
Abstract
Amyotrophic lateral sclerosis is a neurodegenerative illness that causes gradual loss of muscle function. Patients eventually develop bulbar impairment, requiring extensive respiratory support. Noninvasive ventilation (NIV) has gained attention as an easily accessible method with promising benefits. We conducted this systematic review to outline the therapeutic effects of NIV, add to previous publications discussing this topic by providing updates on newly completed and ongoing studies, and identify limitations that must be addressed in future trials. A search of PubMed and Cochran for relevant primary studies yielded 26 publications. Studies indicate NIV use is associated with improvements in quality of life, regardless of the severity of bulbar impairment. However, NIV’s benefits on survival were limited to patients with less bulbar impairment. In addition, our review found several limitations that undermine the efforts to establish a definitive treatment regimen. Future studies will need to address these problems in order to provide patients with better respiratory care.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease characterized by progressive loss of upper and lower motor neuron functions.
Approximately 16,000 people in the United States were reported to be diagnosed with ALS in 2014, with an estimated prevalence of 5.0 out of 100,000. 1 Although a relatively rare condition, ALS continues to present a heavy burden. The overall median survival is 3–4 years. ALS can be clinically categorized into either limb-onset or bulbar-onset ALS depending on the location of onset. 2 Limb-onset ALS is characterized by gradual loss of function in the skeletal muscles of the limbs. In bulbar-onset ALS, patients experience progressive impairment of the muscles of mastication first, leading to the impairment of swallowing, speech, and respiration.
All types of ALS ultimately result in severe bulbar impairment. The decline in respiratory muscle function leads to increased work of breathing, microatelectasis from retention of mucus, and subsequent decrease in lung compliance. 3 Impairment in swallowing also leads to increased risk of aspiration and subsequent respiratory infection, presenting a potentially lethal threat to ALS patients. Indeed, the most frequent cause of death in ALS patients is respiratory insufficiency secondary to respiratory musculature impairment. 4 –6 Treatment is difficult as no method exists to regain muscle function. Disease progression ultimately leads to ventilation assistance. Although this has traditionally been achieved with invasive ventilation via tracheostomy, several studies highlight its shortcomings. Tracheostomy has been associated with long-term morbidity as well as increased burden of care. 7 Incapacitation of the natural airway defenses, chronic bacterial colonization, swallowing impairment, ineffective tracheal suctioning, inability to generate coughs, and chronic hypocapnia from high ventilator volumes have been discussed in several studies. 8– 20 Noninvasive ventilation (NIV) has emerged as a promising alternative with studies showing increasing use in multiple countries. 21, 22 It has been shown to be easier to use, has adequate therapeutic effect, and is preferred by patients as well as providers. 23 –27 The complications involved with using NIV are minimal, including skin allergies, dry mouth, and irritation from air leakage. However, limited evidence exists for its use in ALS patients with bulbar impairment. We conducted this review with the aim to examine NIV’s effects in ALS patients with a focus on the impact of bulbar impairment on these benefits. We placed particular emphasis on NIV’s effects on quality of life (QoL) and survival as these are the most well-studied outcomes. Another aim of our review is to identify the potential needs for improving current treatment strategies.
Methods
We conducted a systematic review using methods outlined in the Centre for Reviews and Dissemination (https://www.york.ac.uk/crd). Databases including PubMed (https://www.ncbi.nlm.nih.gov/pubmed) and the Cochran Database of Systematic Reviews (https://www.cochranelibrary.com) were used to search for relevant articles from inception to August 28, 2018. We used disease-specific search terms “amyotrophic lateral sclerosis, motor neuron disease, neuromuscular disease” and intervention-specific terms “noninvasive, ventilation.” The online searches were supplemented by scrutinizing reference lists of included articles for additional relevant publications. We also searched for ongoing trials using the website https://www.clinicaltrials.gov.
All selected publications were first screened for relevance according to the abstract and then reviewed in full. Studies were included in the review if they discussed NIV usage in patients diagnosed with ALS. Studies for which full texts could not be obtained, that were not in English, or that did not directly examine data on NIV use in ALS patients were excluded. Based on these criteria study selection was conducted by one investigator. Data on ALS diagnosis criteria, ventilation methods, ventilation initiation criteria, study measurements, and outcomes were collected.
Results
Our initial search produced 227 results. After filtering by exclusion criteria and sorting based on relevance, we found 26 studies that examined the effects of NIV use on ALS patient populations (Figure 1). Meta-analysis could not be performed due to the heterogeneity of the study designs.

Flow diagram of articles collected on NIV use in ALS. NIV: noninvasive ventilation; ALS: amyotrophic lateral sclerosis.
Among these, 8 were retrospective studies 27 –34 and 18 were prospective studies 24,35 – 51 (Table 1). Six studies had control groups, 24,38,39,42,48,49 and only one study was a randomized controlled trial (RCT). 42 The population size in these studies varied from 5 to 140 patients. Although most studies used the El Escorial criteria to confirm the diagnosis of ALS, six studies used unspecified diagnostic criteria. 28,31,32,35,38,42 The criteria for initiating NIV varied significantly among the studies (Table 2).
Type and demographics of analyzed primary studies.
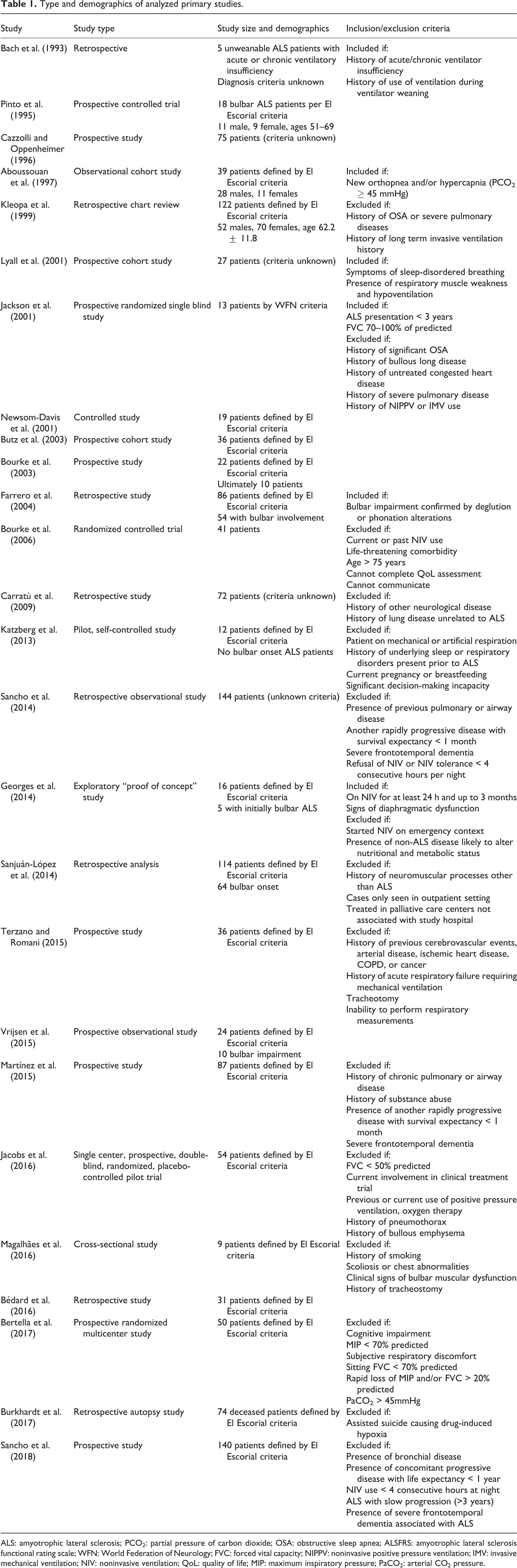
ALS: amyotrophic lateral sclerosis; PCO2: partial pressure of carbon dioxide; OSA: obstructive sleep apnea; ALSFRS: amyotrophic lateral sclerosis functional rating scale; WFN: World Federation of Neurology; FVC: forced vital capacity; NIPPV: noninvasive positive pressure ventilation; IMV: invasive mechanical ventilation; NIV: noninvasive ventilation; QoL: quality of life; MIP: maximum inspiratory pressure; PaCO2: arterial CO2 pressure.
NIV use and initiation criteria.

IPPV: inspiratory positive pressure ventilation; Bipap: bi-level positive airway pressure; O2: oxygen; PCO2: partial pressure of carbon dioxide; FVC: functional vital capacity; NIPPV: noninvasive positive pressure ventilation; ELBG: ear lobe blood gas; PSS: pulmonary symptom scale; NIV: noninvasive ventilation; ABG: arterial blood gas; ESS: Epworth Sleepiness Scores; PaCO2: partial pressure of carbon dioxide in arterial blood; SaO2: saturation of oxygen in arterial blood; AHI: apnea-hypopnea index; PImax: maximum static inspiratory pressure; SNIP: sniff nasal inspiratory pressure; HMV: home mechanical ventilation; EFNS: European Federation of Neurological Societies; PtcCO2: partial pressure of transcutaneous CO2; VC-CMV: volume control continuous mandatory ventilation; IPAP: inspiratory positive airway pressure; EPAP: expiratory positive airway pressure; PEG: percutaneous endoscopic gastrostomy; SpO2: blood oxygen saturation; MAC: mechanically assisted coughing; PCF: peak cough flow.
As each study had different objectives, there was a wide variety in the measurements used to evaluate NIV’s effects in different areas. A summary of the outcomes of these studies is organized in Table 3.
Method of measurement and outcomes.

PCO2: partial pressure of carbon dioxide; ALS: amyotrophic lateral sclerosis; RFT: respiratory function test; Bipap: bi-level positive airway pressure; FVC: functional vital capacity; VC: vital capacity; PO2: partial pressure of oxygen; PFT: pulmonary function test; ABG: arterial blood gas; ALSSS: amyotrophic lateral sclerosis severity scale; SF-36: 36-item short form survey; ALSFRS: amyotrophic lateral sclerosis functional rating scale; ELBG: ear lobe blood gas; ESS: Epworth Sleepiness Scores; ALSFRS-R: amyotrophic lateral sclerosis functional rating scale-respiratory version; SAQLI: modified Calgary Sleep Apnea Quality of Life Index; MIP: maximal inspiratory pressure; MEP: maximal expiratory pressure; PCEF: peak cough expiratory flows; NIPPV: noninvasive positive pressure ventilation; KOLT: Kendrick object learning test; CO2: carbon dioxide; PaO2: partial pressure of oxygen in arterial blood; PaCO2: partial pressure of carbon dioxide in arterial blood; SpO2: peripheral capillary oxygen saturation; QoL: quality of life; PImax: maximum static inspiratory pressure; PEmax: maximum static expiratory pressure; SNIP: sniff nasal inspiratory pressure; CRQ: Chronic Respiratory Disease Questionnaire; AHI: apnea-hypopnea index; MRC: Medical Research Council; HMV: home mechanical ventilation; REM: rapid eye movement; AI: apnea index; HI: hypopnea index; OR: odds ratio; HR: hazard ratio; PiMAX: maximal inspiratory mouth pressure; BMI: body mass index; REESB: resting energy expenditure with spontaneous breathing; V’O2: oxygen consumption; V’CO2: CO2 production; REENIV: resting energy expenditure with NIV; REEpred: predicted resting energy expenditure; ECG: electrocardiogram; FEV1: forced expiratory volume in 1 s; TLC: total lung capacity; PSQI: Pittsburgh Sleep Quality Index; MQoL: McGill quality of Life questionnaire; N1: stage 1 sleep; AAI: arousal-awakening index; N3: stage 3 sleep; SE: sleep efficiency; N2: stage 2 sleep; PtcCO2: partial pressure of transcutaneous CO2; TDI: transitional dyspnea index; PEF: peak expiratory flow; PCF: peak cough flow; MIC: maximum insufflation capacity; ALSAQ-40: amyotrophic lateral sclerosis assessment questionnaire; V cw: chest wall volume; Veicw: chest wall end-inspiratory volume; Veecw: chest wall end-expiratory volume; VE: minute ventilation; V rep%: contribution percentage of pulmonary rib cage; V rca%: contribution percentage of abdominal rib cage; V ab%: contribution percentage of abdomen; VAS: Visual Analogue Scale; PCFMIC: manually assisted peak cough flow; PCFMI-E: mechanically assisted peak cough flow; HR: heart rate; RR: respiratory rate; %sleepSpO2 < 90: percentage of time spent with SpO2 < 90% at night.
Multiple studies have since continued to examine NIV’s effects on ALS patients. However, as statistical analysis was not yet done on data from these studies, we were unable to include them in our analysis. A 12-week, randomized crossover study was conducted to compare standard NIV and low expiratory pressure NIV in ALS patients (NCT01154283). 52 Twenty-eight participants were separated into two groups and given standard inspiratory (IPAP) and expiratory (EPAP) positive airway pressure noninvasive positive pressure ventilation (NIPPV) and IPAP-only NIPPV in differing orders, crossing over at 6 weeks. Eighteen participants completed the study. Results showed participants were able to use the standard bilevel NIPPV for longer hours (49.94 vs. 45.75). However, when asked for preference, more participants preferred the IPAP-only configuration. Changes in difficulty breathing measured by the transitional dyspnea index showed less deterioration with the IPAP-only configuration (−3.14 ± 2.98 vs. −1.21 ± 2.72). QoL as measured by the EuroQol Visual Analogue Scale showed better QoL improvements reported with the IPAP-only configuration (52.86 ± 25.32 vs. 62.79 ± 17.28).
Discussion
All forms of ALS ultimately lead to respiratory failure secondary to bulbar dysfunction. Maintaining adequate ventilation is, therefore, necessary to increase survival and QoL. Below we discuss different parameters assessed in our study related to the use of NIV in the management of ALS.
QoL benefits
NIV has been shown to have significant QoL benefits, regardless of bulbar impairment. Multiple studies demonstrated significant improvements in vitality, daytime sleepiness, and depression with NIV use. Lyall et al. observed significant improvements in the vitality domain of 36-item short form survey (SF-36) with NIV use. 38 Newsom-Davis et al. showed that the use of NIV had positive effects on cognitive function due to improvements in sleep quality. They found significant improvements in list learning over trials (85.58 vs. 100.13, p = 0.017) and Kendrick object learning test (KOLT) raw scores (37.14 vs. 43.00, p = 0.04) with NIV use. Furthermore, NIV groups showed significantly better improvement in performance than the control group in list learning (14.55 vs. −0.59, p = 0.013), list recall (8.95 vs. −9.19, p = 0.026), and KOLT (5.86 vs. −4.0, p = 0.007). 39 Butz et al. reported QoL improvements during the 10 months of NIV use. Sleep quality remained stable throughout the 33-month observation period. 41 Bourke et al. demonstrated large improvements in Epworth Sleepiness Score, SF-36, Chronic Respiratory Disease Questionnaire, and modified Calgary Sleep Apnea Quality of Life Index (SAQLI), with most improvements occurring during the 35 months after initiating treatment using pressure-support NIV in spontaneous/timed mode with various interfaces. Pressures were adjusted for maximum comfort and efficiency with mean IPAP of 15 cmH2O and mean EPAP of 4 cmH2O. 40 Katzberg et al. reported NIV use improved minimum overnight oxygen saturation when compared to baseline (86 ± 4% vs. 79 ± 9%, p = 0.01), with greater change observed during rapid eye movement (REM) (81.2% vs. 87.8%, p = 0.012) than in other sleep stages (83.1% vs. 84.4%, p = 0.46). Time spent below 90% oxygen saturation was also significantly reduced (30% vs. 19%, p < 0.01). 43 Findings from Vrijsen et al. further showed NIV’s benefit in sleep. Both slow-wave sleep (1% vs. 15%, p < 0.05) and REM sleep (9% vs. 18%, p < 0.05) lengthened with NIV use. Arousal-awakening index was also significantly improved (37 vs. 17, p < 0.01). 47
On the other hand, Jackson et al. saw no significant improvement in QoL. No statistically significant improvement was seen in SF-36 or SAQLI with NIV use. 37 In addition, Vrijsen et al. reported that bulbar impairment reduced the improvement from NIV use. Only oxygen saturation during REM sleep was significantly improved after NIV use (33.4% vs. 0.1% peripheral capillary oxygen saturation REM < 90%, p < 0.05). They saw no improvement in respiratory function or sleep structure that they had seen in their patients without bulbar impairment. 47 This discrepancy was possibly from interference with NIV caused by impairments in swallowing and secretion management. 53
Interestingly, a systematic review by Hannan et al. showed only somnolence and fatigue to consistently improve across multiple studies with NIV use. They suggested that the benefits from NIV on QoL were lesser than those previously proposed, possibly due to the rapid progress of the condition negating benefits or a lack of benefit in the first place. 54 QoL may be difficult to assess as there is a wide variety in how patients perceive QoL. 55
Survival
Overall, NIV seems to have beneficial effects on survival in ALS patients. Pinto et al. observed significant improvement in total survival time (22.2% vs. 87.5% survival after 3 years, p < 0.004) and survival from onset of diurnal gas exchange disorders (p < 0.006). 24 Aboussouan et al. showed significant survival benefits in ALS patients who tolerated NIV (relative risk for intolerant vs. tolerant patients 1.72, p = 0.04). 36 Carratù et al. reported survival rates for ALS patients with functional vital capacity (FVC) < 75% who used NIV was significantly better after 1 year than for patients with FVC < 75% who did not (12/16 vs. 4/12, p = 0.02). In addition, they saw no significant difference in survival between the patients who used NIV and the control (12/16 vs. 37/44, p = 0.5). They showed that the median rate of FVC decline was significantly slower with NIV use (1.52 ± 0.3 vs. 2.81 ± 0.8, p < 0.0001). 31 The survival benefits were not different between volume-cycled NIV and pressure-cycled NIV (7.48–22.41 vs. 10.25–19.75 months, p = 0.533). 32 A recent postmortem study by Burkhardt et al. also found that the NIV use have increased the survival significantly (hazard ratio (HR) 0.19, p = 0.01). 34
However, studies that examined the impact of bulbar impairment on survival suggest it may preclude NIV’s beneficial effects. Cazzolli and Oppenheimer reported patients with bulbar impairment could not tolerate NIV, saying NIV did not relieve their respiratory symptoms. Furthermore, patients using NIV died within 2 months of bulbar symptoms onset unless they underwent tracheostomy. 35 Kleopa et al. saw statistically significant improvement in survival that correlated with longer NIV use. The group that used NIV > 4 h/day had better survival rates than the group that used NIV < 4 h/day (35.5 ± 23.6 vs. 29.2 ± 18.8, p = 0.0031), which in turn had better survival rates than the group that did not use NIV (35.5 ± 23.6 vs. 29.5 ± 12.7, p = 0.028). 29 Farrero et al. observed significant survival benefits in patients without bulbar impairment but not in the group with. When compared, the group of patients without bulbar impairment at the start of NIV treatment had better survival (17 ± 4 vs. 35 ± 6 months, p = 0.03). 30 Bourke et al. saw better NIV use associated with better bulbar function (9.3 vs. 3.8 h/day) with further increase in uses in the better bulbar function group as the study progressed. While they saw a median survival benefit of 205 days in the better bulbar function group (p = 0.006), they did not see such benefits in the group with severe impairment. 42 Sancho et al. reported bulbar dysfunction as an accurate predictor of NIV effectiveness (odds ratio 1.07, p = 0.02). 32 Bédard et al.’s retrospective study suggested NIV’s beneficial effects on survival depended on adequate bulbar function as well as adequate cough flow. 33 Sancho et al. also reported that, although patients with bulbar impairment, as measured by Norris scale bulbar subscore, did see significant benefits in survival with NIV use (13 vs. 3 months, p < 0.001), severity of bulbar function was a significant prognostic factor (HR 0.5, p = 0.001) along with time spent with oxygen saturation under 90% (HR 1.12, p = 0.02). 51
Some recent findings suggest a possible explanation behind how bulbar impairment hinders NIV’s beneficial effect on survival. A retrospective analysis of data from 190 patients showed that, after correction for leaks, approximately 40.8% of patients were inadequately ventilated at night. Sixty-seven percent of these cases were due to obstructive events. Inadequate ventilation was correlated with shorter survival. Interestingly, shorter survival was also seen in patients with upper airway obstructive events even when there was no oxygen desaturation. Patients with these upper airway obstructions were also noted to have reduction of ventilator drive. 56 A recent study examined the mechanism behind this phenomenon, named upper airway obstruction with decreased central drive, and attributed these events to the adduction of vocal folds. Sancho et al. suggest this may be due to corticobulbar pathway degeneration and bulbar hyperreflexia. 57
On the other hand, some studies claim bulbar impairment may not have as severe an impact on NIV’s benefits. Aboussouan et al. acknowledged bulbar impairment may be partially responsible for intolerance, but its detrimental effects were limited to discomforts such as mask fit, nasal congestion, or air leaks. In addition, they suggested that several studies that calculated survival times in ALS patients 58– 60 show bulbar symptoms may not have a significant impact on survival. 36 Sanjuán-López et al. reported no significant difference in median survival from initiation of NIV between patients with bulbar impairment and without (30.15 vs. 17.4 months). Instead, they attributed improved survival to prescribed programmed ventilation as opposed to NIV initiation without prior evaluation due to emergency situations (27.1 vs. 14.0 months from ALS onset, p < 0.012; 12.3 vs. 2.8 months from NIV initiation, p < 0.004). 27 Martínez et al. showed NIV tolerance was significantly correlated to median survival (22.0 vs. 6.0 months, p = 0.03), but no significant difference was found in Norris bulbar subscores between the NIV-tolerant patient group and the NIV-intolerant group (29.3 ± 9.2 vs. 24.1 ± 8.1, p = 0.15). Instead, they noted mechanically assisted cough peak flow was the sole significantly different variable between the two groups (4.6 ± 2.1 vs. 3.0 ± 1.2 L/s, p = 0.01). 45
The mechanism behind NIV’s beneficial effects on survival may stem from its effects on the respiratory muscles. ALS patients with bulbar impairment have weak respiratory muscles that need to be constantly strained even at rest. This could lead to permanent damage to muscles which can then be further compounded by hypoxia, continuing a vicious cycle. 61 NIV may be addressing this by providing relief and countering hypoxia. A study by Georges et al. used indirect calorimetry to demonstrate NIV use significantly reduced respiratory energy expenditure (1149.2 vs. 1197.3 kcal/24 h, p = 0.03). This effect was observed both immediately after NIV use and much later. 44 Terzano and Romani showed NIV use significantly reduced decline in lung function. Patients who used NIV had significantly better FVC (43.35 ± 7.78% vs. 38.6 ± 5%, p = 0.02), forced expiratory volume in 1 s (44.8 ± 11.3% vs. 39.87 ± 9.74%, p = 0.05), and maximum static inspiratory pressure (29.4 ± 8.58 vs. 18.18 ± 6.65 cmH2O, p = 0.007) by the end of their observation. 46 Magalhães et al. used optoelectronic plethysmography to show NIV use significantly increased operating lung volumes while not affecting volume distribution. Chest wall volume (0.43 vs. 0.57 L, p = 0.04), end-inspiratory volume (18.37 vs. 18.95 L, p < 0.01), end-expiratory volume (17.94 vs. 18.37 L, p < 0.01), and minute ventilation (6.44 vs. 10.13 L/min, p = 0.03) were significantly better with NIV use. They also noted a significant increase in diaphragmatic velocity and abdominal muscle shortening with NIV use (p = 0.008), suggesting more efficient use of these muscles and possibly explaining the increase in lung volumes. 49 Although their findings were limited to ALS patients without significant bulbar impairment, they provide insight into how NIV helps with respiratory function. Another possible explanation for NIV’s beneficial effects is that it may be improving central respiratory drive and lung compliance.
It is worth noting that a more recent prospective RCT suggested NIV use in ALS patients with FVC ≥ 50% had no benefit in survival. Jacobs et al. reported that, although the active NIV group used NIV 1.5 h longer than the sham NIV group (p = 0.018), there was no significant improvement in median survival (27 vs. 29 months). The only significant improvements they saw with NIV use were in maximum inspiratory pressure (0.58 vs. 1.50, p < 0.001) and maximal expiratory pressure (0.76 vs. 0.13, p = 0.02). 48 While this finding introduces the possibility of using sham NIV for more RCTs in the future, it also questions the suggestion that NIV’s benefits increase with earlier initiation.
NIV initiation criteria
A wide variability in criteria for initiating NIV was observed (Table 2). Multiple studies used subjective symptoms of respiratory insufficiency, such as daytime somnolence, orthopnea, and morning headaches for the initiation of NIV. 29,30,32,36 –42 Among these, orthopnea has been proposed as a reliable measure. Bourke et al. reported that orthopnea was associated with significant sleep disruption and reduced REM sleep, despite the absence of desaturation or daytime hypercapnia. They suggested that orthopnea may be the best predictor of compliance and effectiveness of NIV. 40 The use of more objective measures such as %FVC predicted, continuous oxygen desaturation, bicarbonate level in arterial blood gas (ABG), and sniff nasal inspiratory pressure have been reported as well. 30 –34,36 –40,42 –45,47,48,51,62 Although not utilized in a trial involving ventilator use in ALS patients, venous chloride and bicarbonate were also proposed as a reliable indicator of when to initiate NIV. 63 Many of these studies proposed %FVC predicted was the most accurate measure of respiratory function.
It is important to note, however, the difficult challenges created by the variable nature of ALS. Variable patterns were observed in pulmonary function decline in ALS patients, with studies showing accelerated, decelerated, or steady rate of decline. 64 – 68 This complicates establishing a clear point in pulmonary function decline at which to initiate NIV use. Early recognition of respiratory decline is difficult as the significance of respiratory symptoms such as sleep disorders or dyspnea may be overlooked. 69 In addition, changes in ABG levels occur late in the respiratory impairment, making it difficult for timely detection of impairment. 64 Also, it is difficult to accurately measure respiratory function in ALS patients. As they often perform poorly on pulmonary function tests, it is difficult to gauge the true extent of their pulmonary muscle strength. 70 Interestingly, a recent study suggested the rate of FVC decline in ALS patients is sigmoidal, initially rapid but slow after an inflection point. Panchabhai et al. suggested deceleration of pulmonary function decline is independent of NIV use, and observation of pulmonary function after the inflection may falsely show benefit. 71
Both the American Academy of Neurology (AAN) and the American College of Chest Physicians (ACCP) recommend the use of NIV in the management of ALS patients. 72 –74 AAN recommends NIV be started when FVC < 50% of predicted. 73 ACCP recommends NIV in the presence of hypoventilation symptoms and at least one of the following: partial pressure of carbon dioxide in arterial blood (PaCO2) >45 mmHg, nocturnal oximetry data showing oxygen desaturation <88% for at least 5 continuous minutes, or maximum inspiratory pressure <60 mmH2O. 72 However, no definite criteria yet exist that outline the appropriate time for initiating NIV, appropriate settings, or subsequent measurements of efficacy.
The lack of a consensus in practice criteria leads to a wide variance in study results and causes subsequent misinterpretations. Future studies should aim to establish effective criteria. Moreover, the lack of an established, reliable guideline may be the reason behind the poor adherence to protocol observed in practice. Only 5 of the 20 centers examined were performing routine evaluations with chest physicians. 75 Another evaluation showed less than 10% of 2018 patients with FVC < 40% of predicted were offered NIV. 76 Some studies saw not all patients who fit AAN’s criteria for initiating NIV were offered the option.41, 77 A study of 38 centers in Italy reported patients were offered respiratory assistance only after presenting with respiratory symptoms. 78 The need to provide better respiratory care is just as important as establishing a reliable criteria.
Limitations
Multiple limitations undermine efforts to establish an adequate protocol for ventilation management. The first problem is in the fundamental nature of ALS. Heterogeneity of disease presentation as well as variable rates of progression make it difficult to establish a guideline that uniformly applies to all cases.
Another limitation is in the sheer lack of research done on the subject. As ALS is a rare condition to begin with, only a small number of cases are available for study. Small sample size has been pointed out as a significant limiting factor in several studies. 36 ,37 Also, many recent studies have not been able to report their findings as low recruitment has made it difficult to examine sufficient amounts of data.
In addition, ethical concerns about withholding a simple, noninvasive, and potentially beneficial treatment from patients with a high mortality condition has deterred many researchers from utilizing a control group. Only four of the studies examined in this review utilized a control group, with only one being an RCT. Other studies reviewed charts and used natural history controls. 79 The high mortality and progressive nature of ALS further jeopardize attempts to research. Cazzolli and Oppenheimer’s study saw 16 of 25 NIV users die before the conclusion of the study. 35 In Aboussouan et al.’s study, 29 of 39 research participants died mid-study. 36 Lyall et al. saw 11 NIPPV users die during the study. 38 In Bourke et al.’s 2006 study, only one patient was alive 45 months after randomization. 42 Sanjuan-Lopez et al. saw 106 of 114 patients who met inclusion criteria die by the end of the follow-up period. 27 Bédard et al. saw 24 of their 37 patients die before the study’s conclusion. 33 Such premature exits from the study limit the amount of data available for examination, further hampering efforts to understand and address ALS.
Multidisciplinary approach
As patients develop significant impairments in their ability to communicate as well as maintain nutrition, bulbar impairment in ALS presents a significant challenge regarding intervention. 80, 81 Due to this multifaceted nature of the condition, a multidisciplinary approach may prove beneficial. 82 Multidisciplinary care involving physicians, respiratory therapists, sleep therapists, and dieticians has been shown to decrease the frequency and duration of hospital admissions as well as increase the utilization of palliative care, ventilation support, and percutaneous endoscopic gastrostomy. 83 – 87 It has also been associated with prolonged survival and higher QoL. 84 ,88 Achieving adequate ventilation in the face of progressive bulbar decline is the biggest challenge that will have to be addressed in future studies.
Ongoing studies
A randomized, crossover trial by Lechtzin et al. (NCT00386464) attempted to examine NIV’s effects in ALS patients with mild respiratory involvement. 89 A study in Taiwan by Lee (NCT00958048) also attempted to examine survival benefits of early NIV use. 90 A prospective cohort study by Basner (NCT00537641) attempted to examine whether home NIV delivers adequate breathing support overnight. 91 An RCT by Farrero (NCT01641965) also looked into early NIV use. 92 Unfortunately, none of these studies have yet published their results. Two studies are currently ongoing. A study comparing the current bilevel ventilation in spontaneous/timed mode of NIV with intelligent volume assured pressure support mode in ALS patients is active but not currently recruiting (NCT01746381). 93 A study in Toulouse is attempting to identify predictive factors for initiating NIV in ALS patients (NCT03452618). 94 These will provide more insight into solving the difficult challenge of determining NIV’s beneficial effects in ALS patients.
Conclusion
ALS is a progressive neurodegenerative illness that eventually leads to respiratory impairment. NIV use has been shown to have QoL benefits regardless of the level of bulbar impairment. Benefits on survival negatively correlated with the level of bulbar impairment. Due to several limiting factors, there is a lack of data on this subject. Further examining the pattern of pulmonary function decline in ALS will help guide the assessment of NIV’s effects in future studies. Additional research on the benefits and potential complications of NIV use will also aid in making a more accurate assessment of NIV’s effects as well as in establishing an effective treatment protocol.
Footnotes
Acknowledgements
We would like to thank Dr. Amir Sabouri (Kaiser Permanente Walnut Creek Medical Center) for reviewing the manuscript.
Author contributions
All authors have approved the final article. Research was conducted by Junghyun Kim and Jafar Kafaie, and preparation of the article was done by Junghyun Kim, John Daniel Bireley, Ghazala Hayat, and Jafar Kafaie.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.