
Abstract
Background:
Carbon dioxide tension (PCO2) monitoring during sleep, is crucial to identify respiratory failure in patients with neuromuscular disorders (NMD). Transcutaneous PCO2 monitoring is an available technique to measure PCO2.
Objectives:
To assess the quality level of transcutaneous blood gas measurements via SenTec monitor.
Methods:
A 12-month analysis of SenTec measurements was conducted in a Belgian Centre for Home Mechanical Ventilation (HMV). Over two consecutive nights; SpO2 and PCO2 measurements, the presence of PCO2 drift and drift correction with SenTec, were reviewed and scores (0, 1, 2 for poor, medium and high level) were assigned to estimate the quality of measurements.
Results:
Sixty-nine NMD patients met the inclusion criteria, of which 48/69 used HMV. PCO2 drift and drift correction were present in 15% and 68% of the 138 recordings, respectively. The quality level of measurements throughout night 1, scored 1.55 (0–2). The relevance of our clinical findings from SenTec scoring 1.94 (1–2); was considered highly satisfactory. HMV was ineffective in 24/48 patients. Among 12 patients with hypercapnia, 8 patients improved PCO2 between night 1 and 2. Among 12 patients with hypocapnia, PCO2 improved in 4/12 patients, who reached the range of normal PCO2 (35–47 mmHg).
Conclusions:
The quality of SenTec measurements was acceptable in the majority of recordings and clinical findings were deemed satisfactory in all cases. A single SenTec measurement was sufficient to determine the need for NIV. However, two SenTec registrations were insufficient to both improve NIV effectiveness in 50% of cases, and, to ensure follow-up of our interventions.
What the study adds to the field of knowledge. Nocturnal transcutaneous blood gas exchange measurement via SenTec monitor provides satisfactory clinical findings Obtaining consistent quality measurements is challenging Training sessions of nurses using SenTec at night are desirable A single SenTec can be sufficient to screen whether NIV is needed Multiple SenTec can be required to adjust interventions in patients with ineffective nocturnal NIV.
INTRODUCTION
Neuromuscular disorders (NMDs) are degenerative disorders, which are predominantly hereditary. They are characterized by progressive weakness of body muscles. According to the diagnosis, the progression of NMDs can be either slow or rapid and can affect infants, children and adults [1]. NMDs can affect respiratory muscles, leading to chronic respiratory failure [2]. Respiratory failure is characterized by hypoventilation during sleep, and later, during both night and day [3]. At the time of respiratory failure, noninvasive ventilation (NIV) via a nasal mask is offered during sleep [4, 5].
Hypoventilation during sleep is characterized by hypercapnia - an elevated carbon dioxide tension level (PCO2); and oxygen desaturation - a low level of oxy-hemoglobin present in blood (SpO2). A technique to detect hypoventilation, consists of electrochemical transcutaneous measurements of PCO2 and SpO2, via an ear clip during sleep [6]. Doctor Philippe Soudon, from our institution, introduced this technology in Belgium in the early 1980’s [7]. In our country, the initiation of NIV is based on the following measurements: gas exchange during both sleep and wakefulness, lung function and anamnesis of patients. According to the Belgian agreement for the establishment and follow up of home mechanical ventilation, the criteria to access NIV are defined as follows (https://www.inami.fgov.be/SiteCollectionDocuments/overeenkomst_ademhalingsondersteuning_thuis.pdf). Criterion (2) is primarily used to initiate NIV in our hospital:
“Patients with restrictive lung disease of neuromuscular origin meeting one of the following criteria:
PaCO2≥47 mmHg during the day. or nocturnal transcutaneous oximetry with a decrease in SpO2 to ≤90% for at least 5 consecutive minutes and nocturnal arterial, transcutaneous or end-tidal PCO2≥47 mmHg for at least one hour in total time in bed. or suffering from
–restrictive lung disease as a result of a rapidly progressing neuromuscular disease with a loss of at least 10% of the value of Forced Vital Capacity (FVC), measured in two consecutive studies with a maximum of 1 year apart
–or restrictive lung disease as a result of a rapidly progressing neuromuscular disease and a maximum inspiratory pressure <60 cmH2O or a VC <50% of the predicted value.”
Because full polysomnography recordings have limitations regarding availability, cost and access; this technology is not used in our Rehabilitation Hospital. During sleep, accurate and simpler tests via transcutaneous monitors, are reported to be beneficial in the management of sleep-disordered breathing. Monitors produced by various manufacturers are widely used across the World [8]. There is evidence that transcutaneous PCO2 and SpO2 monitoring, is both accurate and reliable enough to ensure the respiratory follow-up of patients in chronic settings. There is also a positive relationship between transcutaneous and arterial PCO2 [9–11]. However, there are some limitations regarding these monitors. Primarily, testing does not clearly identify the reasons for NIV ineffectiveness. The detection of: asynchronies between the ventilator and the patient, leaks through the mouth or the nasal mask and ineffective settings; can all be ascertained through additional explorations [12]. Full polysomnography can be used when available [13]. Alternatively, simple tools can be used to collect ventilation parameter data from patients receiving HMV. Most of the recent ventilators are equipped with Secure Data (SD) cards. Data can then be reviewed by clinicians and ventilator prescriptions adjusted. Analysis from SD cards provides information about: tidal volume and potential overshoot suggesting leaks, achieved pressures, leaks, minute ventilation and respiratory rate [14], and potential apneas, hypopneas, and asynchronies [15]. The compliance of patients using NIV is also easy to follow. However, evidence is lacking as to whether using ventilator data downloads provides value in terms of patient outcomes and cost-effectiveness [14]. An additional template used by nurses to collect clinical information during NIV supported sleep, provides useful contextual information. In our Hospital, this template includes the following items, which are collected every 30 minutes by nurses who record: actual settings given by the ventilator, the leaks (L/min) when available, the body position, the state of wakefulness, the visual presence of leaks and snoring. This template is very useful for the interpretation of the SenTec data.
The technical advances of SenTec monitors are reported in a recent report [16]. As illustrated in Fig. 1, drift and drift correction of PCO2 signal is part of this technology; and is related to individual diffusion capacities of the skin, which is itself influenced by the thickness and microcirculation of the skin [16]. Additional unwanted drift can occur when the electrodes are not placed according to the manufacturer’s guidelines.
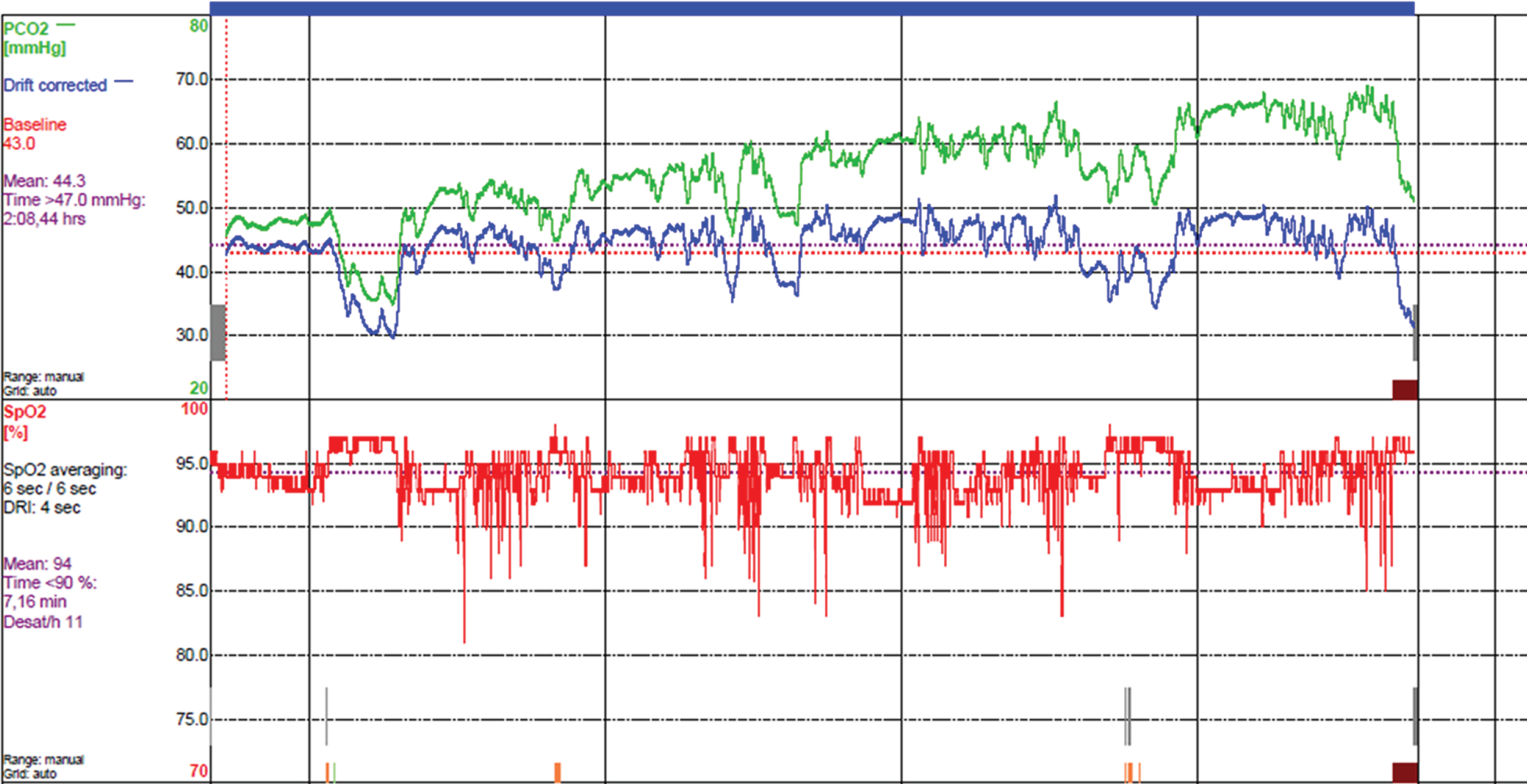
Unperfected SenTec measurement in patient # 49, affected by Limb Girdle Dystrophy. The Sentec recordings include a PCO2 drift (green line) corrected by a drift correction (blue line). This patient uses ineffective nasal ventilation during sleep (presence of massive leaks through the mouth).
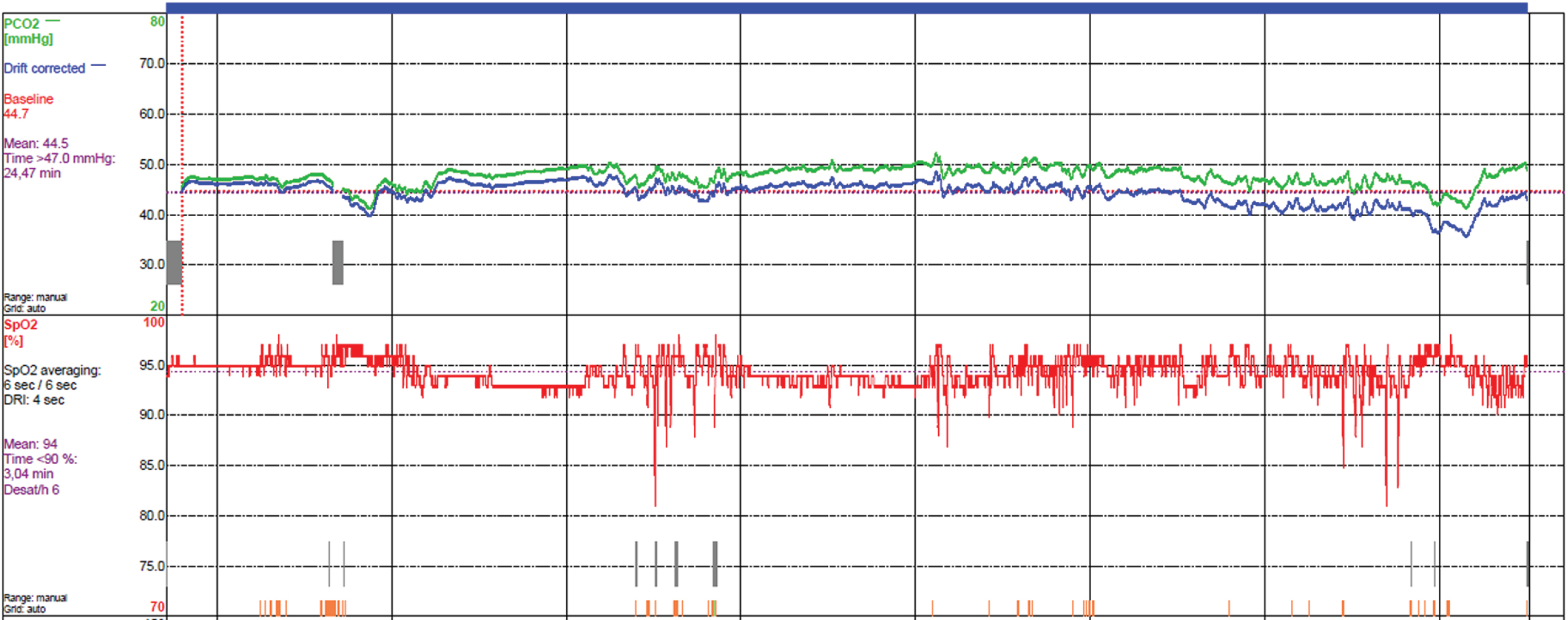
Improvement of the quality of a second SenTec measurement in patient # 49. Nasal ventilation is improved with an better control of the leaks with the use of a chinstrap during ventilation.
At Inkendaal Rehabilitation Hospital, we used the SenTec device (SenTec AG, Therwil, Switzerland) to monitor patients with NMDs. During the past months, we intensified the use of SenTec devices. In our experience, it was challenging to obtain high quality recordings during sleep. To explain this challenge, SenTec monitors are high-technology and complex devices [16] that are handled by nurses [17] who perform a significant number of tasks each night. Yet those devices are fragile and require caution when handled. As a consequence, we were faced with growing and recurrent errors, inconsistent alarms, uncontrolled PCO2 drift signals and absence of PCO2 drift corrections, dirty membranes and joints, errors during calibrations and replacement of calibration gas, and also errors during membrane replacement.
For this reason, we organized group-training sessions to educate our nurses working on night shift. Despite our initial efforts, technical problems did not disappear, and we still faced recurrent errors. As a result, we had to interpret incomplete data that could have compromised the relevance of clinical findings and, in turn, lead us to potentially make hazardous clinical decisions. We asked ourselves the following questions. What is the quality of our SenTec measurements? Are they relevant? Do we record unexpected drifts? Do we download the recordings properly, including the drift correction? Can we make a clinical decision, even when the SenTec recordings are not perfect? What is the rate of successful interventions implemented after SenTec data analysis?
In general, quantitative information involving troubleshooting from overnight studies of SenTec recordings, is still lacking [10]. In order to measure the quality of transcutaneous recordings and the related impact on the respiratory management in adult NMDs, we conducted a one-year retrospective study to analyze the data from our SenTec measurements.
Aims
We aimed at quantifying the quality of Sentec signals by counting and scoring the technical issues during two consecutive SenTec (nights 1 and 2) in the same patient; analyzing the reproducibility of SenTec recordings between two nights, and scoring the quality of clinical findings. A second goal of this study was to assess the effectiveness of our interventions to improve NIV in adult neuromuscular disorders between SenTec 1 and 2.
MATERIAL AND METHODS
Patients
All adults affected by NMDs and attending the Centre for Home Mechanical Ventilation of Inkendaal Rehabilitation Hospital between March 2019 and February 2020, were considered for study inclusion. Individuals starting nocturnal NIV signed an informed consent prior to NIV implementation.
Inclusion criteria
All adult patients with NMD, either NIV users or candidates for using NIV, attending Inkendaal Hospital and monitored using SenTec recordings for a minimum of two consecutive nights.
Exclusion criteria
Single night SenTec recordings and/or daytime only rather than nocturnal measurements, acute respiratory infection during the study period, patients using CPAP devices.
Study design
In this 12-month retrospective study, individuals acted as their own control during an admission to our Centre for Home Mechanical Ventilation. Transcutaneous PCO2 and SpO2 measurements were tested for two consecutive nights in the same patients. Nurses started the 8-hour SenTec measurements at 10 PM and stopped at 6 AM. All nurses working night shift, were offered a group-training session in order to use the SenTec devices appropriately, prior to the study. They were also trained to download the data in the early morning via a dedicated computer with appropriate software.
Material
Continuous SpO2 and TcCO2 were recorded continuously during sleep via an ear clip connected to a transcutaneous SenTec monitor (SenTec AG, Therwil, Switzerland). Transcutaneous PCO2 and SpO2 was measured during each night with a SenTec monitor. According to the criteria from the Belgian agreement on Home Mechanical Ventilation, we recorded the time spent with SPO2 < 90% and PCO2 > 47 mmHg. The last author, head of the Centre for Home Mechanical Ventilation Inkendaal, reviewed the SenTec reports according to the study period and inclusion/exclusion criteria. Scores were given for each SenTec recording. The scores aimed at reflecting our judgment on the quality level scored between bad (0), medium (2) or excellent (3), for the following outcome measures. Figure 1A illustrates an unperfected SenTec measurement that includes an unwanted drift (consistent increasing of PCO2 signal) but with a drift PCO2 correction.
Outcome measurements
Primary outcomes measures
The presence of a PCO2 drift, highlighting a bad contact between the membrane and the skin, was scored as either 0, absent drift or 1, present drift. Drift can be defined as a clear and consistent trend to increase or decrease, irrespective of the respiratory events occurring during sleep with spontaneous or assisted breathing. The presence of the drift correction (PCO2 blue line present), related to the correct downloading of data in the computer, was also scored as 0, absent correction and 1, present correction. The quality level of SenTec recordings (nights 1 and 2) was scored as follows: 0, poor quality, with drift without correction; 1, medium quality, without drift or with drift and correction; and 2, high quality, without any drift or artefact issue. The reproducibility of the quality of SenTec recordings between the first and the second night was scored as 0, decreasing quality; 1, stable quality; and 2, improved quality. Finally, the help in decision-making after SenTec 1 and 2, was scored as 0, no clinical decision possible; 1, unclear decision; and 2, easy clinical decision.
Secondary outcome measures
In patients using noninvasive ventilation (NIV) ineffectively, the adequacy of our interventions to improve PCO2 was scored as 0, PCO2 worsened; 1, PCO2 stabilized; and 2, PCO2 improved. Effective ventilatory support was considered when PCO2 was in the normal range of values, defined as 35–47 mmHg. Median SpO2 (%) and PCO2 (mmHg) values, and time (minutes) spent at PCO2 > 47 mmHg and SpO2 < 90%, were compared between the first and second night with SenTec monitor. Improvements in PCO2 were considered when patients reached the range of normocapnia (35–47 mmHg).
Data analysis
Data was tested for normality with Kolmogorov-Smirnov test and reported as median (Minimum-Maximum) for abnormal distribution. Comparisons between SenTec 1 and 2 were performed by Wilcoxon test. P < 0.05 was considered as significant.
RESULTS
During the study period, 105 patients with NMDs were seen for routine respiratory control via SenTec measurements. Sixty-nine patients met inclusion criteria. The reasons for exclusion are reported in the flow chart of Fig. 2. Diagnosis included 21 individuals affected by Duchenne Muscular Dystrophy, 17 by Amyotrophic Lateral Sclerosis, 10 by Limb Girdle Dystrophy, 7 by Spinal Muscular Atrophy, 5 by Congenital Myopathies, 4 by Charcot-Marie-Tooth, and 5 by miscellaneous forms of NMDs. Mean age was 45.1 (SD: 17.1) years and 48/69 used nocturnal NIV at home. Two SenTec measurements were reviewed in each patient. A total of 138 SenTec recordings were analyzed. Results are presented as primary and secondary outcome measures with median (min-max) values.
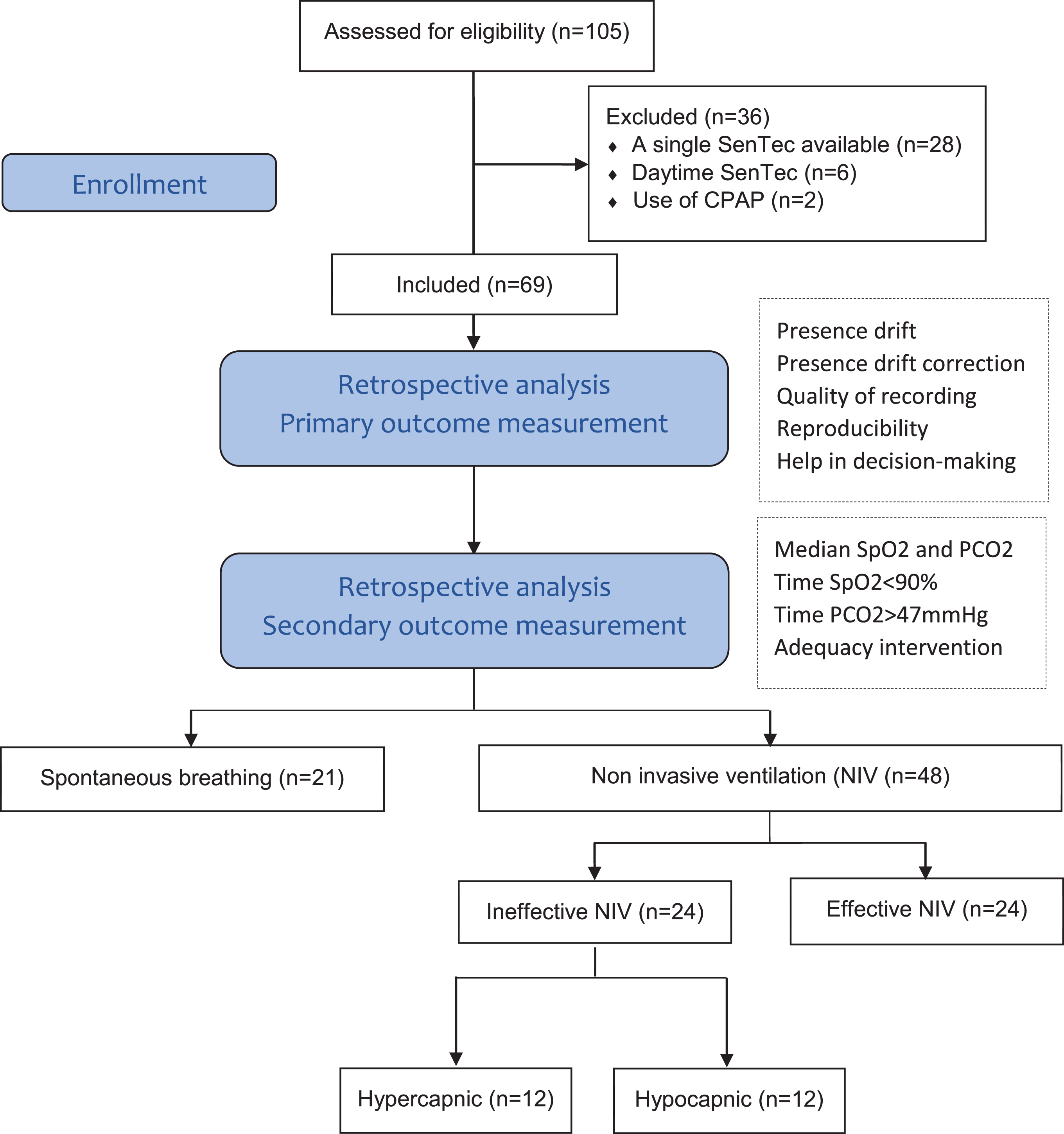
Flow chart diagram.
Primary outcome measures
The score of quality of SenTec recordings reached 1.55 (0–2) and 1.45 (0–2) points from a maximum of 2 points for SenTec (night) 1 and 2, respectively (NS; p = 0.37). A PCO2 drift was present in 17% and in 12% (p = 0.35), and drift correction in 80% and 65 % in SenTec 1 and 2 (p = 0.06). The score assessing the reproducibility of recordings between the first and the second night was scored as 0.78 (0–2) of 2 points, suggesting a tendency to poor reproducibility with slight deterioration of the quality of recordings and download between SenTec 1 and 2. Finally, the help in decision-making after data analysis from SenTec 1 and 2, was scored as 1.94 (1–2) and 1.74 (0–2), suggesting overall easy clinical decision-making (difference SenTec 1 and 2, p = 0.16).
Secondary outcome measures
Among the 69 patients with NMDs included in the study, 48 individuals were invited to control for nocturnal NIV effectiveness. Among them, 24/48 patients (50% of NIV) were controlled as normocapnic with effective NIV at night, while another 24/48 patients presented initially with values out of the range of normocapnia (35–47 mmHg) during the first night. Tables 1 and 2 report data analysis through SenTec 1 recordings from two sub-groups: hypercapnic and hypocapnic group.
Group hypercapnic NIV patients
NIV: Noninvasive ventilation; hypercapnic refers to PCO2 > 47 mmHg; SpO2: O2 saturation; SpO2 < 90% : time of the night spent at SpO2 < 90%; PCO2: CO2 tension; PCO2 > 47 mmHg: time of the night spent at PCO2 > 47 mmHg; NA: not available because the sample size was too small to allow a reliable calculation of the Wilcoxon signed-rank statistic; * p value <0.05.
Group hypocapnic NIV patients
NIV: Noninvasive ventilation; hypocapnic refers to PCO2 < 35 mmHg; SpO2: O2 saturation; SpO2 < 90% : time of the night spent at SpO2 < 90%; PCO2: CO2 tension; PCO2 > 47 mmHg: time of the night spent at PCO2 > 47 mmHg; NA: Not available because the sample size was too small to allow a reliable calculation of the Wilcoxon signed-rank statistic; *p value <0.05.
Nocturnal NIV was deemed ineffective in a sub-group of 12 hypercapnic patients (25% of all NIV patients) as suggested by PCO2 > 47 mmHg recorded in Sentec 1. After assessment of our interventions between Sentec 1 and 2, 8/12 patients improved and reached PCO2 < 47 mmHg and 4/12 worsened or stabilized with PCO2 > 47 mmHg. Figure 1A and B illustrate the improvement of the quality of recordings and NIV. Interventions varied between: changes in ventilator settings (pressure, rate, target volume, trigger), implementation of a chinstrap to compensate for oral leaks, change of nasal mask or change in body position in bed. Despite PCO2 not improving in 4/12 individuals, the time spent with PCO2 > 47 mmHg decreased between the two nights (Table 1). When looking at the 8/12 improved patients, PCO2 decreased from 53 to 42.9 mmHg (p < 0.01) between the two nights, suggesting a consistent change in 67% hypercapnic patients after one intervention. The 33% who did not reach PCO2 lower than 47 mmHg were invited to receive a third consecutive SenTec measurement or were invited for another PCO2 control in the short term. The results of any further SenTec sessions are not part of the current study.
In the group of hypocapnic patients, 12 individuals (25% of all NIV) presented hyperventilation with persistent hypocapnia (PCO2 < 35mmHg). A decision was made to support ventilation at a lower level by reducing pressure and/or tidal volume, plus the rate and inspiration time of cycles of assisted ventilation. Four patients improved with PCO2 > 35 mmHg after our intervention as assessed via SenTec 2, but 8/12 worsened or stabilized with PCO2 < 35 mmHg. Except for the 4 improved patients, where PCO2 increased from 31 to 42.4 mmHg (p = 0.04) between the two nights, we were not able to normalize PCO2 in this group (Table 2). The clinical decision taken after SenTec 1 was a posteriori deemed as satisfactory in 4/12 (33%) of hypocapnic NIV patients. Details of individuals of the two sub-groups are reported in the online supplement 1 and 2.
DISCUSSION
To our knowledge, this is the first study reporting on the troubleshooting of transcutaneous blood gas measurements and their impact on clinical findings. This is also the first study assessing the impact of the quality level of recordings, as well as on the interventions made to improve the efficiency of mechanical ventilation in neuromuscular patients in the short term.
Firstly, we recorded a good quality level of SenTec recordings with a lower rate of drift issues, than initially expected. Absence of drift correction, was the largest technical issue with a prevalence of 32% of 138 SenTec recordings, while unwanted drifts were observed in only 15% recordings. It must be noted that 25% of missing drift correction was observed during both nights in the same patients, suggesting human factors influencing the absence of drift correction, invaliding calibration data. This can occur when: the sensor was disconnected from the monitor for >30 minutes, the sensor was exposed to ambient air for >30 minutes, the sensor was removed from the docking station more than 12–16 hours ago if the ‘Calibration Interval’ was ≤8–12 hours. It also can occur when the nurses do not change the membrane when requested by the monitor, or when calibration is not performed at all or aborted by the user (docking station door opened before termination of the calibration). Finally, it can occur when gas leak is detected.
Storre et al. [10] reported that a limitation of transcutaneous PCO2 monitoring is the occurrence of technical drifts that affect the quality of recordings throughout the night. Fortunately, a substantial improvement in PCO2 drifts is seen with the recent SenTec monitors [10]. According to the group of Storre, we recorded low drift problems. The score of quality level reached 1.5/2 points, which is an estimation between ‘medium’ and ‘high’ quality level. Accordingly, we were able to obtain relevant clinical findings in all cases, and we were able to decide on interventions to improve the respiration of our adult NMDs when needed. Unfortunately, the quality of recordings between the first and the second night worsened in the majority of patients, suggesting that we did not learn from our errors and failed to improve the quality level in the short term. In other words, we were not able to improve the quality of the second SenTec when the first one was not satisfactory. This finding is essential to argue for the need to intensify the training of the nurses in our hospital.
Secondly, we found that a single SenTec can be sufficient to screen for the need for NIV; but that multiple SenTec nocturnal measurements can be required to adjust interventions in patients with ineffective nocturnal NIV. Fifty percent of NIV patients had ineffective assisted ventilation during the study period, 25% with hypercapnia and 25% with hypocapnia.
Interestingly, only 67% of hypercapnic patients were improved in the short term. This is important, since patients resist staying longer than 48-hours in the hospital for NIV controlled observations. However, the present study suggests that multiple nights can be useful. We found that optimization of nocturnal ventilation, was not reached in 33% of hypercapnic patients by 48 hours. NIV adjustments such as: changes in the settings on the ventilator, the type of mask, the body position during sleep, and sometimes, the adjustment of a chinstrap to control the leaks at night with NIV, were insufficient to control PCO2. Despite the limited time available to improve NIV, 67% of the hypercapnic patients improved or stabilized during the night following our interventions.
The improvement of hypocapnic patients was more challenging. Only one third of this patient group had satisfactory PCO2 after our intervention, while two thirds worsened after reducing the pressure and/or the volume, set on the ventilator. Again, this finding suggests that we would need more than two consecutive nights to control PCO2 in those hyperventilated patients.
Our findings highlight the need for a higher quality level of SenTec measurements. Van Weteringen et al. reported that this technique remains laborious [16]. They suggest implementing trainings, to be able to distinguish technical/operator failure from measurement drift, stemming from patient factors influencing the measurement.
The encouraging results of the current study encourage us to strengthen the training of nurses. We recently decided to train night shift nurses on an individual basis via one- on-one educational sessions in Inkendaal Hospital. An assessment of this training regarding the assessment of drift issues, will be conducted prospectively in 2020-2021, using the same methods as for the current study. We also decided to restrict several technical activities to our technical staff. For example, membrane switches and change of calibration gas bottles.
Limitations of the study
There are limitations in the present study. These include the typical risks of the biases inherent in retrospective studies with limited numbers of patients. This study was monocentric and used largely subjective evaluation, rather than objective data in an heterogeneous population of NMDs. Additionally, we did not collect data other than drift issues troubleshooting. For instance we did not quantify dirty membranes, inadequate placement of the membrane on the skin, losing time before downloading, and other human related errors. Another limitation is that our interventions to improve NIV were not consistently documented. In the hypercapnic patients, we suggested new settings, sometimes a totally different mode of ventilation, even sometimes a different ventilator. Other patients were invited to sleep in a different position, some others received a chinstrap to control the leaks. In the hypocapnic patients, we tried to decrease the ventilatory support by changing the settings; either by reducing the inspiratory pressure, shortening the inspiration time, reducing the target volume or a combination of the three.
We did not systematically use the ventilator SD cards and did not report the content of the templates with the nurse’s notes. However, documenting our interventions was not the goal of the current study. The objective of the study was to see if the quality of the SenTec recordings, provided satisfactory clinical findings. Despite these limitations, our study highlights that the rate of drift and absence of drift corrections was low; and that our SenTec recordings allowed either effective screening of the need for NIV, or diagnosis of NIV effectiveness.
In conclusion, we found that the quality level of nocturnal transcutaneous blood gas exchange measurements, via SenTec recordings, is challenging but satisfactory. A single SenTec monitored admission is sufficient for NIV screening. However, multiple SenTec monitored nights, can be required to adjust interventions in patients with ineffective nocturnal NIV. In the future, drift and drift corrections should be improved by training nurses rostered on night shift.
CONFLICT OF INTEREST
The authors have no conflict of interest to report