
Abstract
OBJECTIVE:
The main purpose of this study is to investigate the effects of lumbar stabilization exercises on pain intensity, transversus abdominis (TrA) activation capacity, functional disability, and TrA thickness in patients with low back pain (LBP).
METHODS:
The subjects of this study were 30 LBP patients. The experimental group performed diverse lumbar stabilization exercises (LSE) in different postures, and the control group conducted an ordinary trunk muscle strengthening exercise (TSE). All interventions were conducted 3 times per week for 6 weeks.
RESULTS:
Significant differences between LSE and TSE groups were shown in the pain intensity, TrA activation capacity, and functional disability after the intervention (
CONCLUSION:
This study provides clinical evidence that LSE for LBP patients is more effective than TSE in improving pain intensity, functional disability, and TrA activation capacity.
Introduction
Low back pain (LBP) is an ailment of the musculoskeletal system. It involves pain in the 10th thoracic vertebra to the lumber region that continues for more than three days [1]. Annual prevalence rate was in the range of 5 to 22%, and its lifetime prevalence rate is 59%. The prevalence rate for acute, sub-acute, and chronic patients is 53%, 21%, and 26%, respectively [2]. Although chronic LBP patients recover within six to twelve weeks, 60 to 80% undergo recurrence [3]. LBP often implicated with obesity, reduced spinal mobility, increased lumbar lordosis and tension in the hamstring muscle, abdominal muscles weakness, imbalance in trunk muscle strength, and differences in the lengths of the legs [4]. Among them, instability in the lumbar vertebrae, which triggers problems in postural maintenance and trunk stability, causes functional problems in the body [5].
Conventionally, trunk muscle strengthening exercise (TSE) has been used to improve muscular adjustment and trunk stability [6], however outcomes were variable. In contrast, lumbar stabilization exercise (LSE) has recently used to improve trunk stability and pain because it has clinical effects. Selective exercise of the transversus abdominis (TrA), lumbar multifidus, pelvic floor muscle, and diaphragm will all engage in stabilization [7]. In particular, spinal stabilization exercises that increase the contraction capacity of the TrA and lumbar multifidus muscles, alleviate pain, and improve function [8]. Stabilization exercises based on the abdominal drawing-in maneuver (ADIM) are widely used to contract the TrA [9]. ADIM retrains the deep muscles using isometric contractions [10], minimal contractions of the large muscles, and selective contraction of the TrA [11, 12]. Appropriate ADIM provides the stability of the lumbar spine and pelvis by co-contraction of isolated TrA, pelvic floor muscle, and multifidus [13].
Despite the importance of clinical study on stabilization exercise, there is a dearth of evidence on the LSE in patients with LBP. In addition, although there are studies on the effect of LSE on pain and TrA thickness, there is no comprehensive study of pain, TrA activation capacity, functional disability, and TrA thickness in the stabilization exercise. Therefore, this study intends to examine the effects of LSE on pain intensity, TrA activation capacity, and functional disability as well as the thickness of TrA in patients with LBP. Clinically, this comprehensive study enabled us to better understand the mechanism for core stability and thus provide guidelines for core stabilization exercise in patients with LBP.
Methods
Subjects
The age, height, weight, and duration of the experimental group was 31.67
Demographic features (
30)
Demographic features (
To make a blind study, the data analyst did not know what data belong to which group. All outcome measurements were consistently administered in pre- and post-intervention. The visual analog scale (VAS) was used to measure pain intensity. The VAS is a continuous scale of a 10 cm horizontal line which has been shown to be highly correlated with a numeric rating scale ranging from 0.62–0.91 and intra-rater reliability was 0.94 [15]. A pressure biofeedback unit (PBU, Chattanooga Group, Australia) was used to assess TrA activation capacity. PBU test has already been validated comparing to electromyography (EMG) data that are regarded as the gold standard of TrA activation measurements [16]. Prior to testing, the subjects were familiarized with the process of performing the ADIM for approximately 30 minutes. The device was placed on the TrA above the anterior superior iliac crest with the subject in a prone position. The PBU was inflated at 70 mmHg and the subject was asked to draw in subject’s belly button back towards the spine. The subject was instructed to maintain a pressure of 60 mmHg while the TrA was contracted without moving the spinal area and the hip joint, pressure was assessed three times and average values were used for analysis [17]. The Korean version of the Oswestry disability index (K-ODI) was used to evaluate functional disabilities that the subjects experienced because of lumbar pain during daily activities [18]. Intra-rater reliability was found higher in 88 LBP patients (ICC
Lumbar stabilization exercise.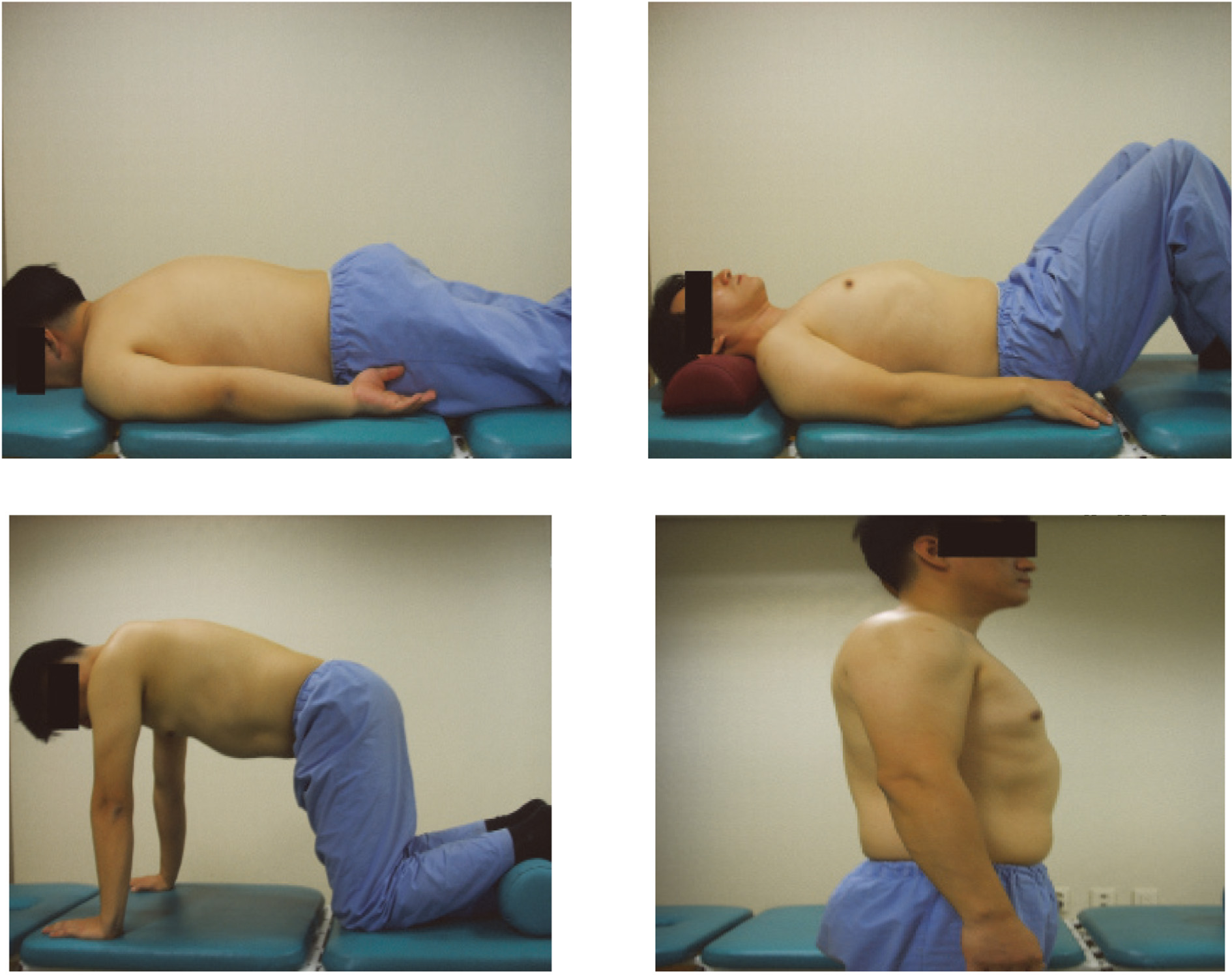
All subjects were instructed to rest in intervals of three minutes between each set [20] and the VAS was used to evaluate the severity of the pain during exercise [21]. The experimental group and the control group conducted LSE and TSE, respectively, for 6 weeks, three times per week. For the LSE, the subjects conducted the ADIM in prone, hook-lying, quadruped, and straight-standing positions by maintaining each motion for 10 seconds. Each motion was conducted 15 times in sets of three repetitions (Fig. 1). For the TSE, the subjects performed trunk extension in a prone position, trunk flexion with rotation in the hook-lying, and hip and knee joint flexion at 90
Trunk strengthening exercise.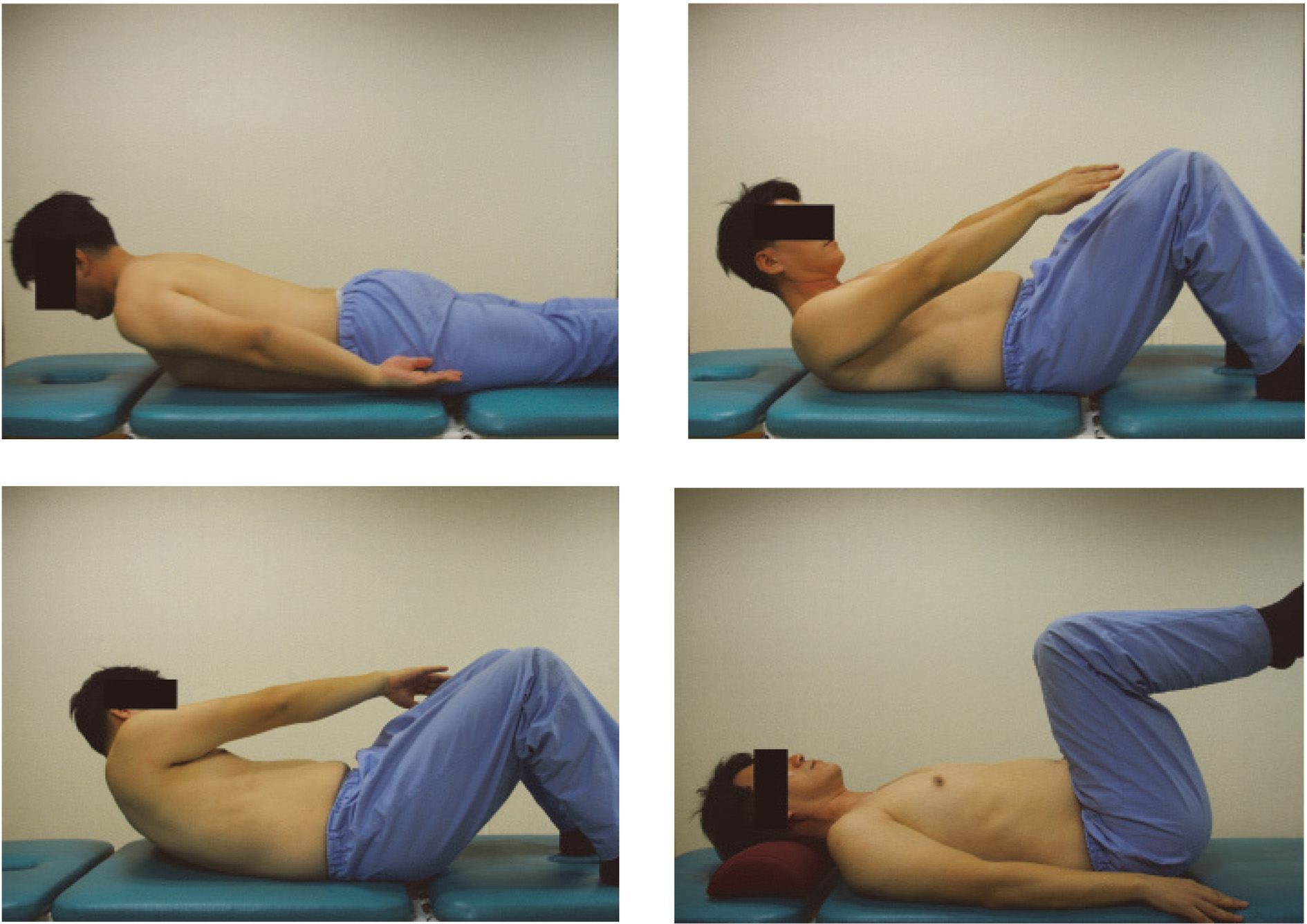
The research design.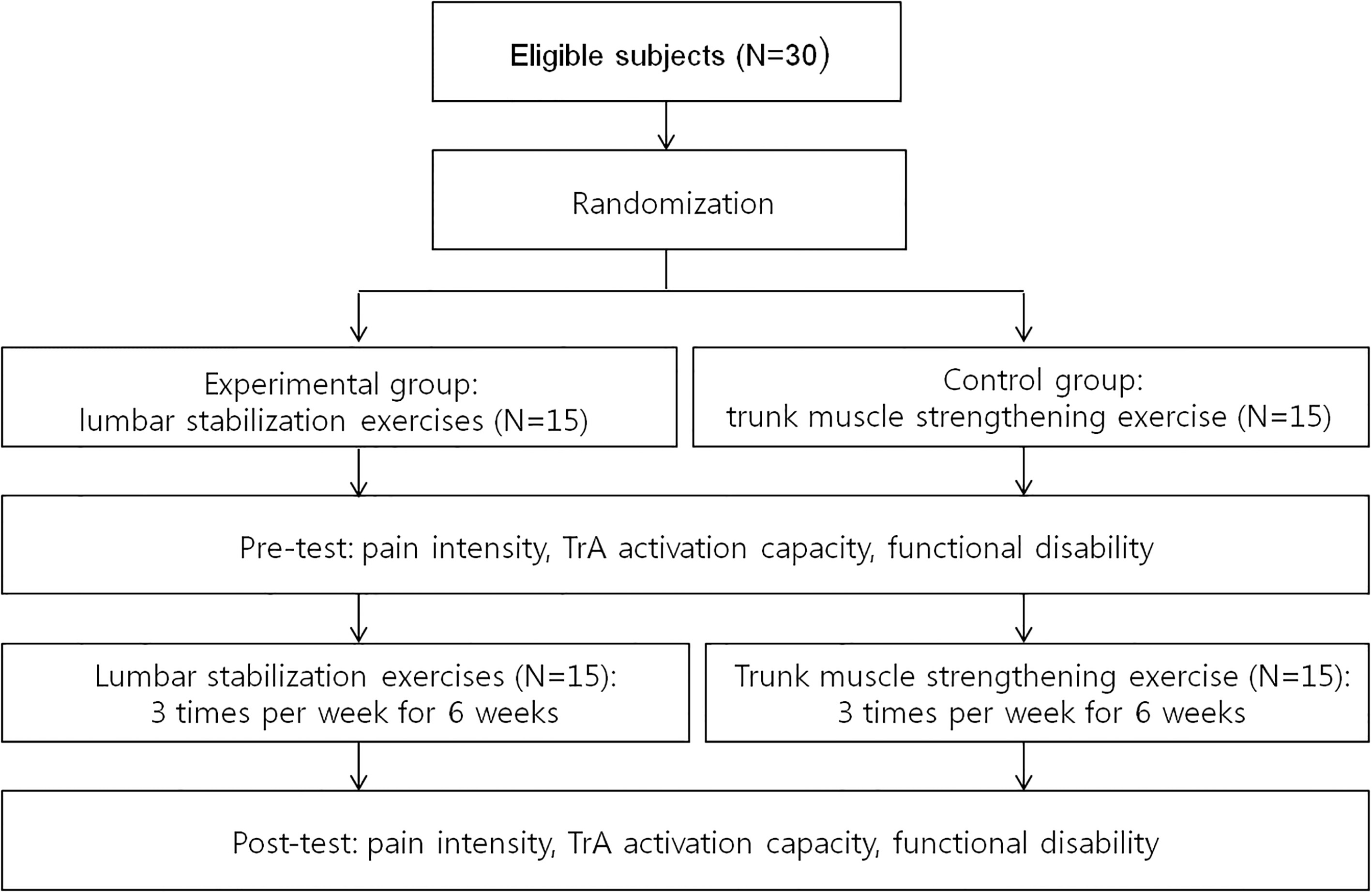
PASW Statistics 20 (Norusis/SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. Kolmogorov-Smirnov test was used to estimate the normality of distribution. A Chi-squared test was used to compare the homogeneity of demographic characteristics. The independent t-test was utilized to analyze the difference of all variables between two groups. The statistical significance level was set at 0.05.
Results
The Kolmogorov-Smirnov test used for normality showed a normal distribution of all dependent variables (
Outcome measurements (
30)
Outcome measurements (
The present study was undertaken to investigate the effects of LSE on pain intensity, TrA muscle activation capacity, functional disability, and the thickness of TrA in patients with LBP. To the best of our knowledge, this is the first clinical trial highlighting the superior effects of LSE on reducing pain and activating TrA muscle in patients with LBP.
Most importantly, this finding suggests that LSE is helpful for reducing pain and activating TrA muscle in patients with LBP. The VAS score was reduced significantly in the LSE group compared to the TSE group. This finding supports the following researches: (1) Slade and Keating [22] observed that muscle strengthening and endurance exercises reduced pain and improved function in chronic LBP patients; (2) Macedo et al. [23] noted that motor control exercise (optimal spine control) were significantly effective in alleviating pain (14-point difference on a 0–100 pain scale).
The TrA activation capacity was significantly increased in the LSE group more than the TSE group. The present finding suggests that LSE was more effective to facilitate TrA muscle than TSE. This result was in line with Franca’s data which showed increased TrA activation capacity (48.32%) after stabilization exercise for six weeks, twice per week. Additionally, Tehen et al. [12] also reported that TrA muscle activation was improved in participants with LBP. Moreover, deep muscles did not recover after pain decreased in chronic LBP patients, and therefore exercise to recover these muscles was necessary [6]. In this study, the difference of the TrA activation capacity was not greater than the Franca’s study. The reason for this is that the mean value of the baseline TrA activation capacity of the subjects was about 3 mmHg, which is higher than that of the previous study subjects approximately 0.67 mmHg. Therefore, patients with TrA activation capacity of 3–4 mmHg are advised to apply interventions longer than 6 weeks.
The K-ODI data demonstrated that LSE was more reduced than TSE, which showed results similar to those of the previous research. Andrusaitis et al. [24] asserted that stabilization exercises were more effective than muscle strengthening exercises in a study where pain and functional disability were compared after stabilization and muscle strengthening exercises. Andrusaitis’s study reported that the ODI decreased from 11.8 to 3.4 and the VAS score decreased from 5.08 to 0.23 after stabilization exercises. However, in the muscle strengthening exercise group, the ODI decreased from 19.8 to 18.2 and the VAS score decreased from 4.83 to 3.59.
A concurrent ultrasound measurement of TrA thickness showed a significant within-group main effect, however statistical significance failed to reach significance level between groups. Franca et al. [25] asserted that stabilization training of the TrA should be included in rehabilitation protocols for chronic LBP patients. In addition, Mannion et al. [26] noted that measuring the thickness of the TrA to evaluate core stability was important. Their results showed that the thickness of the TrA of LBP patients was 21% smaller than that in normal people. Similarly, Hides et al. [27] verified the relation between weight load and the thickness of the TrA, noting that the thickness of the TrA was 4.0 mm at rest and increased to 4.5 mm at 25% weight load and to 4.9 mm at 45% weight load. Additionally, Teyhen et al. [28] observed that the thickness of the TrA increased from 3.8 mm at rest to 6.1 mm during lumbar stabilization in unilateral LBP patients. Moreover, the thickness of the TrA increased from 4.1 mm at rest to 6.8 mm during lumbar stabilization in normal subjects, with no difference between the two groups. Noormohammadpour et al. [29] asserted that specific TrA training was necessary, which was similar to previous studies that showed TrA played an important role in the stabilization of the spine [27, 30]. They observed that the thickness of the TrA increased from 0.42 mm prior to the intervention to 0.48 mm after the intervention.
Taken together with our findings, LSE is an effective strategy for alleviating pain and functional disability, as well as in activating the TrA when compared to TSE. Thus, if clinicians use LSE program with pelvic floor and multifidus muscle strengthening exercise, trunk stability and back pain may improve in patients with LBP.
There are some limitations in this study. First, the number of subjects was too small. Further studies will require larger sample size. Second, this study focused on the TrA muscles and pain in LBP patients. However, patients with LBP are associated with inactivation of multifidus and pelvic floor muscles. Therefore, further studies are needed to determine the multifidus and pelvic floor muscle activation in LBP populations.
Conclusion
Six weeks of lumbar stabilization exercise for LBP patients is more effective than ordinary trunk muscle strengthening exercise in improving pain intensity, functional disability, and TrA activation capacity, although the latter was not associated with any inter-method difference.
Footnotes
Conflict of interest
None to report.