
Abstract
Objectives:
To evaluate the efficacy of intensive care unit ventilators versus dedicated noninvasive ventilators when used for noninvasive ventilation.
Methods:
This was a secondary analysis of data from a multicenter prospective observational study. Eligible patients were recruited from 17 hospitals in China between September 2017 and September 2021. Inclusion criteria were restricted to those receiving noninvasive ventilation for acute hypoxemic respiratory failure. The type of ventilator used was determined at the discretion of the treating clinicians. The primary objective was to compare clinical outcomes between intensive care unit ventilators and dedicated noninvasive ventilation ventilators for noninvasive ventilation delivery. Key outcomes included noninvasive ventilation failure rate, 28-day mortality, intensive care unit length of stay, and hospital length of stay.
Results:
A total of 2054 patients were enrolled, with 5% (n = 103) receiving noninvasive ventilation via intensive care unit ventilators and 95% (n = 1951) via dedicated noninvasive ventilation ventilators. No significant difference was observed in the overall noninvasive ventilation failure rate between the two groups (46% versus 38%, p = 0.15). However, the median time from noninvasive ventilation initiation to endotracheal intubation was shorter in the intensive care unit ventilator group (9 h, interquartile range: 3–25) compared with the dedicated noninvasive ventilation ventilator group (21 h, interquartile range: 6–65). The 28-day cumulative incidence of noninvasive ventilation failure was significantly higher in the intensive care unit ventilator group (log-rank test p = 0.01; crude hazard ratio = 1.43, 95% confidence interval: 1.06–1.91; adjusted hazard ratio = 1.41, 95% confidence interval: 1.04–1.93). No significant difference was found in 28-day mortality between the groups (16% versus 17%, p = 0.79). The 28-day cumulative incidence of mortality also did not differ (log-rank test p = 0.65; crude hazard ratio = 0.84, 95% confidence interval: 0.52–1.34; adjusted hazard ratio = 0.95, 95% confidence interval: 0.58–1.55).
Conclusions:
The use of intensive care unit ventilators for noninvasive ventilation is uncommon in China. Based on low-level evidence, intensive care unit ventilators are not associated with a difference in mortality compared with dedicated noninvasive ventilation ventilators, but are linked to earlier endotracheal intubation.
Introduction
Noninvasive ventilation (NIV) functions as a pivotal therapeutic bridge between conventional oxygen therapy and invasive mechanical ventilation, facilitating the delivery of positive airway pressure without the need for endotracheal intubation. In patients with acute hypoxemic respiratory failure, NIV effectively reduces respiratory workload, alleviates respiratory distress, and improves oxygenation. 1 Compared with standard oxygen therapy, it decreases the incidence of intubation and the utilization rate of invasive mechanical ventilation.2,3 Given that invasive mechanical ventilation is associated with multiple complications, including ventilator-associated lung injury, ventilator-associated diaphragmatic dysfunction, and ventilator-associated pneumonia,4–6 NIV has been integrated into clinical practice as a conditional recommendation.7,8
Two primary types of ventilators are utilized for NIV in acute hypoxemic respiratory failure: intensive care unit (ICU) ventilators and dedicated NIV ventilators. ICU ventilators were originally designed for operation within a leak-free closed circuit in patients who have undergone endotracheal intubation. However, during NIV application, leaks at the patient-mask interface are inevitable. To address this issue, NIV-specific algorithms (commonly referred to as “NIV modes”) have been developed in the latest generation of ICU ventilators to mitigate the impact of such leaks. 9 In contrast, dedicated NIV ventilators are primarily engineered to manage leaks and optimize patient comfort via a single-limb circuit.10,11 Equipped with specialized algorithms for air leak compensation, these devices have demonstrated superior patient–ventilator interaction compared to ICU ventilators in bench studies, even in the presence of significant leaks.12,13 Despite these technical differences, ICU ventilators remain widely used for NIV in clinical settings, with some reports indicating utilization rates as high as 100%.14,15 The comparative effectiveness of these two ventilator types in real-world clinical practice remains unclear. Therefore, this study aims to evaluate the clinical outcomes associated with ICU ventilators versus dedicated NIV ventilators when employed for NIV.
Methods
This study was a secondary analysis of a prospective observational study conducted to develop a scoring system for predicting NIV failure in patients with acute hypoxemic respiratory failure. 16 For the current study, patients receiving NIV across 17 hospitals in China between September 2017 and September 2021 were enrolled. The study protocol was approved by the respective ethics committees (approval no. 2016150). Written informed consent was obtained from all patients with legal capacity. For patients experiencing delirium, written informed consent was obtained from their legally authorized representatives.
All patients receiving NIV for acute hypoxemic respiratory failure were screened. Acute hypoxemic respiratory failure was defined by the fulfillment of all the following criteria: (1) arterial oxygen partial pressure/fraction of inspired oxygen (PaO2/FiO2) < 300 mmHg; (2) arterial carbon dioxide partial pressure (PaCO2) < 50 mmHg; 3) respiratory rate >25 breaths/min or clinical manifestations of resting respiratory distress (e.g. active contraction of accessory inspiratory muscles or paradoxical abdominal motion). Patients aged ⩾16 years were included in this study. Exclusion criteria were as follows: NIV use following scheduled or accidental extubation; NIV use due to treatment failure of high-flow nasal cannula therapy; prior NIV use for >2 h before admission to the participating center; and unavailable data on NIV ventilator type.
NIV management was performed by attending physicians, respiratory therapists, and responsible nurses. The selection of ventilators for NIV was based on clinicians’ clinical experience. Disposable two-limb circuits were used for ICU ventilators, while disposable single-limb circuits were used for dedicated NIV ventilators. Both types of ventilators were equipped with a humidifier and a thermometer. The humidification temperature was adjusted based on patient comfort, tolerance, and adherence, with a maximum limit of <41 ℃. 17 The circuit water trap was maintained at the lowest possible level to collect condensed water. Ventilator circuits were replaced every 7 days, or earlier if visibly contaminated or malfunctioning. For patients receiving NIV via ICU ventilators, the NIV algorithm function was activated. Both dedicated NIV ventilators and ICU ventilators were operated in either continuous positive airway pressure (CPAP) mode or bilevel positive airway pressure mode. Oronasal masks were the first choice for all patients; if patients experienced discomfort, nasal masks were used as an alternative. Mask size was selected according to the patient’s facial anatomy, and mask straps were adjusted to the tightest possible fit while maintaining patient comfort. Inspiratory pressure was typically maintained between 10 and 20 cmH2O, and expiratory positive airway pressure was maintained between 4 and 10 cmH2O. The FiO2 was adjusted to maintain peripheral capillary oxygen saturation >92%.
Continuous NIV use was recommended during the initial phase of treatment. Once respiratory distress was relieved and oxygenation improved, NIV was administered intermittently until patients achieved complete weaning. However, endotracheal intubation for invasive mechanical ventilation was performed if respiratory failure progressed. The intubation criteria have been described previously, 16 and the decision to intubate was made at the discretion of the attending physician. NIV failure was defined as the need for endotracheal intubation.
The primary outcome was NIV failure in patients receiving NIV via ICU ventilators versus dedicated NIV ventilators. Secondary outcomes included ICU length of stay, hospital length of stay, 28-day mortality, and time from NIV initiation to intubation. Baseline data and underlying diseases were extracted from electronic medical records. Respiratory rate, heart rate, blood pressure, arterial pH, PaO2/FiO2, and PaCO2 were collected before NIV initiation and recorded at 1–2, 12, and 24 h after NIV initiation.
Statistical analysis
Data were analyzed using SPSS (version 25.0; IBM Corp., Armonk, NY, USA) and R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria). Normally distributed continuous variables are presented as mean ± standard deviation, with between-group comparisons conducted using the unpaired Student’s t-test. Nonnormally distributed continuous variables are presented as median and interquartile range (IQR), with between-group comparisons performed using the Mann–Whitney U test. Categorical variables are presented as counts and percentages, with between-group comparisons conducted using the chi-square (χ2) test or Fisher’s exact test, as appropriate. Cox proportional hazards regression was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for NIV failure and 28-day mortality. Furthermore, to examine the potential effect of disease severity, a secondary inferential analysis was conducted involving randomized patient selection, which was adjusted for sequential organ failure assessment (SOFA) score. 18 A two-tailed p < 0.05 was considered statistically significant.
A constrained linear mixed-effects model was used to analyze respiratory rate, heart rate, systolic blood pressure, diastolic blood pressure, arterial pH, and PaO2/FiO2 measured at NIV initiation and at 1–2, 12, and 24 h after NIV initiation. Fixed effects included the treatment group, a quadratic time effect (if applicable), and the treatment–time interaction. Random effects included the time-varying intercept and slope. Within-subjects correlations were modeled using first-order autoregressive errors.
Results
A total of 2118 patients with acute respiratory failure were screened for eligibility (Figure 1). However, 64 patients were excluded due to missing data regarding the type of NIV ventilator used. Ultimately, 2054 patients were enrolled in the study, including 103 in the ICU ventilator group and 1951 in the dedicated NIV ventilator group. In the ICU ventilator group, the Savina 300 (Drägerwerk AG & Co. KGaA, Lübeck, Germany) was the most commonly used device (77.7%), followed by the PB 840 (Medtronic, Dublin, Ireland) (16.5%; Figure 2). In the dedicated NIV ventilator group, the V60 (Philips Respironics, Murrysville, PA, USA) predominated (78.3%), with the BiPAP Vision (Philips Respironics, Murrysville, PA, USA) ranking second (18.5%).

Patient enrollment flowchart.

Distribution of different ventilator types.
Compared with the dedicated NIV ventilator group, patients in the ICU ventilator group had a higher SOFA score, a larger proportion of mixed ICU populations, a higher incidence of cardiogenic pulmonary edema, a lower respiratory rate, and a lower PaO2/FiO2 ratio (Table 1). Trends in respiratory rate, heart rate, systolic blood pressure, diastolic blood pressure, pH, and PaO2/FiO2 from NIV initiation to 24 h postinitiation are summarized in Figure 3.
Demographics.
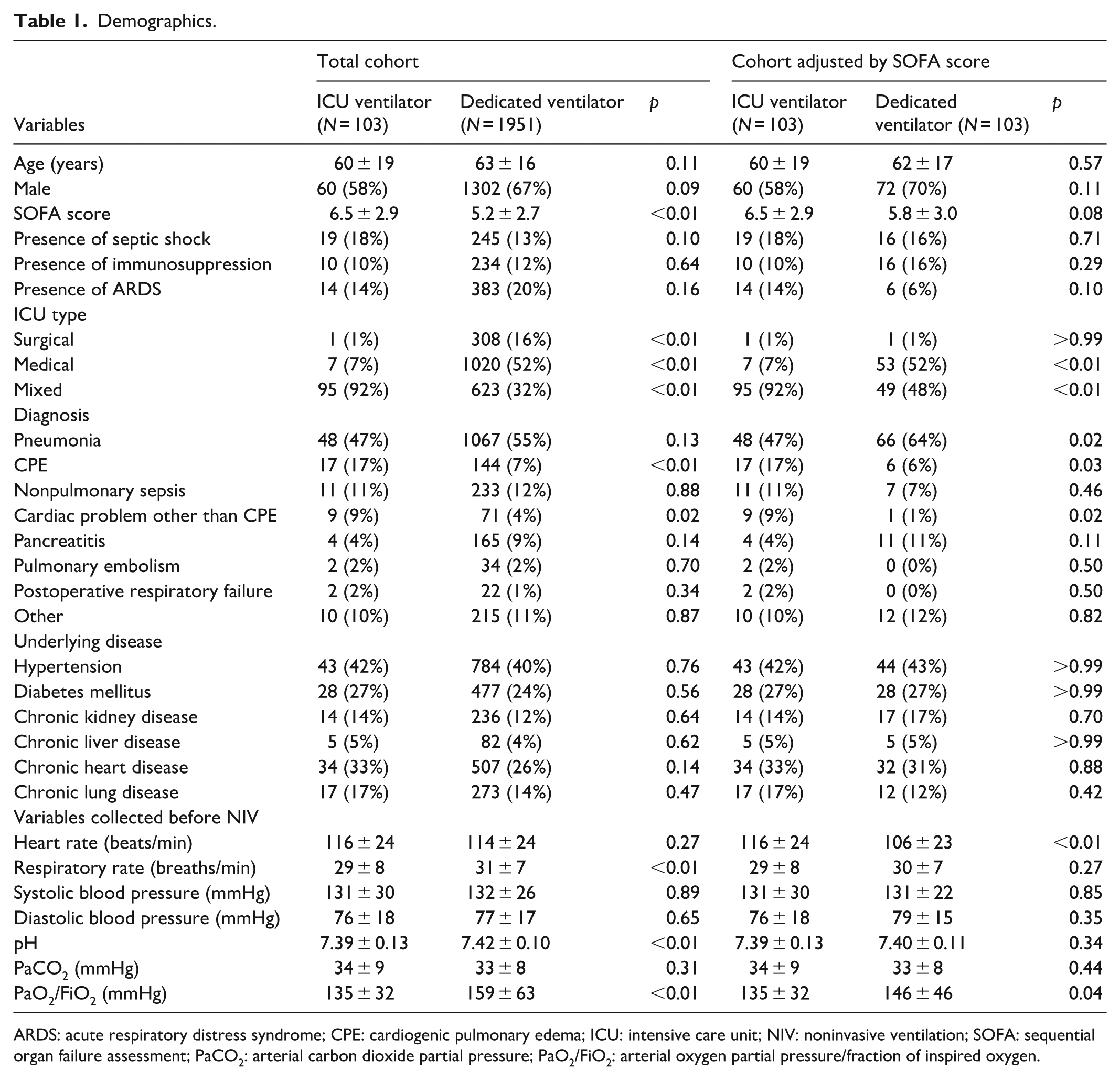
ARDS: acute respiratory distress syndrome; CPE: cardiogenic pulmonary edema; ICU: intensive care unit; NIV: noninvasive ventilation; SOFA: sequential organ failure assessment; PaCO2: arterial carbon dioxide partial pressure; PaO2/FiO2: arterial oxygen partial pressure/fraction of inspired oxygen.

Trends in vital signs and arterial blood gas tests from initiation to 24 h of NIV.
The time from NIV initiation to endotracheal intubation was significantly shorter in the ICU ventilator group than in the dedicated NIV ventilator group (median: 9 h (IQR: 3–25) versus 21 h (IQR: 6–65), p < 0.01; Table 2). The length of ICU stay was also significantly shorter in the ICU ventilator group (median: 6 days (IQR: 3–10) versus 7 days (IQR: 4–12), p < 0.01). However, no significant differences were observed between the two groups in terms of NIV failure rate (46% versus 38%, p = 0.15) and 28-day mortality (16% versus 17%, p = 0.79).
Outcomes.

ICU: intensive care unit; NIV: noninvasive ventilation; SOFA: sequential organ failure assessment.
The cumulative incidence of NIV failure was significantly higher in the ICU ventilator group than in the dedicated NIV ventilator group (log-rank test, p = 0.01; crude HR = 1.43, 95% CI: 1.06–1.91; adjusted HR = 1.41, 95% CI: 1.04–1.93; Figure 4 and Table 3). In contrast, there was no significant difference in 28-day mortality between the two groups (log-rank test, p = 0.65; crude HR = 0.84, 95% CI: 0.52–1.34; adjusted HR = 0.95, 95% CI: 0.58–1.55). Similar trend was found in cohort adjusted by SOFA score (Figure 5).
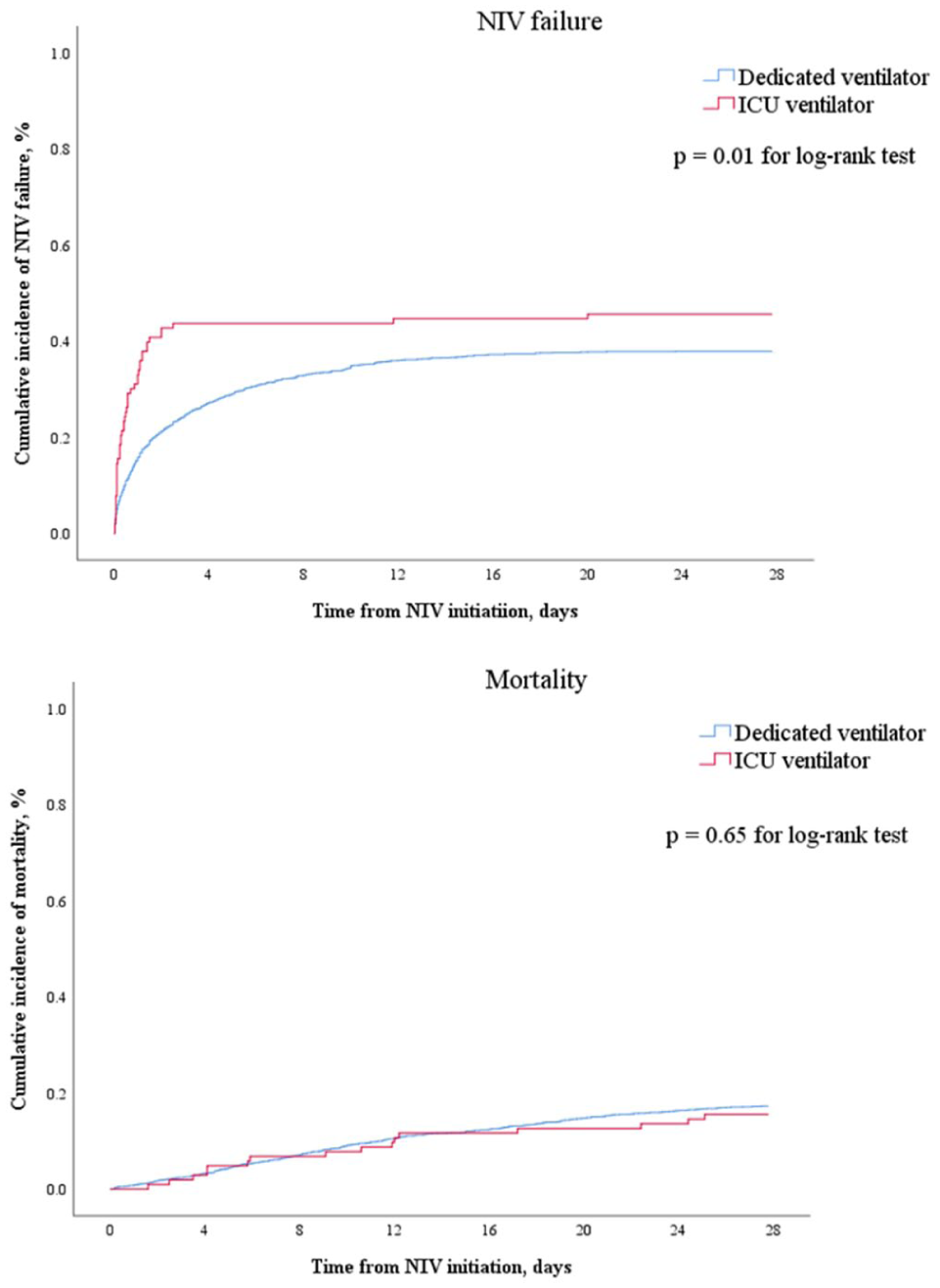
Cumulative incidence of NIV failure and mortality within 28 days in total cohort.
HR of NIV failure and mortality within 28 days in patients with ICU ventilator.

ARDS: acute respiratory distress syndrome; CI: confidence interval; HR: hazard ratio; ICU: intensive care unit; NIV: noninvasive ventilation; SOFA: sequential organ failure assessment; PaCO2: arterial carbon dioxide partial pressure; PaO2/FiO2: arterial oxygen partial pressure/fraction of inspired oxygen.
It was adjusted by age, sex, SOFA score, presence of septic shock, presence of immunosuppression, presence of ARDS, ICU types, diagnosis, underlying disease, and heart rate, respiratory rate, systolic blood pressure, diastolic blood pressure, pH, PaCO2, and PaO2/FiO2 collected before NIV.

Cumulative incidence of NIV failure and mortality within 28 days in cohort adjusted by SOFA score.
Discussion
To the best of our knowledge, this is the first study to conduct a head-to-head comparison of ICU ventilators versus dedicated NIV ventilators for delivering NIV in patients with acute hypoxemic respiratory failure. In China, the use of ICU ventilators for NIV remains uncommon. Patients in the ICU ventilator group underwent endotracheal intubation earlier; however, this was not associated with a difference in 28-day mortality compared with those treated with dedicated NIV ventilators.
A key advantage of ICU ventilators for NIV delivery is their two-limb circuit design, which enables accurate measurement of expiratory tidal volume. In contrast, dedicated NIV ventilators utilize a single-limb circuit, with tidal volume estimated via built-in algorithms 19 —a measurement, that is, highly susceptible to air leakage. Given that tidal volume can reflect patient self-induced lung injury, and higher tidal volumes (especially >9.5 mL/kg of predicted body weight) are associated with an increased risk of NIV failure, 15 accurate monitoring of tidal volume may assist clinicians in determining the optimal timing for endotracheal intubation. Another potential benefit is that ICU ventilators can switch between NIV and invasive ventilation modes using the same two-limb circuit. This feature may improve device utilization efficiency in hospitals and reduce medical costs for patients requiring both ventilation modes.
The most notable disadvantage of ICU ventilators for NIV is patient–ventilator asynchrony. Although ICU ventilators can be equipped with an NIV module to mitigate this issue, some European studies have reported the use of ICU ventilators for NIV without such modules. 20 The use of an NIV module significantly improves patient–ventilator synchrony with ICU ventilators12,21; however, even with this module, synchrony—particularly in terms of auto-triggering—remains inferior to that achieved with dedicated NIV ventilators. 12 This limitation may restrict the widespread adoption of ICU ventilators for NIV.
To date, direct comparisons of clinical outcomes between these two types of NIV devices are limited. A systematic review focusing on de novo acute respiratory failure reported NIV failure rates of 37% in the dedicated NIV group and 39% in the ICU ventilator group. 22 However, these data were aggregated from heterogeneous studies with unreported baseline characteristics, resulting in very low-quality evidence. Consistent with this review, our study found no significant difference in NIV failure rate between the two ventilator types. Notably, however, patients in the ICU ventilator group underwent intubation earlier. As our study was a concurrent analysis, it provides relatively higher-quality evidence in this research field.
This study has several limitations. First, only 17 hospitals in China were included, and this small sample size may not be representative of the overall landscape of NIV practice across the country. Second, the ICU ventilator group primarily used Savina 300 and PB 840 devices, while the dedicated NIV group used V60 and BiPAP Vision ventilators. Given the wide variety of ventilators capable of delivering NIV, future studies should explore the efficacy of NIV across different device models. Third, in both the dedicated NIV group and the ICU ventilator group, the ventilation mode used was either CPAP or bilevel positive airway pressure. However, since we did not record the specific ventilation mode applied to each patient, this oversight may limit the internal and external validity of our study results. Fourth, no sample size calculation was performed, as this was a secondary analysis. Only 103 patients were enrolled in the ICU ventilator group, which may have diminished statistical power.
Conclusions
The use of ICU ventilators for NIV is not common in China. Low-quality evidence suggests that patients treated with ICU ventilators for NIV undergo intubation earlier but that this is not associated with a difference in 28-day mortality compared with those treated with dedicated NIV ventilators.
Footnotes
Acknowledgements
We would like to thank all medical staff for their assistance in patient management and data collection.
Ethical considerations
The Ethics Committee of the First Affiliated Hospital of Chongqing Medical University approved the study protocol (approval no. 2016150).
Consent to participate
For patients experiencing delirium, written informed consent was obtained from their legally authorized representatives.
Author contributions
J.D. conceived the study. J.H. and J.D. managed and analyzed the data, and drafted the article. K.W., W.S., and W.H. participated in patient recruitment and data collection, and revised the article. All authors read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.