
Abstract
BACKGROUND:
Active straight leg-raise (ASLR) is often performed to strengthen abdominal muscles. The correct execution and maximum benefit of the ASLR can be achieved using abdominal hollowing (AH) and abdominal bracing (AB) exercises.
OBJECTIVE:
To compare the effects of AH and AB on transverse abdominis (TrA), internal oblique (IO), and external oblique (EO) thicknesses, as well as on the pelvic rotation angle, in healthy women during active ASLR.
METHODS:
The participants in this study were assigned randomly to either the AH (
RESULTS:
The thickness of the TrA was significantly greater during ASLR with AH than during ASLR with AB (
CONCLUSIONS:
We recommend that AH be performed for the selective contraction of TrA during ASLR, and that AB be performed for the prevention of the pelvic rotation during ASLR. Therefore, AH and AB should be separately done in stabilization exercises.
Introduction
Active straight leg-raise (ASLR) is often performed to strengthen abdominal muscles for the promotion of health and prevention of musculoskeletal disease in healthy people, as well as for rehabilitation in individuals with back and hip pathologies [1, 2]. If the lumbopelvic and hip regions are not stabilized while raising the lower extremity, the pelvis rotates, and the lumbar spine undergoes excessive lordosis [3]. Repeated or sustained pelvic rotation during ASLR or activities of daily living may produce or aggravate low back pain [4, 5, 6]. Therefore, abdominal muscle control is important to prevent excessive lumbo-pelvic motion during lower limb movement.
The abdominal hollowing (AH) and abdominal bracing (AB) maneuvers are commonly used to assess and rehabilitate abdominal muscles [7, 8, 9, 10]. AH involves selective contraction of the transverse abdominis (TrA) and internal oblique abdominis (IO) by pulling the navel towards the vertebra [11]. Furthermore, AH helps prevent excessive lordosis of the lower back and forward incline of the pelvis [12]. In a previous study, Oh et al. [13] reported that prone hip extension with AH resulted in increased muscle activation and reduced anterior pelvic rotation. The use of AH minimizes pelvic motion because it provides internal stabilization of the lumbopelvic region while raising the leg from the ground. Suehiro et al. [14] also showed that, compared with AB, AH can improve the anteroposterior stability of the lumbo-pelvic region during prone hip extension.
In contrast, AB is a method for isometric co-contraction of all muscles in the trunk, which fixes the lumbar spine [15]. AB increases the stability of the vertebrae against sudden perturbations and reduces the movement of the lumbar spine [16]. Liebenson et al. [17] demonstrated that AB can measurably improve the rotational stiffness of the lumbar spine during ASLR. Furthermore, Kim and Kim [18] suggested that, compared with AH, AB results in greater reduction of the angle of pelvic lateral rotation during side-lying hip abduction.
To the best of our knowledge, there have been no published studies comparing the effects of AB and AH on stabilization of the pelvis during ASLR. Therefore, the purpose of this study was to compare the effects of AH and AB on TrA, IO, and external oblique abdominis (EO) thicknesses, as well as on the pelvic rotation angle, in healthy women during ASLR. Investigation of these outcome measures will provide information that is beneficial to clinicians for designing and implementing effective exercise protocols. We hypothesized that performing AB exercises would increase abdominal muscle thicknesses and reduce the pelvic rotation angle during ASLR.
Methods
Participants
This study included 30 healthy women, who were placed in either of two groups: AH (
General characteristics of the subjects (mean
SD)
General characteristics of the subjects (mean
Abbreviation: AH, abdominal hollowing; AB, abdominal bracing; SD, standard deviation.
Ultrasound measurement of abdominal muscles thickness. Abbreviation: TrA, transversus abdominis; IO, internal oblique; EO, external oblique.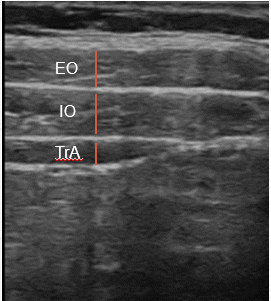
The changes in abdominal muscle thickness of within and between group (unit: mm)
Values are presented as mean (SD). Abbreviation: AH, abdominal hollowing; AB, abdominal bracing; TrA, transverse abdominis; IO, internal oblique; EO, external oblique.
Real time ultrasound imaging (RUSI) measurement of abdominal muscle thickness
Real time ultrasound imaging (RUSI) was performed using the SONON 300L (Healcerion Inc, South Korea) to measure changes in the thicknesses of the TrA, IO, and EO during ASLR with AH or AB (Fig. 1). The instrument was set in B-mode with a 7.5 MHz linear head transducer [19]. The ultrasound transducer was placed transversely across the abdominal wall over the anterior axillary line midway between the 12th rib and the iliac crest to obtain a clear image of the three antero-lateral abdominal muscle layers [20]. Measurements of abdominal thickness were made on the right side of the abdominal wall at the end of expiration during ASLR with AH or AB. Prior to testing, participants were trained by a physiotherapist to ensure they performed the abdominal maneuvers correctly.
Smart phone-based measurement tool (SBMT) measurement of pelvic rotation angle
A smart phone-based measurement tool (Smart KEMA) [21] was used to measure the pelvic rotation angle in the transverse plane during ASLR with AH or AB (Fig. 2).
Measurement of abdominal muscles thickness and pelvic rotation angle using RUSI and SBMT during ASLR with AH and AB. Abbreviation: AH, abdominal hollowing; AB, abdominal bracing; RUSI, Real time ultrasound imaging; SBMT, Smart phone-based measurement tool.
ASLR
Participants were instructed to lay in a supine position on a therapeutic mat with the upper trunk, pelvis, and lower extremity in a straight line. Both arms were crossed across the participant’s chest to prevent them from pushing on the ground with their hands. The dominant leg was flexed at the hip until the heel was 20 cm above the table and maintained contact with the target bar for 5 s [17, 22] (Fig. 2). The dominant leg was determined by asking the participant to kick a soccer ball, with the kicking leg determined to be the dominant leg [23]. All participants were allowed a 5-min rest between test conditions.
ASLR with AH or AB
The participants were asked to gently draw the lower abdominal wall in toward the spine for AH and to tighten their abdominal wall and increase the lateral diameter of the waist for AB [7, 9, 10]. The cursor points measured the muscle thickness between fascial bands during ultrasonography. The image was frozen on the screen and the muscle thickness was measured by the marker (Fig. 1). The ultrasound transducer was not displaced during the testing procedure. The participants performed three abdominal muscles contractions and the mean value of the three measurements was used for further analysis.
Pelvic rotation during ASLR
Measurements of pelvic rotation were made using the SBMT smart phone app to track anterior superior iliac spine placement during ASLR with AH and AB [21] (Fig. 2). Each trial was repeated three times for 5 s each.
Statistical analyses
SPSS Statistics (ver. 18.0, SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Results are presented as mean (standard deviation). The independent
The changes in pelvic rotation angle of within and between group (unit:
)
The changes in pelvic rotation angle of within and between group (unit:
Values are presented as mean (SD). Abbreviation: AH, abdominal hollowing; AB, abdominal bracing.
The changes in abdominal muscle thickness of AH and AB group (unit: mm). Abbreviation: AH, abdominal hollowing; AB, abdominal bracing; TrA, transverse abdominis; IO, internal oblique; EO, external oblique. 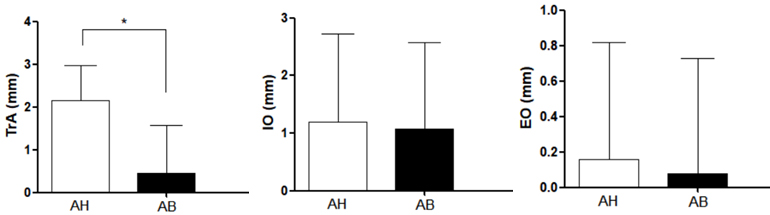
The general characteristics of the participants did not significantly differ between the AH and AB groups (Table 1). In addition, the AH and AB groups did not significantly differ at baseline in terms of abdominal muscle thickness (TrA,
For within-group comparisons, the AH group showed significantly increased TrA (
The changes in pelvic rotation angle of AH and AB group (unit: 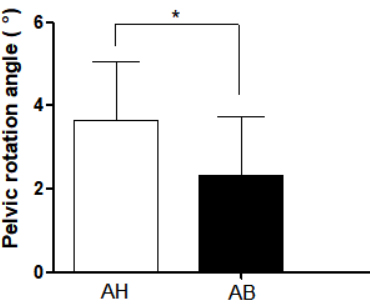
For between-group comparisons, only TrA (
The purpose of this study was to investigate the effects of AH and AB on abdominal muscle thicknesses and pelvic rotation angle during ASLR.
AH and AB are widely used in lumbo-pelvic stabilization exercises. In AH, the abdomen is drawn in without any motion of the lumbo-pelvis. In contrast, AB is performed by tightening the abdominal wall and increasing the lateral diameter of the waist [7, 8, 9, 10]. In this study, AH and AB were compared to obtain clinically important information and evidence for stabilizing the lumbo-pelvic region during limb movement.
In this study, AB significantly reduced the pelvic rotation angle, compared to AH, while performing ASLR. AB is presumed to provide increased stability in all directions and in various types of movements by promoting spinal stiffness. This includes providing stability to the lumbo-pelvic region during various movements which is beneficial during ASLR. In a previous study comparing trunk stability between AB and AH, Vera-Garcia et al. [16] showed that AH was inefficient for reducing fluctuations caused by sudden movements, while AB increased trunk stability by reducing lumbar lordosis. These findings indicated that AB training, but not TrA training, could be more effective for reducing pelvic rotation angle. Therefore, AB during ASLR is presumably a more efficient approach to prevent pelvic rotation.
However, the thickness of the TrA was significantly less during ASLR-AB than ASLR-AH, potentially due to TrA’s activity. The TrA originates on the inner part of the lower thorax and inserts on the iliac crest. It functions in combination with other abdominal muscles to aid in a variety of movements [24]. Although the lower part of the TrA is presumed to affect stability, it may not be related to rotation. Hicks et al. [25] suggested that there was a lack of evidence indicating that the selective contraction of local muscles stabilized the trunk. It is also questionable whether a single muscle can create lumbar stability and aid functional movement [26]; notably, the TrA, which contributes 2% of the maximum isometric contraction of the trunk muscles, acts as an agonist with the IO [27]. In addition, recent studies suggest that selective activation of the TrA alone reduces the efficiency of overall trunk stability, which results in a need for global abdominal muscle activation to achieve balance [28]. Based on this information, overall contraction of the abdominal muscles may be more suitable, relative to selective contraction of the TrA, for trunk stability during ASLR.
Queiroz et al. [29] reported that the IO muscle had a greater role in controlling the lumbo-pelvic position than the EO muscle. The IO contributes to lumbo-pelvic stability by controlling the intra-abdominal pressure and creating tension in the thoracolumbar fascia [30, 31, 32]. In the present study, IO thickness increased after ASLR-AH, but this was not expressed by a significant difference after ASLR-AB. The results of the present study and the previous ones show that IO thickness contribution to lumbo-pelvic stabilization may be increased with ASLR-AH. As for EO thickness, there was no apparent difference after both ASLR-AH and ASLR-AB. This indicates that the EO does play a role in trunk stability during limb movement.
Currently, trunk stabilization exercise is commonly used in clinical practice, applying various approaches. Among them, AH and AB are widely used for lumbo-pelvic stabilization. These two methods, however, are different from each other. The results of this study show that AH is more effective than AB for contracting the local muscles, including the TrA and IO muscles. However, when a large load is applied to the limbs, the excessive motion of the lumbo-pelvis segment cannot be restricted by contracting only the local muscles. In this case, AB may be effective for preventing excessive motion of the lumbar spine or pelvis. In the clinical setting, AH and AB may be used separately according to the external load. For this reason, this study maybe of clinical significance as it compares the thicknesses of the abdominal muscles after ASLR-AH and after ASLR-AB.
This study had several limitations. First, because this study focused on healthy female adults, it may be difficult to generalize the results to other populations. Second, we could not confirm whether the muscular activity was bilateral. Finally, due to the cross-sectional study design, we could not determine whether AB would have been appropriate for long-term improvement of ASLR.
Conclusions
We suggest that AH is more effective than AB for increasing the TrA thickness during ASLR. Our findings also suggest that AB can reduce the pelvic rotation angle during ASLR. Therefore, ASLR-AH can be used for the selective contraction of the TrA while ASLR-AB is recommended for preventing unwanted pelvic rotation motion.
Author contributions
All authors contributed equally.
Ethical considerations
Ethics approval for this study protocol was obtained from Inje University (INJE 2019-02-006-002) and written informed consent was obtained from all participants before the commencement of data collection.
Funding
This work was supported by the 2019 Inje University research grant.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None declared. Given his role as an Editorial Board Member, Jaeseop Oh had no involvement nor access to information regarding the peer review of this article.