
Abstract
BACKGROUND:
The squat exercise is frequently used to develop muscle strength of the lower back, hip, and knee regions to improve physical performance.
OBJECTIVE:
To investigate the effects of squat exercises involving three types of isometric hip contractions and two types of wall conditions on the thickness of abdominal muscles in college athletes.
METHODS:
Twenty-seven college athletes, 17 men and 10 women, took part in the study. Subjects performed the standard squat without hip contraction, the isometric hip adduction squat, and the isometric hip abduction squat with and without using a wall. Abdominal thickness was measured with an ultrasound and presented as muscle thickness ratio.
RESULTS:
The transversus abdominis (TrA) and internal oblique (IO) thickness ratio was significantly greater during the isometric hip adduction squat exercise compared to the standard and isometric hip abduction squat exercises. The TrA and IO thickness ratio in the isometric hip abduction squat exercise was significantly higher than that in the standard squat exercise. The external oblique (EO) thickness ratio was significantly higher in the squat exercise without wall compared to the squat exercise with wall.
CONCLUSIONS:
Isometric hip adduction squat exercise may be an effective method for increasing the TrA and IO thickness ratio while performing the squat exercise without wall may help increase the EO thickness ratio.
Introduction
The squat exercise can be used to develop lower limb muscle strength by activating the quadricep, hamstring, gastrocnemius, and gluteus maximus muscles [1]. It requires effective recruitment of not only the hip and ankle joint muscles but also the abdominal and spinal erector muscles [2]. To develop muscle strength of the lower back, hip, and knee regions to improve physical performance, the squat exercise is frequently used in a number of sports as well as in daily life. In the clinic, it is used as an effective exercise to enhance the strength of the muscles of the lower limbs in rehabilitation programs after surgery [1, 3], because it can mobilize a number of muscle groups with a single motion [4]. However, incorrect exercise performance or inappropriate exercise prescription during squats can cause serious damage such as ruptured intervertebral discs, spondylolysis, spondylolisthesis in the trunk, and ligament sprains in the hip and knee joints [5].
Core stability is a critical factor for the prevention of lower back injury during the squat exercise, and is defined as the ability of the lumbo-pelvic-hip complex to recover balance from body perturbations and to prevent buckling of the spinal column [6]. The spinal column has an unstable structure, and maintaining its stability requires active muscle contraction that is adequately controlled by the central nervous system [7]. By instantly responding to changes in posture and loading, anatomical structures involved in the core provide stability to the trunk when the extremities move [8]. Muscles involved in the core stability include the multifidus, diaphragm, deep abdominal muscles, and pelvic floor muscle, which increase intra-abdominal pressure and global trunk stiffness [9]. Moreover, an increase in the intra-abdominal pressure increases spinal column stability by reducing compressive loading on the spine [10].
Hodges and Richardson [11] reported that the trunk muscles act in a feed-forward mechanism to cause automatic neuromuscular control as anticipatory postural adjustments during movement of the lower limbs regardless of direction. In particular, the transversus abdominis (TrA) is the first muscle to contract among the deep abdominal muscles. The authors compared the onset time of TrA between healthy adults and patients with lower back pain and reported that TrA contraction was markedly delayed during movement of the extremities in patients with lower back pain [11].
Previous studies on the squat exercise have mainly involved changes in activation of the trunk and lower limb muscles, as measured by surface electromyography (EMG). Lander et al. [12] reported that wearing weight belts during squats decreases trunk muscle activation and increases intra-abdominal pressure. Hanten et al. [13] reported that isometric contraction of the hip adductors facilitates activity of the vastus medialis oblique muscle. However, Boling et al. [14] reported that dynamic hip adduction during the squat exercise resulted in no significant change in the EMG amplitude of the vastus medialis oblique muscle. Irish et al. [15] found that reduced activity of the vastus medialis muscle caused patellar maltracking. Cho [3] applied that modified wall squat exercises and an abdominal drawing-in method during the bridge exercise, and reported that both methods caused a significant change in the thickness of the deep abdominal muscle. In the clinic, the squat exercise is used in diverse forms to develop the strength of the lower limbs and trunk muscles. However, few studies have investigated changes in the thickness of the deep abdominal muscles, which stabilize the trunk during squat exercises. The most effective method was identified by measuring changes in the thickness of the deep abdominal muscles according to the different types of isometric hip contractions and the application of the squat exercise both with and without the use of walls.
Therefore the aim of this study was to investigate the effects of squat exercises involving three types of isometric hip contractions (standard squat without hip contraction, isometric hip adduction squat, and isometric hip abduction squat) and two types of wall conditions (with and without wall) on the thickness of abdominal muscles using real-time ultrasound imaging (USI) in college athletes.
Method
Subjects
Twenty seven college athletes, 17 men and 10 women, participated in the study. The inclusion criteria were no history of knee lesions or knee or lower-limb surgery [16], and no current knee pain [17]. The exclusion criteria were any experience of lumbo-pelvic, hip joint, or femoral pain, or hospital visits due to pain within the last year [18]. We recruited 30 subjects at the beginning of the study. Three subjects were not satisfied with the inclusion criteria of this study. Finally, who met the inclusion criteria participated in this study. Each subject signed an informed consent form, and the rights of each subject were protected. The research protocol was approved by the Yonsei University Wonju Institutional Review Board (Certification number: #1041849-201504-BM-043-01). Table 1 describes the general characteristics of the subjects.
General characteristics of the subjects
General characteristics of the subjects
Abbreviations: BMI, body mass index.
To image the abdominal muscles, a 25 Hz com- puterized ultrasound (ultrasound sonography-SonoAce X8, Medison Co Ltd, Seoul, Korea) was used with a 50 mm 7.5 MHz linear array probe. All of the subjects who participated in the experiment had a dominant right lower extremity (i.e., the side used when kicking a ball). Hence, the right lateral deep abdominal muscle was visualized by ultrasound. The location of the probe was suggested by Rankin et al. [19], where the location is immediately below the rib cage, indirect vertical alignment with the anterior superior iliac spine (ASIS). During the test session, the probe location was marked on the skin with a marker pen to allow for identical measurements [20]. To minimize measurement error, two measurers received 20 min training on the ultrasound technique before measuring muscle thickness, which included accurate probe location, major anatomic landmark location, pressure application, and location of the cursor indication [21]. During the measurements, the two measurers worked together, one recording and the other performing the imaging. The imager located the probe in the spot where the muscle structure was most visible [22] and the recorder stored the image. For relative reliability of the measurements, the intraclass correlation coefficient (ICC) was used to analyze the thicknesses of the TrA, internal oblique (IO), and EO at rest (TrA ICC
Three squat exercise with and without wall. A, standard squat exercise with wall; B, standard squat exercise without wall; C, isometric hip adduction squat exercise with wall; D, isometric hip adduction squat exercise without wall; E, isometric hip abduction squat exercise with wall; F, isometric hip abduction squat exercise without wall.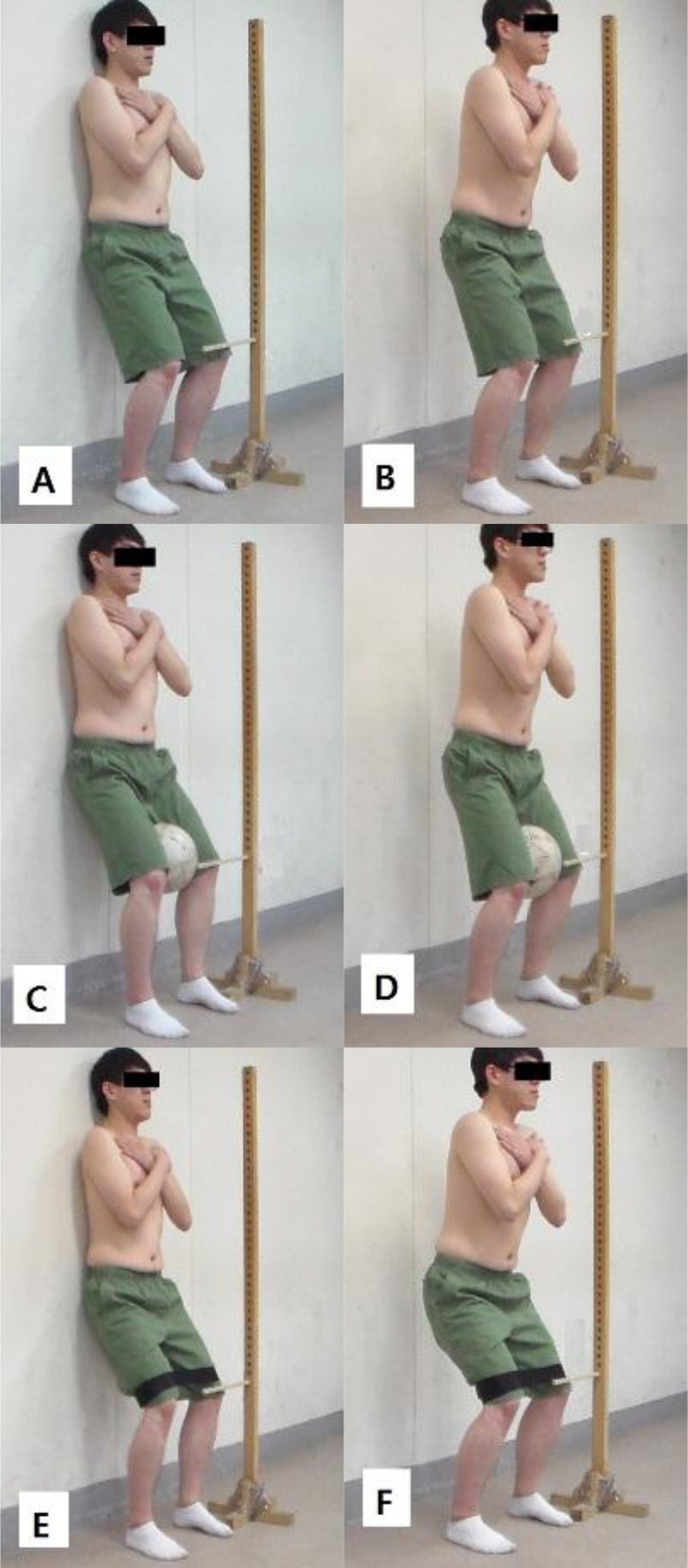
The study participants were allowed to familiarize themselves with the three squat exercises for 10 min before data collection. During the measurement, a 30 s rest period was given between repetitions of three squat exercises. Before the next squat exercise, a 2 min rest period was given to minimize muscle fatigue. The subjects performed squat exercises, including three types of isometric hip contractions (standard squat without hip contraction, isometric hip adduction squat, and isometric hip abduction squat) with two types of wall conditions (with and without wall) (Fig. 1). The order of the exercises and the wall conditions was randomly determined by drawing straws. The subjects performed the squat exercises while maintaining vertical alignment of the knee and toe with 60 degrees of knee. The target bar was located vertically to prevent valgus collapse. The measurer confirmed the 60 degrees of knee flexion using a goniometer, and positioned the target bar so that the right patella of the subjects was just touching it. To prevent compensation movements of the knee during the squat exercise, the heel and big toe of the subjects were aligned with tape attached to the ground.
Standard squat exercise
The subjects widened their legs to shoulder width with straight knees in a standing position. They were asked to keep their pelvis in a neutral position, to fold their arms, and to look forward during the squat. Then they bent their knees down to 60 degrees in 2 s. At the 60-degree knee flexion, the subjects maintained their posture for 5 s and resumed the initial position in 2 s. Three repetitions were performed, and the duration of the exercise was 9 s. The timing was checked using a metronome [23].
Isometric hip adduction squat exercise
The posture and method were the same as the standard squat exercise. A hard ball with a diameter of 22 cm was located on the medial femoral epicondyle. The subjects bent their knees down to 60 degrees in 2 s. At 60-degree knee flexion, the subjects maintained the maximum isometric adduction of the hip joint for 5 s and resumed the initial position in 2 s [14]. Three repetitions were performed, and the duration of the exercise was 9 s.
Isometric hip abduction squat exercise
The posture and method were the same as the standard squat exercise. A non-contraction band (OMPT Manual Belt, COREBODY, Namyangju, Korea) was placed on the lateral femoral epicondyle. The subjects bent their knees down to 60 degrees in 2 s. At 60-degree knee flexion, the subjects maintained the maximum isometric abduction of the hip joint for 5 s and resumed the initial position in 2 s [17]. Three repetitions were performed, and the duration of the exercise was 9 s.
Data collation
USI of the thickness of the deep abdominal muscles were directly collected at the end of inspiration at rest, and measured along a horizontal reference line located 2 cm from the medial edge of the TrA in the captured image [20] (Fig. 2). To investigate the relative muscle thickness, the average of the three images, determined by measuring the thicknesses of the TrA, IO, and EO in the three squat exercises, was divided by the resting average (e.g., TrA thickness ratio
Descriptive statistics of mean muscle thickness ratio for all exercise types and wall conditions
Descriptive statistics of mean muscle thickness ratio for all exercise types and wall conditions
Abbreviations: TrA, transversus abdominis; IO, internal oblique; EO, external oblique; A, standard squat exercise with wall; B, standard squat exercise without wall; C, isometric hip adduction squat exercise with wall; D, isometric hip adduction squat exercise without wall; E, isometric hip abduction squat exercise with wall; F, isometric hip abduction squat exercise without wall.
Deep abdominal muscles. TrA, transversus abdominis; IO, internal oblique; EO, external oblique.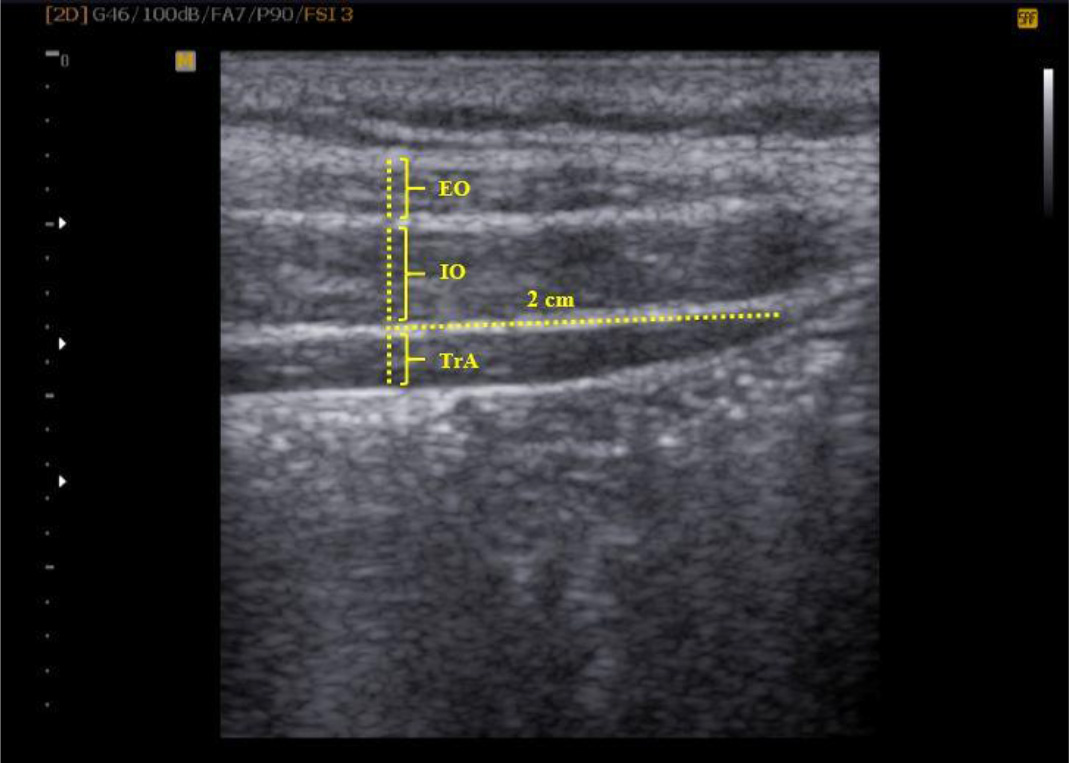
Results of two-way repeated ANOVA on muscle thickness ratio
Abbreviations: TrA, transversus abdominis; IO, internal oblique; EO, external oblique;
Post hoc comparisons of the muscle thickness ratio
Abbreviations: TrA, transversus abdominis; IO, internal oblique; EO, external oblique; ST, standard squat exercise; AD, isometric hip adduction squat exercise; AB, isometric hip abduction squat exercise; W, wall; WO, without wall;
Two-way repeated analyses of variance (ANOVA) with two within-subject factors (exercise types: standard squat exercise, isometric hip adduction squat exercise, isometric hip abduction squat exercise; wall conditions: with wall, without wall) were used to assess the statistical significance of the TrA, IO, and EO thickness ratios. The statistical significance level was set at
Results
The descriptive statistics of the mean muscle thickness ratio for each exercise type and wall condition are presented in Table 2.
TrA thickness ratio
There was no significant interaction effect between the exercise types and the wall conditions in the TrA thickness ratio (
IO thickness ratio
There was no significant interaction effect between the exercise types and the wall conditions in the IO thickness ratio (
EO thickness ratio
There was no significant interaction effect between the exercise types and the wall conditions in the EO thickness ratio (
Discussion
We investigated the most effective method of increasing the deep abdominal thickness ratio from isometric hip contractions during the squat exercise. The TrA and IO thickness ratio was greater in the isometric hip adduction squat exercise than in the isometric hip abduction and standard squat exercises. There were no differences in EO thickness ratio with exercise types, nor were there differences in the TrA and IO thickness ratio when the wall was incorporated into the exercise. The EO thickness ratio increased without incorporation of the wall. The TrA and IO thickness ratio according to exercise types supported the hypotheses of this study, but this was not the case for the EO thickness ratio. The TrA and IO muscle thickness ratio when incorporating the wall into the exercise did not support the hypotheses of this study. However, there was support for EO muscle thickness ratio when the wall was incorporated.
The TrA and IO thickness ratios were significantly greater during the isometric hip adduction squat compared to the isometric hip abduction and standard squat. The hip adductors are linked to the deep abdominal muscles to support or fix them, and to promote their contraction [25]. Contraction of the deep abdominal muscles is critical for stabilizing the pelvic muscles against the pulling force of the hip muscles [26]. When the pelvic muscle is stable, the forces on the trunk are efficiently transmitted to the hip joint and lower extremities [27]. Thorborg et al. [28] showed that the isometric hip adduction torque was greater than the isometric hip abduction torque in elite soccer players. During the isometric hip adduction squat, the spine and lumbo-pelvic muscles co-contract, particularly the TrA that originates in the iliac crest and pulls the ilium in the transversus direction of the spine [29]. Contraction of the TrA generates a rigid cylinder ventrally in the abdominal cavity [30], resulting in enhanced stiffness of the lumbar spine and increased trunk stability. Hence, the isometric hip adduction squat may contribute to the increase in deep abdominal muscle thickness compared to the increase observed after isometric hip abduction and standard squat exercises.
The TrA and IO thickness ratio was significantly greater during the isometric hip abduction squat compared to the standard squat. The gluteus medius, gluteus minimus, and quadrature lumborum are the major lateral muscles of the hip and trunk on the frontal plane. The gluteus medius and minimus act as a primary lateral stabilizer of the hip joint. Although they play a role in hip joint abduction in the open chain, they maintain the pelvis during the stance phase in a closed chain [8]. The gluteus medius and minimus have an appropriate structure to stabilize the trunk during upright activities [31]. Hence, it is thought that they affect the change in thickness of the trunk core muscle of the TrA and IO during the isometric hip abduction squat.
The EO thickness ratio did not significantly differ in the three squat exercises. However, it significantly increased in the squat exercise without using wall compared to using wall. The EO is a superficial muscle among the abdominal muscle group that is not significantly related to core stability. Hence, it may be consistent with overall thickness regardless of the isometric hip abduction and adduction types. Moreover, in our study, the EO was activated less when the squat exercise was performed using wall, as lumbar stability was provided. Lehman et al. [32] reported that activation of the rectus abdominis and EO significantly increased compared to the IO and erector spinae muscle in unstable conditions, such as the use of the Swiss ball during the prone bridging exercise, rather than in stable conditions. Imai et al. [33] reported that exercise on an unstable surface such as BOSU during lumbar stabilization exercises increased the demand of global abdominal muscles. In particular, increased muscle activation of a superficial muscle, such as the EO, decreased the muscle activation of deep muscles such as the TrA [33]. In our study, the squat exercise without incorporating the wall led to a more unstable condition than the exercise using wall, suggesting that the unstable condition affected the change in EO muscle thickness ratio when using wall.
The clinical applications of this study are as follows. Squat exercises were used to strengthen the knee, hip, and deep abdominal muscles. In the rehabilitative center or gym, balls and bands were easy to obtain as exercise props. Using these props during squat exercise can selectively change the thickness ratio of the deep abdominal muscles. The results of this study showed that the TrA and IO thickness ratio increased significantly during the isometric hip adduction squat exercise, and the EO thickness ratio showed a significant increase in muscle thickness in the squat exercise without incorporation of the wall compared to the squat exercise using the wall. Therefore, clinicians and athletic trainers are advised that various squat exercises should be considered to improve selectively the thickness ratio of deep abdominal muscles.
This study had several limitations. First, our findings were limited to a young healthy population, and as such, the results cannot be extrapolated to the general population, including older or symptomatic populations. Second, we examined the change in the deep abdominal muscle thickness in three squat exercises using a cross-sectional design. Additional studies are needed to examine the impact of these three types of squat exercises on the change in deep abdominal muscles using a longitudinal design. Finally, it is necessary to examine the effects of applying these three squat exercises on the change in deep abdominal muscle thickness in patients with lower back pain.
Conclusion
We investigated the most effective method for increasing deep abdominal muscle thickness by measuring the changes caused by isometric hip contraction and application of the squat exercise with and without incorporation of the wall. The TrA and IO thickness ratio showed a significant increase in muscle thickness when isometric hip adduction squat exercise was performed compared to the isometric hip abduction and standard squat exercises. The EO thickness ratio showed a significant increase in muscle thickness in the squat exercise without incorporation of the wall compared to the squat exercise using wall. Based on these, clinicians and athletic trainers should consider incorporating the isometric hip adduction squat exercise, as it is as an effective method for increasing the TrA and IO thickness ratio. In addition, the squat exercise without incorporation of the wall may be used as an effective exercise for increasing the EO thickness ratio.
Conflict of interest
The authors declare no conflicts of interest associated with this publication. The support for this project did not bias its outcomes in any way.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2015R1D1A1A01057620).