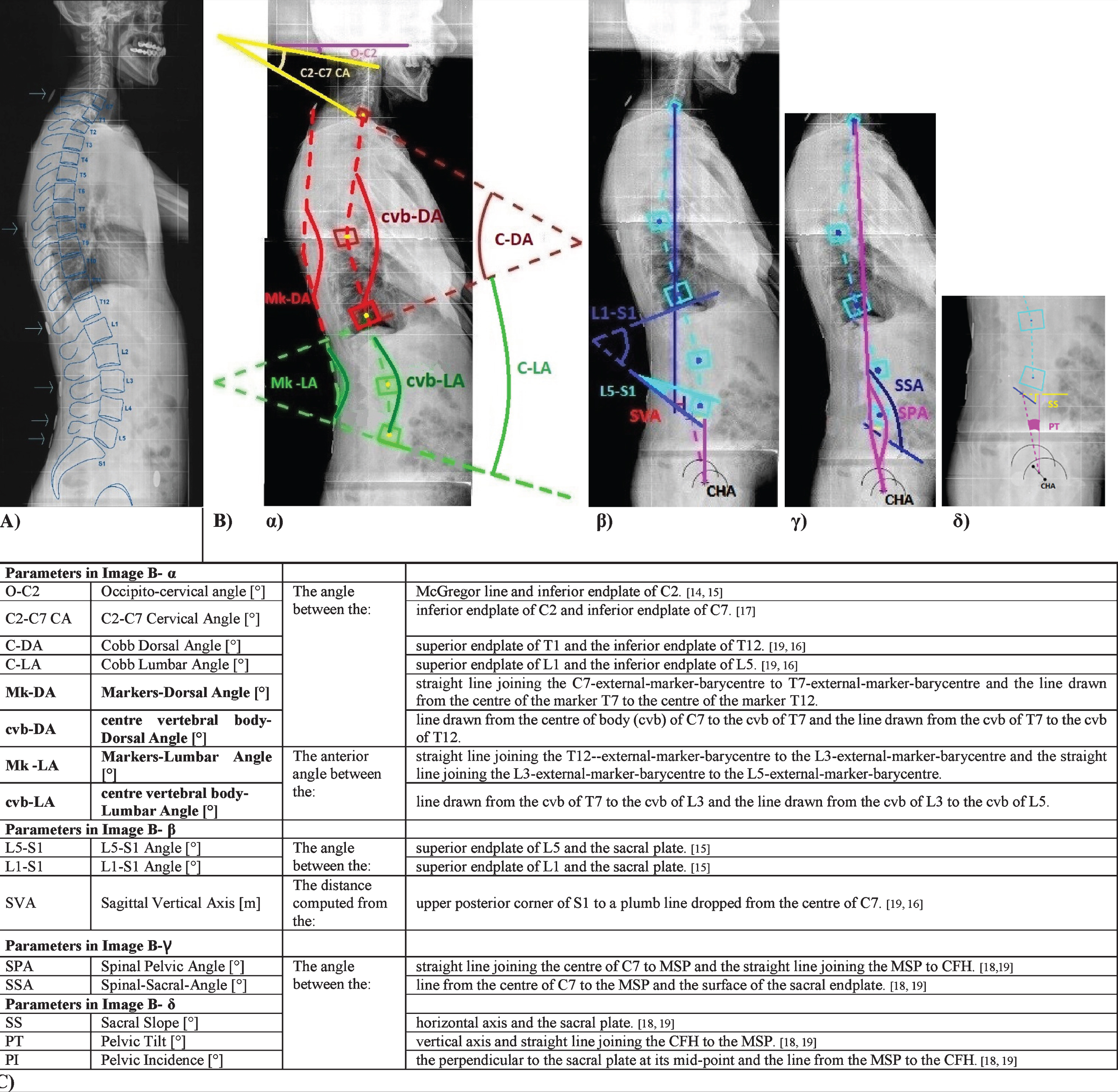
A) x-Ray of sagittal spine, highlighting vertebral body, spiny apophysis and radiopaque markers placed on C7-T7-T12-L3-L5-S2; B) Radiographic parameters calculated with Matlab script; C) definitions of radiological parameters. Figure note: x-Ray of two different patients; MSP: mid-point of the sacral plate; CFH: centre of the femoral heads.
Data pre-processing and analysis of standing data
Data were exported from BTS and processed in Matlab (MATLAB Release 2017b, The MathWorks, Inc., Natick, Massachusetts, United States) with ad hoc developed software.
We analysed the whole-body postural parameters concerning DB Total protocol (as showed in Fig. 1). Using Matlab, radiological values were evaluated and plotted on the x-Ray images, as shown and explained in Fig. 2 B, C. To this aim, an expert radiologist manually identified landmark points (vertebral corners, the profile of the sacral plate, and the profiles of femoral heads) on radiographic images using Osirix; landmarks coordinates were input into ad hoc developed Matlab script.
Statistical analysis
As the aim of the study was to individuate the upright posture parameters more suitable to a characterisation of the LOPD patients compared to the healthy population, for each St and xR parameter the distribution between the two populations was analysed. For clinical and St parameters healthy population was recruited as control group, while for xR normative values were found in literature [13–21]. In particular, baseline features and ROM values have been tested for clinical differences between patients and controls using Wilcoxon-Mann-Whitney test (WMWt), while MRC ones with Wilcoxon Sign test.
Moreover, WMWt was used to evaluate separation between patients and healthy subjects for St-parameters, while t-test was used for xR parameters. P-values less than 0.05 were considered statistically significant different.
Pearson’s correlations coefficients (including confidence intervals) have been computed between St and xR parameters in order to assess the reliability of DB-Total markers set protocol (correlation coefficient: 0.5–0.7 = moderate, > 0.7 = strong correlation). All statistical analysis has been performed in R [22].
RESULTS
Baseline features of LOPD patients (L) and controls (C) are shown in Table 1; no significant difference was found between two groups (Table 1).
Baseline features andclinical evaluation. Mean and Standard Deviation or median were reported for each parameter of patients and controls. Significant differences (p-value < 0.05) between patients and controls have been tested using Wilcoxon test* and Wilcoxon Sign test**
Note: LOPD: Late Onset Pompe Disease; MRC: Medical Research Council; a-, p-ROM: active, passive Range of Motion; SD: Standard Deviation.
LOPD group showed a significant lower strength especially in flex-extensor trunk and tibialis anterior muscles (average MRC = 2), while the other dorsiflexors ankle as extensor digitalis and hallucis longus were less or not compromised; moreover, a significant lower active e passive dorsiflexion (a- and p-ROM) of ankle was found (Table 1, Fig. 3 a, b).
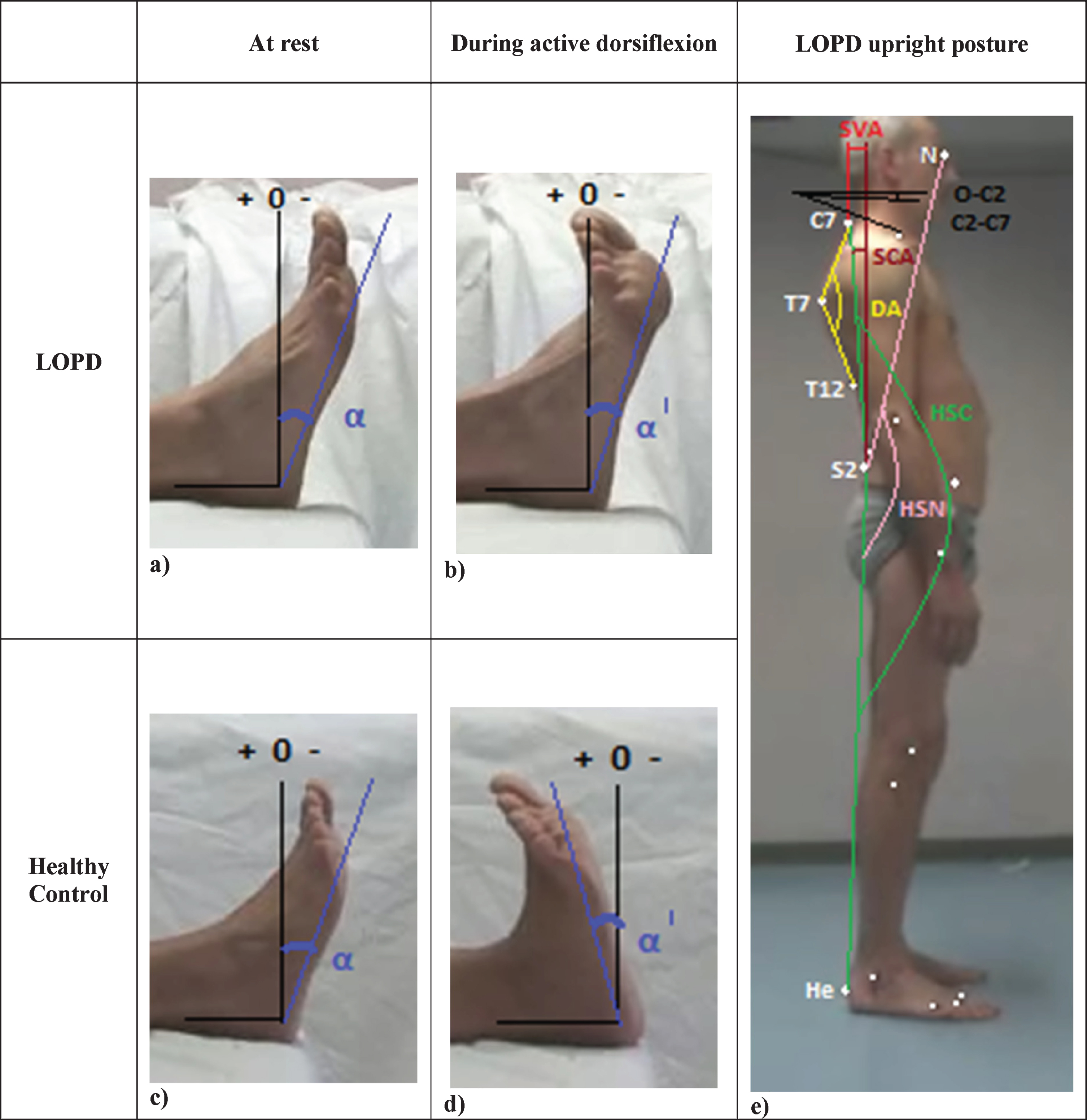
Comparison between LOPD and healthy feet at rest (a, c) and during active dorsiflexion (b, d) on sagittal plane. Upright posture evaluated on sagittal plane with highlighting of significant St and xR parameters in LOPD patients (e). Figure note: α= ankle angle (at rest), α′ (during dorsiflexion); in LOPD patients α′ < 0, while in healthy Controls α′ > 0. St (stereophotogrammetric); xR (radiographic); HSN (Heel-S2-Nasion Angle); HSC (Heel-S2-C7 Angle); DA (Dorsal Angle); SVA (Sagittal Vertical Axis); SCA (S2-C7 Angle); He (Heel); N (nasion); O-C2 (Occipito-cervical angle); C2-C7 (Cervical Angle).
As regard the evaluation of upright posture, stereophotogrammetric analysis showed significant differences in sagittal parameters, with a larger dorsiflexion ankle, flexion knee, dorsal, S2-C7, Heel-S2-C7 and Heel-S2-Nasion angles and a lower Sagittal Vertical Axis (SVA) in the Pompe group compared to the healthy controls (Table 2; Fig. 3 e).
Mean and standard deviation of stereo-photogrammetric (in Helen Hayes M.M. and DB Total protocols) and radiographic parameters were reported. Significant differences (p-value < 0.05) between the two groups were computed using Wilcoxon Mann-Withney Test and T-test respectively and highlighted. Radiografic normal values refer to the following articles [14, 21]
Note: St: Stereophotogrammetric; xR: x-Ray; Mk: Markers; cvb: centre of vertebral body; K: kyphosis; L: Lordosis; DA: Dorsal Angle; LA: Lumbar Angle; NA: Non-available.
About radiographic spinopelvic measurements, no spinal abnormality was found in the frontal plane, but only 4 patients showed deviations < 10°, 2 of them were thoraco-lumbar (with curve length > 8 vertebrae) and other 2 thoracic. Instead, significant differences were found in sagittal angles with a reduction of occipito-cervical (O-C2), C2-C7 cervical (C2-C7-CA) and Cobb Dorsal angles (C-DA) and a trend of reduction of SVA in LOPD patients respect to the normal values (Table 2, Fig. 3 e).
Moreover, a strong correlation was found between xR and St parameters: 1) dorsal and lumbar angles calculated using xR markers placed on spiny apophysis (xR-mks) and St markers (St-mks); dorsal angles calculated using 2) St markers (St-mks) and xR centre of vertebral bodies (xR-cvb), 3) xR-mks and xR-cvb and 4) xR-mks and Cobb Angle (Table 3).
Correlation coefficients with Confidence Intervals (CI) between radiographic and Stereo-photogrammetric parameters: Mk- and cvb- angles, Mk- and St- angles, cvb- and St- angles; Mk and Cobb angles, St and Cobb angles; St-SVA and SVA. The strong and significant correlations between parameters the two groups are highlighted (correlation coefficient > 0.7 and< –0.7; p-value < 0.05)
St: Stereophotogrammatic; Mk: Markers; cvb: centre of vertebral body; C-DA: Cobb dorsal angle; C-LA: Cobb lumbar angle; DA: Dorsal angle; LA: Lumbar angle.
DISCUSSION
The aim of the study was to quantitatively assess the muscular weakness of specific anatomic districts and related postural alterations in upright standing of LOPD patients. Our results showed a weakness of trunk muscles, in accordance to previous reports [1, 7], but also of tibialis anterior muscle, classically present in ERT-treated infantile Pompe disease [2]. A few study had already shown rare involvement of tibialis anterior [9] or altered activation pattern during maximal contractions [23] in adult late onset form. Tibialis anterior muscle deficit is an unusual and interesting finding that is probably related to this subgroup of LOPD siblings: it explains the characteristic morphology of these patients’ feet during passive and active ankle dorsi-flexion that result decreased but not insufficient because the strength of other dorsiflexor muscle is more or less preserved (Fig. 3 a,b,c,d; Table 1).
Moreover, this is the first study that evaluate whole-body standing alignment in LOPD patients using 3D-stereophotogrammetry and, at the same time, x-Ray for spinopelvic parameters.
A new marker set protocol (DB Total protocol, Fig. 1, A), created ad hoc extending standard Helen Hayes M.M. protocol (Fig. 1 A-blue markers) in order to study new specific stereophotogrammetric parameters (Fig. 1 B, C), was introduced to better analyse the postural abnormalities of LOPD patients. Previous “conventional gait models” [24] evaluated especially kinematic joint of pelvis and lower limbs, usually considering the trunk as a single segment and rarely the head; moreover, the most reliable St parameters were found on sagittal plane [25, 26].
A few studies [27, 28] analysed sagittal spine parameters dividing the trunk into several districts and introducing a larger number of markers placed on the spine than standard protocols, but no correlation study was performed between stereophotogrammetric and radiological sagittal angles. To the best of our knowledge, only one study [29] has validated own St marker set for the assessment of lumbar and thoracic curvature in adults with scoliosis, comparing xR and St results. Strong correlations were found between vertebral bodies angles, radio-opaque and stereophotogrammetric angles on sagittal rather than frontal plane and, in particular, for the thoracic spine, in agreement with our study (Table 3). In fact DB Total protocol showed a strong correlation between xR - St parameters and a high reliability in matching markers to spinous processes of the reference vertebrae and in detection of dorsal angles; a lower correlation was found in lumbar angles probably due to the higher thickness of the adipose tissue present in this area.
About stereophotogrammetric evaluation, LOPD patients showed a significant larger dorsal angle, indicating a flattening of the dorsal curve, and a trend of lumbar hypolordosis compared to controls; these results are in disagreement to the literature that previously reported an excessive kyphosis and lordosis [7, 10]. Moreover, a larger S2-C7 angle and a lower Sagittal Vertical Axis revealed a C7 position posterior to the sacrum; these findings, associated to a larger dorsiflexion ankle, flexion knee, Heel-S2-C7 and Heel-S2-Nasion angles (Table 2), highlighted a typical sagittal upright posture of LOPD patient (Fig. 3 e), as a result of a postural compensation strategy for the spinal extensor muscles weakness [9, 30].
About radiographic spinopelvic results, no spinal deviation > 10° was found on frontal plane but only a trend of mild spinal curvature with length > 8 vertebrae, typical of neuromuscular scoliosis [31].
Instead, on sagittal plane, a significant lower Cobb dorsal angle (Table 2) than normative values [14, 21] confirmed the reduction of dorsal kyphosis emerged in stereophotogrammetric analysis; moreover, a significant lower O-C2 and larger C2-C7 cervical angles, found in LOPD patients, revealed a straightening of the cervical lordosis (Fig. 3 e).
No significative difference was found for Cobb lumbar angle, but only a trend of hypo-lordosis in accordance with St-results. Finally, only a reduction trend of SVA was found compared to normal values.
The results of the present study should be evaluated and considered with respect to some limitations. The relatively small sample size of the recruited population prevents to any definitive conclusion because of small statistical power. Investigation over larger population are required. Nevertheless, the genetic homogeneity of the LOPD patients, the accuracy of our marker set protocol demonstrated by x-Ray exam and the exclusive choice of sagittal stereophotogrammetric parameters [25, 26], make our results reliable. Further studies would be needed to better evaluate these quantitative outcome measures not only in static upright posture but also during motor tasks that stress LOPD-specific weak muscles (as walking, sit to stand), in order to highlight pathognomonic postural pattern and verify them in a larger LOPD population and in comparison to other myopathies for differential diagnosis.
CONCLUSIONS
Our study is the first to evaluate quantitatively the upright posture of LOPD patients using 3D-St and sagittal spinopelvic parameters by xR, highlighting postural abnormalities difficult to identify on clinical examination. Moreover, our St-marker set protocol showed high reliability compared to xR, especially for dorsal and sagittal whole-body angles. The finding of these specific postural parameters in a larger LOPD population might confirm the usefulness of these instrumental methods to investigate and monitor the course of the disease and the response to treatment.
CONFLICTS OF INTEREST
The authors declare that there is no conflict of interest
FUNDING
This work was supported by the Inter-University Centre for Research in Neurosciences and University of Campania “Luigi Vanvitelli”.
CONSENT TO PARTICIPATE AND FOR PUBLICATION
Written informed consent was obtained from all participants.
AUTHOR CONTRIBUTIONS
Paolo De Blasiis and Simone Sampaolo conceived and designed the study. Paolo De Blasiis, Filomena Napolitano and Chiara Terracciano recruited the patients and performed clinical assessments. Paolo De Blasiis, Mario Sansone and Allegra Fullin contributed to the acquisition, analysis and interpretation of the data. Paolo De Blasiis drafted the first article. Simone Sampaolo, Maria Rosa Anna Beatrice Melone, Giacomo Lus and Luca Del Viscovo have critically revised the content. All authors have read and approved final version of the manuscript. The material within has not been and will not be submitted for publication elsewhere except as an abstract.