
Abstract
BACKGROUND:
Lateral abdominal muscle strengthening exercise can improve the function and motor control of core musculature, but the influence of exercise posture and unstable support surface is controversial.
OBJECTIVE:
To evaluate the influence of bridge exercise type and support surface on abdominal muscle thickness during three bridge exercises with two different support surfaces.
METHODS:
Real-time ultrasonography was used to measure the muscle thickness of the transverse abdominis, internal oblique, and external oblique muscles in 45 healthy volunteers. The supine, prone, and flank bridge exercise were performed on stable and unstable support surfaces.
RESULTS:
The thickness of all muscles was significantly increased during flank compared to supine bridge exercise and prone with stable support (
CONCLUSION:
Bridge exercises performed with unstable support do not influence the contraction thickness of lateral abdominal muscles any more than those performed with stable support. In healthy individuals, thickening of abdominal muscles is influenced more by maintaining a specific posture than by the support surface when the target muscles are engaged as agonists.
Keywords
Introduction
Many studies have reported that core stabilization exercises weres effective in reducing the risk of low back pain (LBP) and dysfunction [1, 2, 3, 4]. The aim of these exercises is to improve the activation patterns and strengthen the lateral abdominal muscles, such as multifidus and transverse abdominis (TrA) [5, 6]. Noteworthy, although most individuals with recurrent of LBP lack evidence of structural problems [7] core stabilization exercises are often recommended [8, 9].
Core stability is defined as the ability of the lumbo-pelvic-hip complex to return to equilibrium following a perturbation without buckling of the vertebral column [10]. It consists of global and local stability and is achieved from co-activation of trunk muscles that produce these stabilities. The global stability system refers to the large and superficial muscles around the abdominal and lumbar region such as rectus abdominis, paraspinalis and external oblique (EO), the prime movers for trunk. Local stability is provided by the lateral and intrinsic muscles of abdominal wall such as the TrA and internal oblique (IO). These muscles support the segmental stability of the lumbar spine during gross body movements and postural adjustment [11, 12]. Abnormal or impaired function of these muscles is related to dysfunctions for lumbar spine and therefore various exercises have focused on functional improvement of local stabilizing muscles [13, 14].
Bridge exercise, one of the lateral abdominal muscle strengthening exercises, is a common strategy in rehabilitation exercise as well as in physical therapy [15, 16]. It contains multi-planar, multi-joint movements and activates specific muscles as agonists or synergists according to the posture. However, it is difficult to explain this role to patients and hence it is important to find out effective method of prompting an automatic contraction of those muscles [17]. Exercise with unstable support surface (US) leads to postural disturbance, inducing higher activation of those muscles to maintain the posture. Intensive training on unstable support surfaces can enhance the stability of core muscles and enlarge the cross-sectional area of muscles by increasing the speed and intensity of lumber stabilizers’ contraction and the activation [18]. Thereby, bridge exercise with US is used to activate the lateral abdominal muscle easily and automatically [19, 20]. Previous studies have reported that abdominal muscle strengthening exercise with US increase activation of lateral abdominal muscle [21, 22]. However, it is still unknown whether the lateral abdominal muscles are more active with US than with a stable support surface (SS).
Rehabilitative ultrasound image (RUSI) allows the visualization of muscle contraction; it has been shown to reliably assess the lateral abdominal muscle in different body positions [23]. The intra-rater reliability of RUSI for the determination of the thickness of the TrA and the lateral abdominal musculature (EO and IO) at rest, and during the abdominal drawing-in maneuver has been reported as good (ICC
Hence the purpose of this study was to assess the significance of this relationship using three types of bridge exercises: the supine, prone and flank bridge and to find out whether the addition of US is beneficial for automatic contraction thickening of the lateral abdominal muscles.
Methods
Subjects
Forty five healthy subjects (22 men, 23 women, age: 20.9
General characteristics
General characteristics
Note: BMI
RUSI image and contraction thickness of lateral abdominal muscles was measured by drawing a vertical reference line that was located 2.5 cm from the edge of the transverse abdominis muscle. Note: TrA 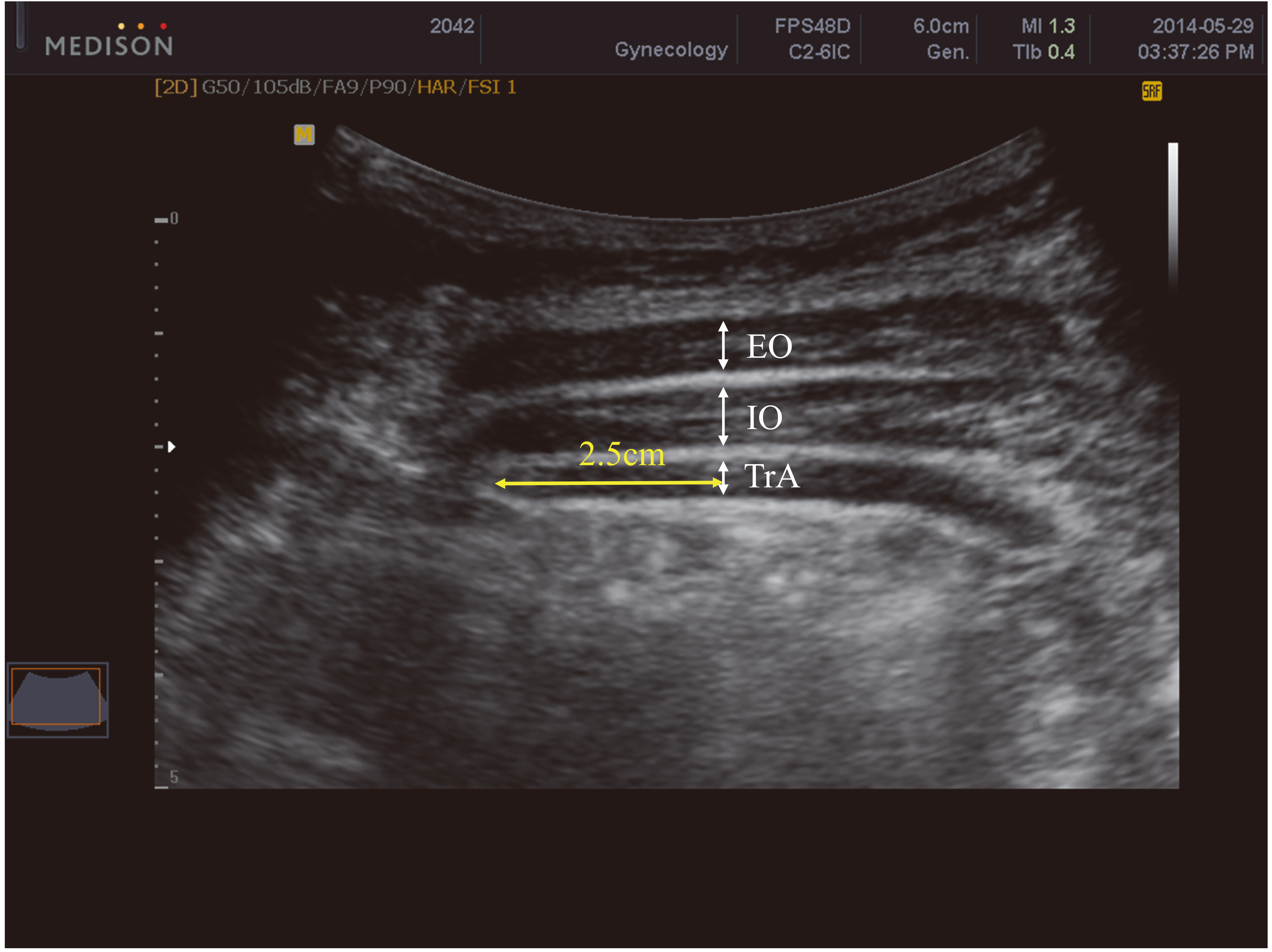
Real-time B-mode (MYSONO US, Samsung Medicine, Seoul, Korea) ultrasonography was used to measure TrA, IO and EO muscle thickness with 7.5 MHz linear transducer. The ultrasonography equipment was prepared for muscular imaging, gel was poured on the transducer, and it was put on the lateral abdominal wall without any pressure. The transducer was placed just superior to the iliac crest on the dominant side in the transverse plane along the mid-axillary line [23]. Images were captured when the muscle fascia and apex of the TrA muscle were clearly visible during end of expiration period of subjects and adjusted so that all three lateral abdominal muscles were observable on monitor. The RUSI measurement was carried out 3 times for each exercise allowing calculation of the average thickness of TrA, IO and EO muscle. The dominant side of the subjects’ TrA, IO and EO was selected for evaluation. The thickness of these muscles was defined by drawing a vertical reference line that was located 2.5 cm from the edge muscle fascia junction of the TrA muscle [29] (Fig. 1).
Descriptive statistics for the differences of 3-lateral abdominal muscles contraction thickness during bridge exercises compared to resting posture
Descriptive statistics for the differences of 3-lateral abdominal muscles contraction thickness during bridge exercises compared to resting posture
Note: TrA
To enable the subjects’ understanding of the entire procedure, each individual received a pictorial representation of resting position and the three types of bridge exercise with SS and US. Images were recorded during those exercises using RUSI. To obtain the contraction thickness of TrA, IO and EO, subjects were positioned supine on the bed with their hip and knee flexed to 30
Bridge exercises used in this study. Supine bridge with stable support surface (A), supine bridge with unstable support surface (B), prone bridge with stable support surface (C), prone bridge with unstable support surface (D), flank bridge with stable support surface (E), flank bridge with unstable support surface (F).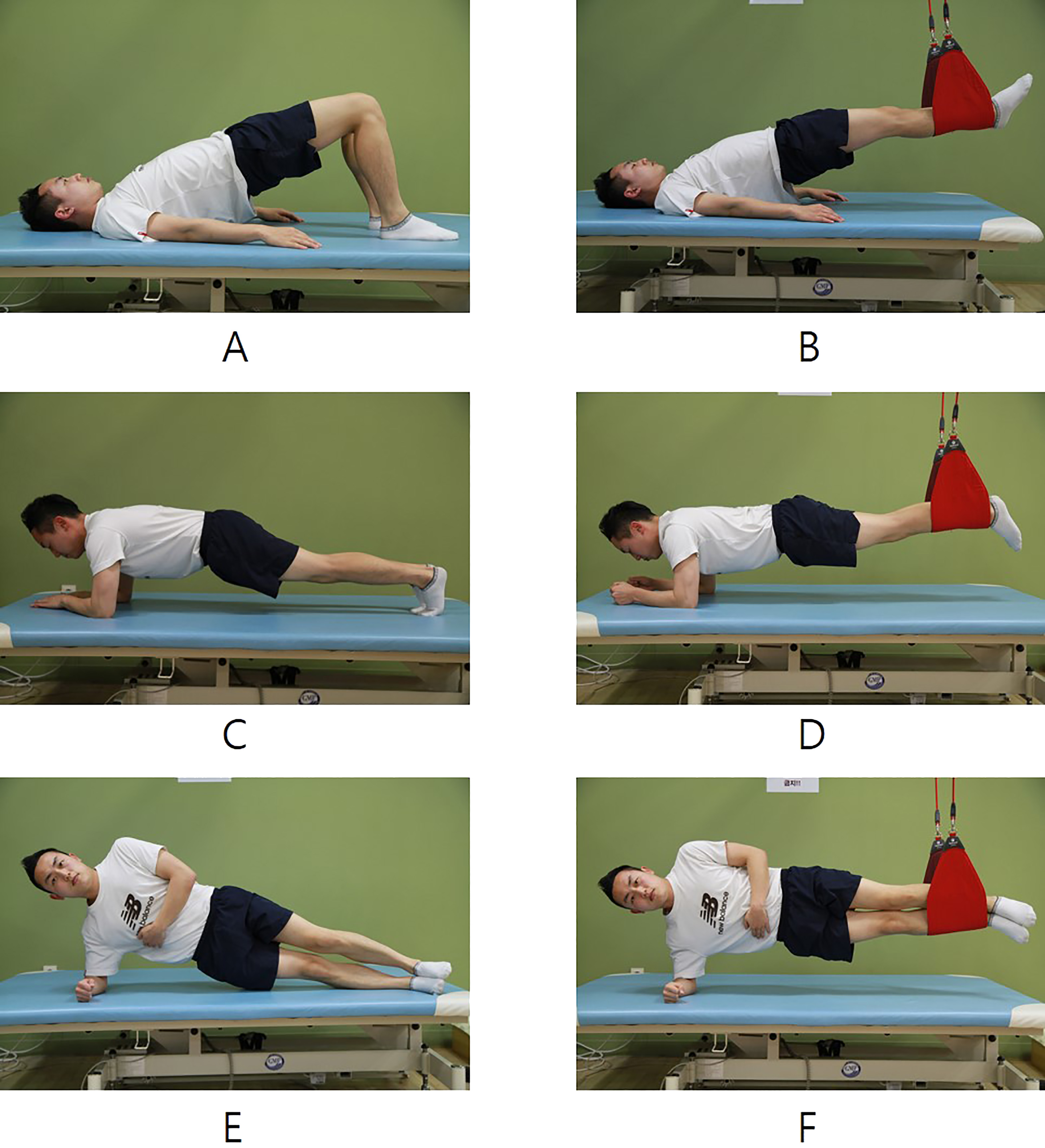
Subjects were required to stay in supine position with the hip and knee joint flexed. Next, the subjects had to lift up their pelvic upward till the thigh and lumbo-pelvic part became straight with the feet contacting the table (SS, Fig. 2A) or use a sling (US, Fig. 2B).
Prone bridge exercise
Subjects were required to stay in prone-plank position on their forearm and then instructed to lift their abdomen upward till the thigh and lumbo-pelvic part became straight with the feet contacting the table (SS, Fig. 2C), or use the sling (US, Fig. 2D).
Flank bridge exercise
Subjects were required to stay in side-plank position on their right forearm and then instructed to put their upper arm vertical to the ground and place the left arm was on their dominant side of hip with the feet contacting table (SS, Fig. 2E), or use the sling (US, Fig. 2F).
Statistical analysis
The PASW statistics 18.0 (SPSS) was used to analyze data. Results were considered significant at a
Results
With SS and US, contraction thickness of TrA, IO and EO muscle during three types of bridge exercise was significantly increased compared to that of the resting position (
The differences of abdominal muscle contraction thickness compared to each of bridge exercise types
The differences of abdominal muscle contraction thickness compared to each of bridge exercise types
Note: SD
The differences of 3-lateral abdominal muscle contraction thickness compared to support surface types
Note: SD
The summary statistics of Repeated Measure two-way ANOVA testing the effects on abdominal muscle contraction thickness by bridge exercise type and different support surface
Note: Df
Differences of abdominal muscle contraction thickness upon performing each of bridge exercise types are given in Table 3. Upon comparing supine vs. prone bridge exercise with SS, EO muscle contraction thickness increased significantly (
Comparison of the same bridge exercises with different support surface (Table 4) indicated significant increases in muscle contraction thickness in the case of TrA and IO muscle during prone bridge exercise with SS vs. US (
This study aimed to investigate the effects of bridge exercises and different support surface on the contraction thickness of the lateral abdominal muscles, respectively. Our study suggests that an unstable support surface can encourage an increase in lateral abdominal muscle contraction thickness compared to its stable counterpart.
Comparison of bridge exercise type
Irrespective of the support surface type, the flank bridge exercise was the most useful for increasing abdominal muscles contraction thickness compared to resting position, followed by prone, and supine (Tables 2 and 3). Imai et al. have reported that the highest activity of EO muscle was recorded during prone and flank bridge exercises [19], while the prone bridge exercise with the Swiss ball was most effective in activating the IO and the TrA [22]. In a study using surface EMG to evaluate trunk muscle activation during core stabilization exercises, the EO and IO manifested the highest activation during flank bridge as opposed to supine and prone bridge exercise [28]. These results are in agreement with our findings i.e. that abdominal muscle activation changes automatically based on the body position during bridge exercises, in order to maintain each posture and lumbo-pelvic stability. Interestingly, while the contraction thickness of the EO was significantly increased in supine vs. prone bridge exercise with SS, neither the IO nor the TrA showed any significant changes. On the other hand, in supine vs. prone and prone vs. flank bridge exercise with US, the contraction thickness of TrA, IO and EO manifested a significant increase. That is, superficial abdominal muscle showed a significant increase in contraction thickness upon changing the bridge exercise type; however, deep abdominal muscle only showed a significant increase upon performing flank bridge exercise. Because the EO muscle is a superficial muscle and a prime mover for trunk [11] its thickness was significantly increased in all bridge exercises, regardless of SS or US. On the other hand, as the TrA and IO are deep muscles which operate as local stabilizers they did not, as expected, undergo a similar change in the supine bridge exercise with SS. With US, the contraction thickness of all monitored muscles did increase significantly in supine vs. prone, supine vs. flank and prone vs. flank exercise since the US probably mandated deep abdominal muscles involvement in order to maintain the lumbo-pelvic stability and postural adjustment. Thus, the contraction thickness of the deep abdominal muscle can be affected both when they are synergistically engaged and/or when they are activated as agonists to maintain posture against gravity direction.
Comparison of stable versus unstable support surface
In a previous study, which used surface EMG it was demonstrated that a lesser SS can enable higher activation of IO compared to EO during supine bridge exercises [31]. This study evaluated abdominal and para-spinal muscle activation in 20 healthy subjects with surface EMG during bridge exercises and reported that muscles activation was significantly increased with unilateral and US bridge exercise compared to SS. Another study involving 9 healthy subjects demonstrated that core stabilization exercise with US enhanced the activation of trunk muscles, with the exception of the supine bridge exercise [19]. Although the results demonstrated that the use of US is beneficial for activation of deep abdominal muscle, the studies might have had a different outcome if those exercises had better technique than traditional exercises [31]. Another study suggested that US is insufficient for generating an increase in selective muscle activity of the scapula-thoracic and glenohumeral muscles [20]; the addition of US in push-up training did not enable greater improvement in muscular strength and endurance than with SS.
Our study assessed 42 subjects and measured the abdominal muscle contraction thickness using RUSI and compared SS vs. US to confirm the influence of US on automatic contraction thickening of abdominal muscle, especially TrA and IO muscle. In Table 4, the TrA and IO demonstrated significant increase in contraction thickness duing prone bridge exercise with US compared to SS. Contraction thickness of deep abdominal muscle was increased during US when those were activated as synergists. During supine and flank bridge exercise, contraction thickness of deep and superficial abdominal muscle was not significantly increased with US compared to SS.
There were significant effects on contraction thickness for TrA, IO and EO, considering the factor of bridge exercise but not that of the support type. Also, the effect size of the TrA, IO and EO thickness in the different bridge type was relatively higher in comparison to that of the support type. This means that the increase of abdominal muscle contraction thickness is probably influenced by the direction of muscle fiber and gravity during each of the bridge exercises. However, neither TrA nor the EO had any effect on contraction thickness considering the factor of support. As in the supine condition, the prime agonist is not the deep abdominal muscle but the gluteal muscles and hamstring. Bridge exercises with US have been known as one of the beneficial methods for automatic activation of deep abdominal muscle.
Limitations
Our study has several limitations. First, only healthy young adults were included and thus the results are probably not generalizable to LBP patients and exercise program for lumbo-pelvic dysfunction. Second, we measured the muscle thickness during static contraction which does not portray the changes taking place during dynamic onesas therefore thickness changes cannot be absolute method of examination for lateral abdominal muscle activation. Third, although our methods encourage participants to maintain each of the bridge exercises accurately, it was difficult to confirm that spine and pelvis were aligned thoroughly straight during bridge exercises; more exact quantitative device or method are needed. Finally, lateral abdominal muscles were investigated only but other factors which affect the stability on lumbo-pelvic region such as multifidus, erector spine, and rectus abdominis have to be included in future studies.
Conclusion
This study suggests that unstable support surface can encourage an increase in deep abdominal muscle contraction thickness compared to its stable counterpart during bridge exercise. We also suggest that muscle thickness may potentially be the most direct determinant for quantifying muscle activity in the cross-sectional plane.
Conflict of interest
We confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.