
Abstract
Objective
These authors contributed equally to this work.
Methods
Patients with ALI who required NIPPV were prospectively enrolled and randomly divided between three intervention groups: group A was ventilated using a mini-ventilator; groups B and C were ventilated using a complex critical care ventilator using different settings. Clinical parameters were recorded before and after 8 h of mechanical ventilation.
Results
A total of 51 patients with ALI were enrolled in the study. Clinical parameters in groups B and C underwent greater improvements than those in group A. Group C demonstrated the lowest treatment failure rate (23.5%). Failure rates were highest in group A (58.8%).
Conclusion
The findings of this present study suggest that there were more satisfactory clinical outcomes following the treatment of patients with ALI when NIPPV was delivered using a complex critical care ventilator compared with a conventional mini-ventilator.
Keywords
Introduction
Acute lung injury (ALI) and its more severe form, acute respiratory distress syndrome (ARDS), are common and devastating complications that occur during acute illness and following injury. ALI and ARDS are associated with high morbidity and mortality and a long-term decrease in health-related quality of life; 1 they account for a high proportion of intensive care unit (ICU) bed use. Invasive mechanical ventilation through an endotracheal tube is often a life-saving intervention, but it may cause or exacerbate lung damage in patients with ALI/ARDS. 2 A number of complications may occur during invasive mechanical ventilation, such as complications of intubation, ventilator-associated pneumonia (VAP), ventilator-induced lung injury (e.g. barotrauma, volutrauma and biotrauma) and cardiovascular events. 2 Noninvasive positive-pressure mechanical ventilation (NIPPV) delivers a positive pressure support to the lungs without the use of an invasive artificial airway. During the past 15 years, NIPPV has become one of the most important developments in respiratory medicine3,4 and is increasingly being used in many countries. 5 NIPPV can provide a more convenient, comfortable and economic type of ventilation, and has a good safety profile, compared with invasive mechanical ventilation. 6 NIPPV can avoid endotracheal intubation and intubation-related complications, permits patients to eat, drink, talk and expectorate, and has become the standard of care in hypercapnic respiratory failure secondary to chronic obstructive pulmonary disease. 7 The application of noninvasive mechanical ventilation (NIV) in hypoxaemic acute respiratory failure (ARF) has also been an area of research over the last two decades. 8 Although two meta-analyses of randomized controlled trials found no robust evidence to support the role of NIV in hypoxaemic ARF and ALI/ARDS, respectively;9,10 the use of NIV in specific settings of hypoxaemic ARF (e.g. for pneumonia in immunocompromized individuals and following lung resection surgery) has been shown to reduce endotracheal intubation rates and even mortality. 11 Although the role of NIPPV in ALI/ARDS remains controversial, research has indicated that the use of NIV increased tidal volume and decreased the inspiratory muscle effort, with a consequent improvement in dyspnoea and oxygenation status in patients with ALI. 12 A randomized clinical trial showed the benefit of using initial NIV treatment in strictly selected ALI patients. 13
Conventional NIPPV is usually provided by a mini-ventilator using the bilevel positive airway pressure (PAP) mode. The application and outcomes of NIPPV treatment are limited by the function of the machine and other aspects. Compared with the use of mini-ventilators for NIPPV, modern large ICU ventilators have unparalleled advantages because they offer a full range of functions, excellent performance and multiple modes of operation. For example, most mini-ventilators are triggered by a posterior pressure sensor, whereas large ICU ventilators are usually triggered by an anterior flow-rate sensor and are therefore more sensitive. Mini-ventilators are commonly employed to deliver NIV, but they use single-limb tubing that can increase the amount of CO2 rebreathing. However, large ICU ventilators can deliver NIV by double air circuits that can make patients breathe more smoothly and constrain CO2 retention. Large ICU ventilators have a higher ventilating pressure and can give enough tidal volume and minute ventilation volume. Moreover, they have a wider range of ventilation modes that can be used for different types of patients. Our clinical team has achieved satisfactory results in the treatment of ALI by NIPPV delivered using a complex critical care ventilator in clinical practice (personal communication). Therefore, the current study was undertaken to test the hypothesis that there would be better clinical outcomes following the treatment of ALI by NIPPV delivered using a large complex critical care ventilator, compared with a conventional mini-ventilator.
Patients and methods
Study population
The study enrolled consecutive patients who met the ALI diagnostic criteria 14 and were admitted to the Department of Emergency Medicine, the Department of Respiratory Diseases and the surgical ICU (SICU) of the General Hospital of Tianjin Medical University between September 2009 and March 2012. Causes of ALI included severe bacterial or viral infection, trauma (abdominal surgery not included) and pancreatitis. During mechanical ventilation, conventional supportive treatments, anti-infective agents and antishock treatments were simultaneously administered as and when required. The study was approved by the Ethics Committee of the General Hospital of Tianjin Medical University (registration number: IRB2009-2015), and written informed consent was obtained from all patients or their authorized carers/legal guardians.
Study design
This study consisted of a prospective part and a retrospective part. The NIPPV part of the study was prospective, with enrolled patients meeting the following inclusion criteria for ALI patients: (i) willing to accept NIPPV with a disposable full oronasal mask and gastrointestinal decompression if necessary; (ii) respiratory rate >23 breaths/min at the beginning or using ancillary respiratory muscles; (iii) arterial oxygen partial pressure/fraction of inspired oxygen (PaO2/FiO2) <300–350 mmHg in standard nasal cannular oxygen therapy. Delivering NIPPV via a complex critical care ventilator only needs the patient to be able to trigger the flow sensor at a flow rate of 3 l/min, so a more obvious degree of consciousness, synchronized capability, and respiratory intensity and depth were not required.
A subgroup of patients with ALI met the diagnostic criteria for ARDS, 14 therefore to compare the use of a complex critical care ventilator to deliver NIPPV with invasive mechanical ventilation via an endotracheal tube, this study also retrospectively recruited patients with ARDS treated with artificial airway mechanical ventilation. 14 These patients had been treated at the Department of Emergency Medicine, the Department of Respiratory Diseases and the SICU of the General Hospital of Tianjin Medical University between November 2008 and August 2009. These patients did not provide written or verbal informed consent because this part of the study was a retrospective review of case history data, with no treatment intervention.
Mechanical ventilation interventions
For the prospective NIPPV part of the study, enrolled patients were divided randomly into three groups using a random number table at study entry and were ventilated for 8 h continuously according to the schedules described below. The ventilator parameters could be modulated according to the conditions 8 h later.
Group A was treated using a conventional mini-ventilator (BREAS iSleep 22 BIPAP; Breas Medical AB, Mölnlycke, Sweden), a disposable oronasal mask and an auto-bilevel PAP mode, i.e. pressure support ventilation (PSV) + positive end expiratory pressure (PEEP), 7–8 l/min oxygen flow by an infusing tube (FiO2 about 40–50%). The O2 flow rate could be increased when PaO2 <40 mmHg continuously. The high-pressure phase was 15 cmH2O (1 cmH2O = 0.098 kPa); the low-pressure phase was 6 cmH2O, triggered at 2–3 cmH2O.
Group B was treated using a new type of large critical care ventilator (Hamilton Galileo Gold Ventilator; Hamilton Medical AG, Bonaduz, Switzerland), a disposable oronasal mask and a spontaneous mode, i.e. PSV + PEEP. FiO2 was 40–60% and FiO2 could be increased when PaO2 <40 mmHg continuously. The PSV was 9 cmH2O, but 15 cmH2O when plus PEEP, which was 6 cmH2O. The trigger flow-rate was 3 l/min at the anterior extremity. The expiratory trigger sensitivity (ETS) was 45%. The pressure rising time (Pramp) was 25 ms.
Group C was treated using the same new type of large critical care ventilator, a disposable oronasal mask and a Duo PAP mode (Duo PAP + PSV). FiO2 was 40–60% and FiO2 could be increased when PaO2 <40 mmHg continuously. The PSV was 9 cmH2O, but actually 15 cmH2O during the low-pressure phase. The high-pressure phase was 25 cmH2O and the low-pressure phase (PEEP) was 6 cmH2O. The low-pressure phase could be overlapped by PSV. The high-pressure phase time was 1.5 s. The mandatory rate was 10 times per min. The flow-rate trigger was 3 l/min at the anterior extremity; the ETS was 45%, and the Pramp was 25 ms.
Clinical parameters (including respiratory rate, PaO2/FiO2, arterial CO2 partial pressure [PaCO2] and blood pH) were recorded and the Murray ALI score was measured to evaluate the severity of ALI before the initiation of NIPPV. 15 Each patient was asked try their best to expectorate, or a sputum suction tube was used to aspirate any secretions and then the patient was given gastrointestinal decompression. An oropharyngeal tube was used to prevent the tongue root from falling, if necessary. This airway secretion aspiration procedure was performed every 1–2 h as this improves the effects of treatment. Clinical parameters were collected again after 8 h of ventilation. The clinical parameters of groups B and C included oral obstructive pressure at 0.1 s after initiation of inhalation (P0.1), rapid superficial breath (RSB) index, stationary compliance of the lung (Cstat) and inflection point, which were computed and analysed using algorithms and analytical software built-in to the large critical care ventilator. Air leakage from the mask was carefully restricted by adjusting the tighntess of the headband. The pressure was high, to ensure ventilation volume, and gastrointestinal decompression helped to relieve abdominal distension and prevent digestive tract haemorrhage.
The retrospectively enrolled patients with ARDS (retrospective group), who were mechanically ventilated using an artificial airway via the mouth, were treated using the same large critical care ventilator and a Duo PAP + PSV mode. The initial FiO2 was 40–60%, but the ventilation parameters were modulated according to clinical conditions in individual patients.
The treatment was considered to fail after the standard 8 h of ventilation when the patient met any one of the following criteria: (i) cannot tolerate NIPPV; (ii) arterial oxygen saturation <85% or PaO2 <50 mmHg, or arterial oxygen saturation ≥85% or PaO2 ≥50 mmHg but the patient needs >60% of the continuous oxygen concentration during and after the 8 h of treatment; (iii) serious difficulty with expectoration; (iv) aggravating symptoms that were too serious to allow successful ventilation (e.g. spontaneous respiratory rate fewer than five breaths per min, too weak to trigger a breath, low tidal volume); (v) having to establish an artificial airway; (vi) patient’s death.
The inflection point was measured by the pressure–volume tools included within the large critical care ventilator. Although during noninvasive ventilation there was a minor error in calculating the inflection point, recording this information remained valuable. An improvement in the inflection point was defined as: lower inflection point disappeared; lower inflection point enlarged to a steep inflection fragment; the slope rate of the line connecting the upper and lower inflection points increased; the slope rate of the tangent line of the pressure–volume curve across the lower inflection point increased.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 11.5 (SPSS Inc., Chicago, IL, USA) for Windows®. Data are presented as mean ± SD or n of patients. Statistical comparisons of demographic and baseline clinical characteristics and improvements in the clinical parameters among different groups were performed by one-way analysis of variance. Independent-samples t-test was used to compare demographic and baseline clinical characteristics, and total respiratory support times, between group C patients with ARDS and the retrospective group of patients with ARDS. Exact probabilities in a 2 × 2 table were used to analyse the development of VAP and treatment failure between groups. A P-value <0.05 was considered statistically significant.
Results
Demographic and baseline clinical characteristics of patients with acute lung injury (ALI; n = 51), enrolled in a randomized study to evaluate the efficacy of three different types of noninvasive mechanical ventilation.

Data presented as mean ± SD or n of patients.
Measured using the Murray ALI score. 15
PAP, positive airway pressure; PSV, pressure support ventilation; PEEP, positive end expiratory pressure; PaO2/FiO2, arterial oxygen partial pressure/fraction of inspired oxygen; PaCO2, arterial carbon dioxide partial pressure
No statistically significant between-group differences (P ≥ 0.05; one-way analysis of variance).
Demographic and baseline clinical characteristics of patients with acute lung injury (ALI) categorized as having acute respiratory distress syndrome (ARDS; n = 9) compared with a retrospective group of patients with ARDS (n = 9), enrolled to evaluate the efficacy of different types of mechanical ventilation.

Data presented as mean ± SD or n of patients.
Measured using the Murray ALI score. 15
PaO2/FiO2, arterial oxygen partial pressure/fraction of inspired oxygen; PaCO2, arterial carbon dioxide partial pressure.
No statistically significant between-group differences (P ≥ 0.05; independent-samples t-test).
Change from baseline in the clinical characteristics of each group of patients with acute lung injury (ALI) after 8 h ventilation using different types of mechanical device.
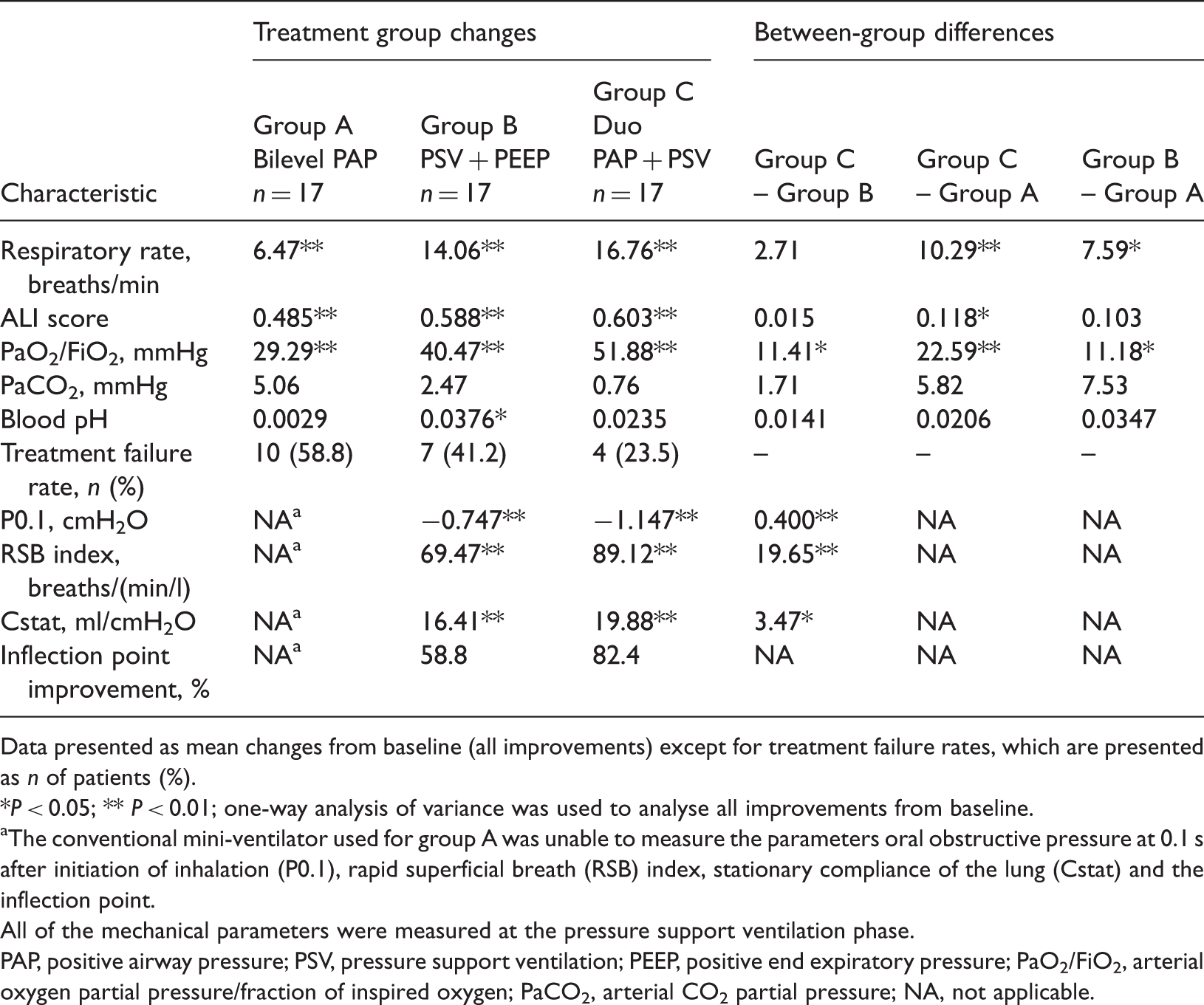
Data presented as mean changes from baseline (all improvements) except for treatment failure rates, which are presented as n of patients (%).
P < 0.05; ** P < 0.01; one-way analysis of variance was used to analyse all improvements from baseline.
The conventional mini-ventilator used for group A was unable to measure the parameters oral obstructive pressure at 0.1 s after initiation of inhalation (P0.1), rapid superficial breath (RSB) index, stationary compliance of the lung (Cstat) and the inflection point.
All of the mechanical parameters were measured at the pressure support ventilation phase.
PAP, positive airway pressure; PSV, pressure support ventilation; PEEP, positive end expiratory pressure; PaO2/FiO2, arterial oxygen partial pressure/fraction of inspired oxygen; PaCO2, arterial CO2 partial pressure; NA, not applicable.
Change from baseline in the clinical characteristics of patients with acute lung injury (ALI) categorized as acute respiratory distress syndrome (ARDS; n = 9) compared with a retrospective group of patients with ARDS (n = 9) after 8 h ventilation with two different types of mechanical device.

Data presented as mean changes from baseline (all improvements) except for ventilator-associated pneumonia (VAP), total respiratory supporting time and treatment failure.
P = 0.012; between-group comparison for VAP; exact probabilities in a 2 × 2 table.
Total respiratory support time was the total time spent on a ventilator for those patients who survived.
P < 0.05; between-group comparison for total respiratory support time; independent-samples t-test.
In the patients from group C with ARDS, treatment failure was when endotracheal intubation was required or death occurred. In the retrospective group, treatment failure was when death occurred or when the patient could not be extubated (a difficult-to-wean patient) and then subsequently died.
P = 0.070; between-group comparison for treatment failure; exact probabilities in a 2 × 2 table.
PaO2/FiO2, arterial oxygen partial pressure/fraction of inspired oxygen; NA, not applicable.
Discussion
This present study enrolled 51 patients with ALI who required mechanical ventilation. A subgroup of nine patients with ALI, randomized to group C, met the diagnostic criteria of ARDS. Consequently, the study retrospectively enrolled a further nine patients with ARDS who were treated with artificial airway mechanical ventilation. The results of this study indicated that delivering NIPPV using a large complex critical care ventilator for patients with ALI was more clinically effective than delivering NIPPV using a conventional mini-ventilator.
Traditional mini-ventilators are usually triggered by a posterior pressure sensor, while the complex critical care ventilator that was used in the present study was triggered by an anterior flow rate sensor, and was therefore more sensitive than the mini-ventilator used in group A. Triggering by an anterior flow rate sensor can decrease the reactive time; 16 in addition, the complex critical care ventilator has an adjustable ETS and Pramp. 17 Mini-ventilators, commonly employed to deliver NIV, use single-limb tubing that can increase the amount of CO2 rebreathing. 18 However, complex critical care ventilators deliver NIV using double air circuits, which can make the patient’s breathing smoother and reduce CO2 retention. Complex critical care ventilators can shorten the inspiration rising time, which decreases the cross product of time and pressure (which is used to estimate the consumption of respiratory work) and increases the initial inspiration flow rate, both of which are efficacious in the inspiratory assistance provided by PSV. In addition, complex critical care ventilators can meet the demands that ALI patients have for a high initial inspiratory flow rate. 19 With a higher ventilating pressure combined with an oropharyngeal airway, complex critical care ventilators can provide adequate tidal volume and minute ventilation volume, and improve the oxygenation of patients. The present study identified better improvements in the oxygenation index (PaO2/FiO2) of groups B and C compared with group A. Complex critical care ventilators do not need to offer a strong matching ability between patients and they can open the upper airway more definitely and attain better synchronization than mini-ventilators. In a multicentre randomized crossover study, Vignaux et al. 20 evaluated the impact of NIV algorithms used by ICU ventilators on the incidence of patient–ventilator asynchrony in 65 patients with acute respiratory failure. The NIV algorithms reduced the incidence of leak-associated asynchronies. 20 They can also reduce the respiratory drive to lower the respiratory work, 21 improve the ventilation/perfusion ratio, open the collapsed alveoli, improve lung compliance and improve the inflection point. In addition, the increasing tidal volume and/or the opening of the alveoli can stimulate the neural reflex to promote respiratory rate normalization. 22 The results of this present study also showed that the lung compliance (Cstat) and the inflection point were improved and central inspiratory drive (P0.1) was decreased, compared with baseline, which were consistent with the viewpoints of the above-mentioned literature. 22 The complex critical care ventilator contains a comprehensive monitor and alarm system that is a patient safety feature. However, NIPPV also has some drawbacks. For example, airway resistance and dead space are more obvious during NIPPV. The parameters and curves measured cannot fully reflect the real situation of the patients because the ventilation tube is not completely sealed.
The high pressure that can be delivered by a large complex critical care ventilator allows operators to use complex modes when ventilating patients. In this present study, the Duo PAP + PSV mode was used in group C to deal with the ‘sponge lung model’ of patients with ALI. Computed tomography scans of lungs with ALI have shown that lung density increases from the ventral to the dorsal part, similar to a sponge soaked with water. 23 The air is progressively extruded out from the basilar lung area, causing compressive atelectasis and consolidation. The Duo PAP + PSV mode allows patients to breathe spontaneously at the alternative two positive pressure levels. Under the Duo PAP mode, there are two alternative positive pressure phases that can produce two functional residual capacities and the difference between the functional residual capacities drives the ventilation of patients. Using the active respiratory valve (which automatically and dynamically assists spontaneous respiration, increases the mean airway pressure and decreases the peak airway pressure), prolongs the high functional residual capacity phase and decreases ventilator-associated injuries. During NIPPV, using the active respiratory valve can reduce pulmonary circulation suppression, open basilar alveoli effectively and ensure spontaneous respiration, and also reduces the use of deep sedation and muscle relaxants.
In the retrospective part of the present study, NIPPV delivered using a complex critical care ventilator demonstrated similar efficacy as conventional artificial airway ventilation in the treatment of a small subgroup of patients with ARDS. These findings suggest that using a complex critical care ventilator to deliver NIPPV could reduce the use of endotracheal intubation. More importantly, delivering NIPPV using a complex critical care ventilator can begin earlier than artificial airway mechanical ventilation and has a wider indication range compared with conventional noninvasive ventilation using a mini-ventilator in clinical practice. 24 Therefore, using a complex critical care ventilator makes it easier for physicians to decide whether or not to use noninvasive mechanical ventilation. For patients with acute hypoxaemic respiratory failure, early selective NIPPV treatment can reduce the need for intubation, reduce the risk of severe complications, improve survival and discharge rate; 11 and is associated with a low incidence of pneumonia and mortality. 25 In addition, patients who accept invasive mechanical ventilation are at risk of emotional stress because they cannot talk; in addition, it is often extremely difficult for them to communicate their needs because of the presence of an endotracheal tube. This stress may negatively impact on ventilator weaning and survival. 26 The delivery of NIPPV using a complex critical care ventilator can relieve such stress because patients can continue to eat, drink, talk and expectorate. In patients who survive following a period of mechanical ventilation, those treated by NIPPV have a shortened ventilation support time, 27 which would be expected to be associated with a lower consumption of medical resources.
This present study had a number of limitations. First, the sample size was relatively small so the evidence should be considered with caution. Future research to investigate the potential usefulness of complex critical care ventilators in the delivery of NIPPV should be undertaken in larger patient populations. Secondly, the two groups of patients with ARDS were not treated during the same time period, so the results may have been affected by bias.
In conclusion, the findings of this present study suggest that more satisfactory clinical outcomes were achieved in the treatment of patients with ALI when NIPPV was delivered using a complex critical care ventilator compared with a conventional mini-ventilator.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by grants from the National Natural Science Foundation of China (grant numbers: 81270144, 30800507, 81170071 and 81100060).