
Abstract
BACKGROUND:
Abdominal stabilization is an important factor during hip extension. Additionally, the prone standing position is a more effective and functional position for hip extension than the prone or supine positions.
OBJECTIVE:
To determine the concentric isokinetic strength of the hip extensors during prone standing hip extension (PSHE) using stabilization maneuvers such as abdominal resting (AR), abdominal bracing (AB), and abdominal hollowing (AH).
METHODS:
Thirty one healthy subjects were recruited for this study. In each of the 3 maneuvers the participants performed concentric isokinetic hip extensions, 4 at 60
RESULTS:
Hip extension strength, as indicated by the PM, differed significantly among the three conditions at both velocities (
CONCLUSIONS:
Prone standing hip extension with AB at 60
Introduction
The hip extensors provide stability to the pelvis [1] and play a particularly important role in many activities of daily living, including sit-to-stand, climbing stairs, and maintaining an upright posture during walking [2]. Inappropriate onset timing and weakness of the hip extensor muscles during gait results in decreased shock absorption at the sacroiliac joint [3, 4] and subsequent instability of the lumbopelvic region.
Active hip extension exercises in the prone position are performed primarily in a rehabilitation setting to strengthen the hip extensor muscles [5]. However, in individuals with lumbopelvic instability, prone hip extension may lead to severe back pain caused by undue stress and compression of the vertebrae due to excessive extension and rotation of the lumbar spine as well as anterior tilt and rotation of the pelvis [6, 7, 8]. In addition, individuals with low back pain (LBP) or lumbopelvic instability tend to have weaker hip extensors than healthy individuals due to over-activity of the erector spinae (ES) and hamstring muscles [9]. As a result, these individuals need to strengthen their hip extensors without causing back pain.
It has been suggested that the prone position does not allow as great a muscle contraction as the prone standing position [10, 11]. In the prone standing position, the hip is flexed and the hip extensor muscle fibers and lever arm are lengthened, allowing for a more favorable length-tension relationship and thus optimizing hip extension moment production [12]. Comerford and Mottram first proposed the prone table hip extension test as a method to co-activate the gluteus maximus and abdominal muscles, which are used to control the lumbar spine and pelvis. This posture is performed while the trunk is supported on the table, with both feet placed firmly on the floor and the lumbar spine in a neutral position [13]. Therefore, the prone standing position may be a more effective and functional position for hip extension than the prone or supine position [14].
Stabilization of the lumbopelvic region during hip extension is an important factor to prevent LBP. Kahlaee et al. reported that lumbar stabilization exercises during prone hip extension altered the delayed onset timing of muscle contractions and reduced stress on the vertebrae by decreasing activation of the ES [15]. Thus, stabilization exercises are effective maneuvers to decrease LBP and prevent its recurrence by providing spinal stability and a proper recruitment pattern of the superficial and deep muscles on the surrounding spine [16, 17, 18]. Prone stabilization exercises are often used in the initial rehabilitation of patients with LBP to minimize external load and pain [19, 20], reduce inappropriate movements of the trunk, and maintain a neutral spine while applying an internal or external force [21]. Abdominal bracing (AB) and abdominal hollowing (AH) maneuvers are commonly used to activate the abdominal muscles to increase spinal stability. AH is performed to activate the deep abdominal muscles, namely the transverse abdominus (TrA) and internal oblique, while minimizing superficial global muscle activity [22]. Meanwhile, AB focuses on activating all of the abdominal wall muscles. According to McGill, sufficient stability of the lumbar spine is achieved with modest levels of simultaneous activation of all trunk muscles [23]. Recently, it was suggested that AH is suitable for treating spinal instability with an altered abdominal muscle recruitment pattern, whereas AB might be more suitable for use in healthy participants [24].
Although there have been many comparative studies on abdominal contraction maneuvers in the supine or sitting position [25, 26], few studies have compared the dynamic postures commonly used in clinical practice [27, 28, 29]. Previous studies have measured muscle activity through surface electromyography (sEMG) during prone hip extension with abdominal contraction maneuvers [15, 30, 31, 32]. One study measured isometric hip extension strength during prone standing [26] but it did not account for dynamic strength through a full range of motion (ROM) at different velocities. However, no studies have investigated isokinetic hip extension strength with different abdominal bracing maneuvers. Thus, the purpose of this study was to determine the dynamic concentric strength of the hip extensors in the prone standing position coupled with abdominal stabilization maneuvers and movement velocity.
Method
Participants
G*Power software was used to estimate the sample size (ver. 3.1.9.2; Franz Faul, University of Kiel, Kiel, Germany) according to Cohen’s d. An a priori sample size calculation determined that at least 28 participants were required to achieve a power of 0.80, an alpha level of 0.05, and effect size of 0.25. A total of 31 healthy male subjects with age: 29.1
Descriptive characteristics of the participants (
31)
Descriptive characteristics of the participants (
SD, Standard deviation.
The experimental protocols and purpose of this study were explained in detail to all participants; they subsequently provided written informed consent. This study was approved by the Yonsei University Mirae Campus Institutional Review Board (1041849-201812-BM-114-04).
A Biodex System 4 Pro (Biodex Medical Systems Inc., Shirley, NY, USA) was used to assess isokinetic function and the strength of hip extension in the prone standing position. All exercise tests were performed in isokinetic mode. A pressure biofeedback unit (PBU, Chattanooga Group Inc., Hixson, TN, USA) was used to ensure lumbopelvic motion and abdominal contraction during exercise and facilitate retraining of the participants’ movement patterns in the clinic.
Prone standing position for the intervention of IKD.
Before performing any isokinetic tests, the back of each participant was fixed to the table using a Velcro strap to minimize any unnecessary compensation in the trunk. The participants leaned forward on a table to support their trunk with the hips flexed to 90
Abdominal resting (AR) AR indicates that the abdominal muscles did not spontaneously contract [36]. Abdominal hollowing (AH) AH is performed to activate the deep abdominal muscles, namely the TrA and internal oblique, while minimizing superficial global muscle activity. Abdominal bracing (AB) AB is performed to activate all abdominal wall muscles, including the external, internal, and transverse muscles, without an abdominal drawing-in motion.
When applying the abdominal stabilization maneuver, a blood pressure cuff was placed under the abdomen to function as a PBU, which was checked under the supervision of a professional therapist. This method was applied as a reliable standardized procedure [30, 37, 38]. It was placed under the abdomen with the navel in the center and the distal edge of the pad in line with the right and left anterior superior iliac spine. With the cuff inflated to 70 mmHg, the participants were asked to perform an isometric abdominal contraction using the two separate maneuvers. When performing AH, the pressure was expected to fall by 4–10 mmHg, whereas an increase in pressure was expected for AB [22]. The participants were alerted when the pressure gauge was reduced below 4 mmHg or increased above 10 mmHg [39], and only data with a pressure change of
The Statistical Package for the Social Sciences (Windows ver. 23.0; SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. All dependent variables are presented as the mean
Isokinetic hip extension at an angular velocity of 60
/s (Mean
SD)
Isokinetic hip extension at an angular velocity of 60
SD, Standard deviation; PM, Peak Moment; TW, Total Work; AP, Average Power. Nm, Newton Meter; J, Joule; W, Watts.
Peak moment of hip extension during PSHE according to three abdominal contraction maneuvers. A. Right hip extension, B. Left hip extension at an angular velocity of 60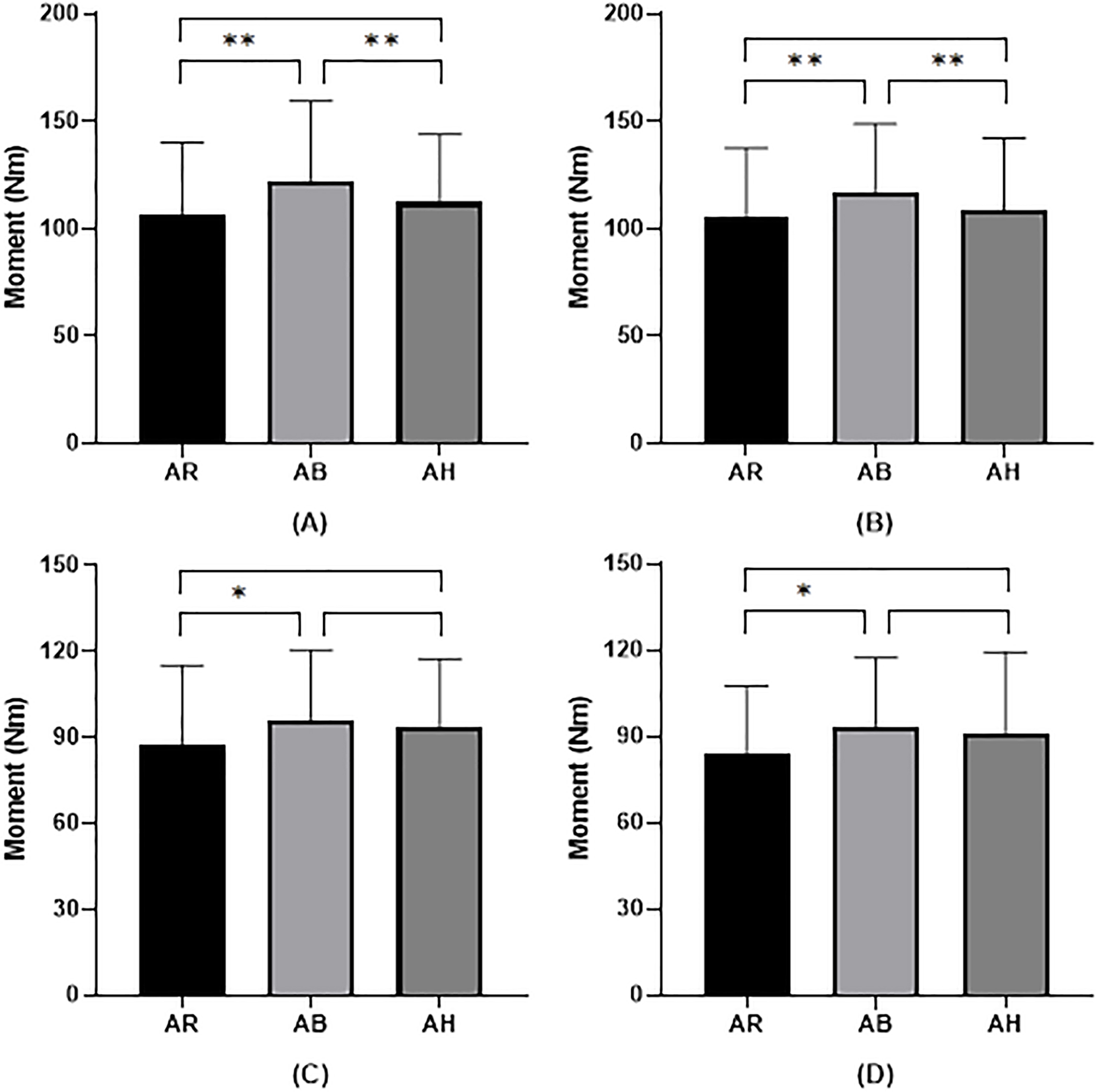
On both sides, hip extension peak moment (PM), total work (TW) in joule and average power (AP) in Watt, were significantly different between the three abdominal contraction maneuvers at 60
Isokinetic hip extension at an angular velocity 180
/s (Mean
SD)
Isokinetic hip extension at an angular velocity 180
SD, Standard deviation; PM, Peak Moment; TW, Total Work; AP, Average Power. Nm, Newton Meter; J, Joule; W, Watts.
Total work of hip extension during PSHE according to three abdominal contraction maneuvers. A. Right hip extension, B. Left hip extension at an angular velocity of 60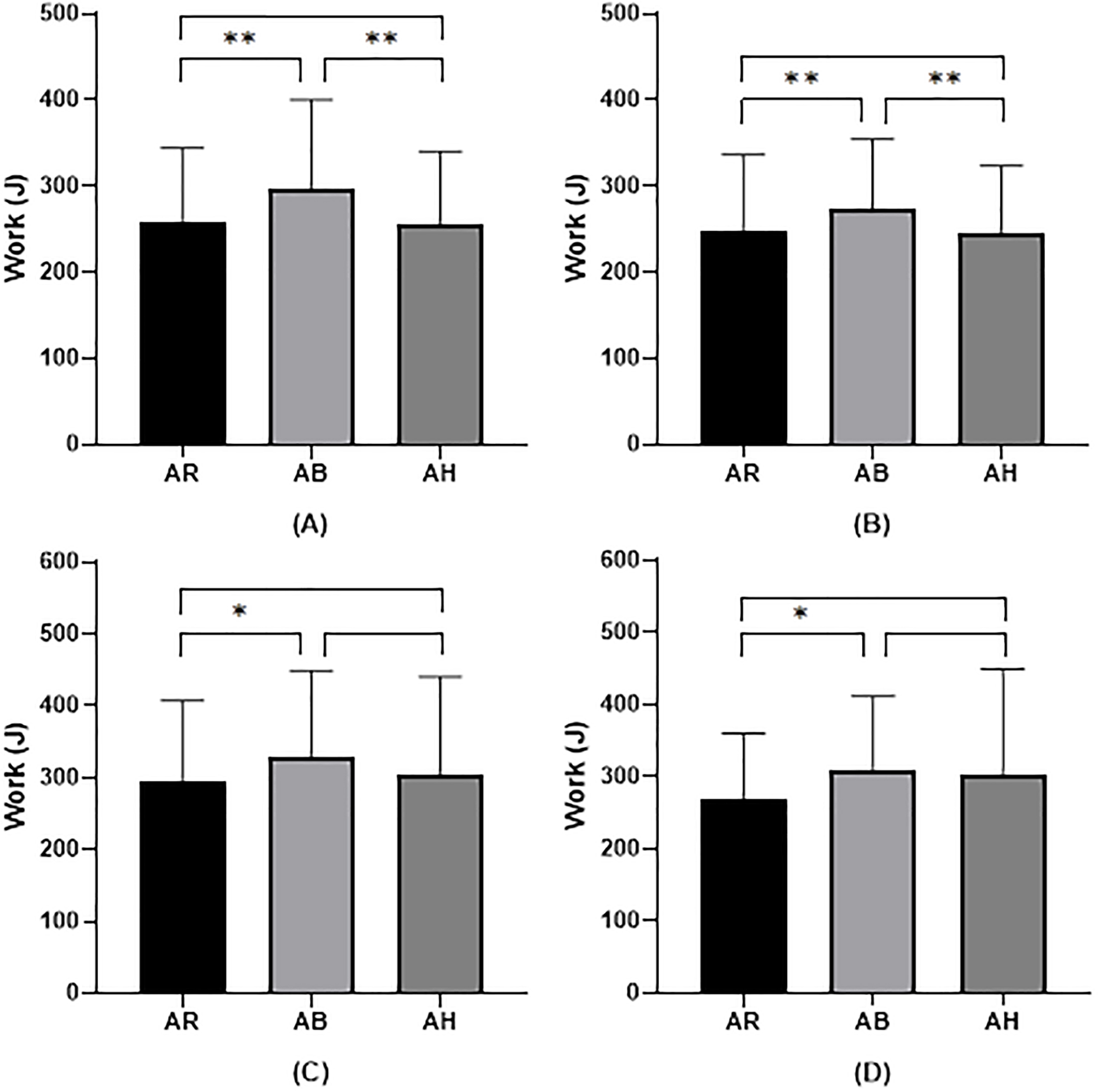
Average power of hip extension during PSHE according to three abdominal contraction maneuvers. A. Right hip extension, B. Left hip extension at an angular velocity of 60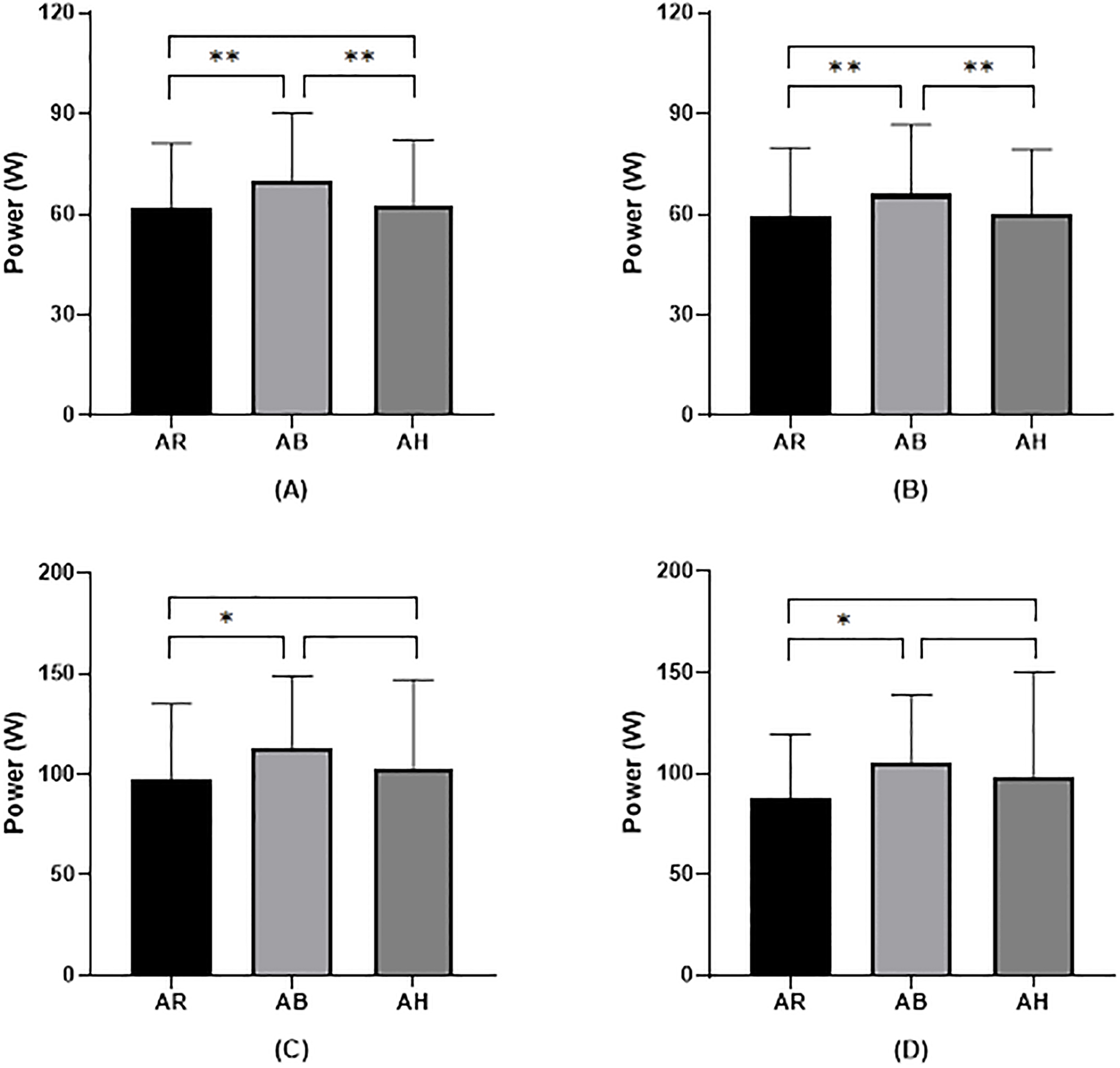
Similarly for the 180
The results of this study show that using AB during PHSE enhanced the moment generated during hip extension compared to hip extension with AH or AR. These results are similar to the findings of other studies on hip extension strength. For example, Tayashiki et al. reported that hip extensor strength in the supine position increased when the subjects performed the AB maneuver [40]. On the other hand, Kim et al. reported that hip extensor strength in the prone position increased by using the AH maneuver [41]. Thus, it is unclear whether the AB or AH maneuver is more effective at enhancing hip extension strength in a non-standing position. In addition, all of these studies only measured muscle activity and did not directly measure isokinetic muscle strength components such as moment, work, and power.
The prone standing position in this study has the advantage of allowing for more stable and increased hip extension strength than could be achieved in the prone position in previous studies [15, 32, 37, 42]. Prone hip extension exercises are often incorrectly performed with excessive compensatory movements in the lumbar spine, inducing lumbar lordosis and unwanted anterior pelvic tilt. This excessive movement of the lumbar spine and pelvis can cause compression and extension stress in the spine and surrounding soft tissues [18, 22]. Thus, Waters confirmed in his study on the correlation between hip angle and hip extension strength that hip extension with 90
Several authors have recommended spinal stabilization exercises during dynamic hip extension movements to control excessive movements of the lumbar spine and pelvis [6, 44]. However, previous studies [15, 31, 37] have only measured the muscle activity of the lower extremities during hip extension with abdominal stabilization maneuvers. In this study, isokinetic concentric contractions were performed to assess also the moment-velocity relationship of the hip extensors at 60 and 180
The PM when using AH was greater than with AR, but there was no significant difference at 60
The PM while using AB was significantly greater than with AR, but there was no significant difference between AB and AH at 180
In this study three isokinetic parameters were recorded: PM, TW and AP. Due to the characteristics of the moment curve, there is a close relationship between the PM and TW. This very strong relationship has been studied and reported before [51]. Moreover, as the power derives directly from the work, the other two are also closely related. These relationships are clearly evident from Figs 2–4, which depict very similar variations in magnitude irrespective of the parameter, relative to the experimental condition. It should also be mentioned that with individual selection of the ROM, the TW is bound to change from subject to subject while the PM, being a single point in the curve is generally stable irrespective of the former [52]. Thus, the use of the PM seems perfectly sufficient for assessing the isokinetic strength of muscles.
This study has several limitations. First, the results of this study are representative of a young, healthy male population, which may not be generalizable to other populations. Second, pressure feedback was used as the sole criterion to differentiate between AB and AH, and the sEMG activity of the abdominal muscles was not monitored. The ability to measure sEMG of the abdominal muscles was limited because the experiment was conducted in the prone standing position, which presses on the abdomen. Third, kinematic data were not collected to confirm the stability of the lumbar spine and pelvis and to describe muscle recruitment patterns.
Conclusion
Based on the results of our study, we recommend that the AB stabilization maneuver be used when performing dynamic motions such as hip extension in the prone standing position.
Footnotes
Conflict of interest
The authors declare no conflict of interest.