
Abstract
Study Design:
Retrospective study of consecutive patients at a single institution.Objective: Examine the effect of minimally invasive surgery (MIS) versus open transforaminal lumbar interbody fusion (TLIF) surgery on long-term postoperative narcotic consumption.
Objective:
Examine the effect of minimally invasive versus open TLIF on short-term postoperative narcotic consumption.
Methods:
Differences between MIS and open TLIF, including inpatient opioid and nonopioid analgesic use, discharge opioid use, and postdischarge duration of narcotic usage were compared using appropriate statistical methods.
Results:
A total of 172 patients (109 open; 63 MIS) underwent primary TLIF. There was no difference in baseline characteristics. The MIS TLIF cohort had a significantly shorter operative time (223 vs 251 min, P = .006) and length of stay (2.7 vs 3.7 days, P < .001) as well as less estimated blood loss (184 vs 648 mL, P < .001). MIS TLIF had significantly less total inpatient opioid usage (167 vs 255 morphine milligram equivalent [MME], P = .006) and inpatient oxycodone usage (71 vs 105 mg, P = .049). Open TLIF cases required more ongoing opiate usage at 3-month follow-up (36% open vs 21% MIS, P = .041). A subanalysis found that patients who underwent an open TLIF with a history of preoperative opioid use are significantly more likely to remain on opioids at 6-week follow-up (87% vs 65%, P = .027), 3-month follow-up (63% vs 31%, P = .008), and 6-month follow-up (50% vs 21%, P = .018) compared with MIS TLIF.
Conclusion:
Patients undergoing MIS TLIF required less inpatient opioids and had a decreased incidence of opioid dependence at 3-month follow-up. Patients with preoperative opioid use undergoing MIS TLIF are less likely to require long-term opioids.
Introduction
Demand for lumbar spinal fusion is increasing over time and mirrors the trend in aging demographics. More than 3.5 million spinal fusion procedures were performed from 2001 to 2010. 1 From 2000 to 2009, the population-adjusted rate of surgery for lumbar spine degenerative disc disease increased 2.4-fold and over that time period, the composite of posterior lumbar interbody fusion (PLIF) and posterior lumbar fusion (PLF) increased 2.8-fold. 2
Transforaminal and posterior lumbar interbody fusion comprise 79% to 86% of lumbar interbody fusions. Goz et al 3 found transforaminal lumbar interbody fusion (TLIF) to be performed on older patients with greater comorbidities than either anterior lumbar interbody fusion or combined anterior/posterior lumbar interbody fusion. 3 In the past decade, minimally invasive (MIS) TLIF has increased in popularity relative to the open counterpart. Proponents note decreased length of hospital stay, lower blood loss, and improved patient-reported outcomes (PRO). 4 -7 It should be noted that improvement in PROs is not uniform within the literature and several studies do not demonstrate a significant difference in PROs between open and MIS TLIF. 6 -8
Prescription opioids are the most common cause of unintentional overdose and account for more deaths than all illicit drugs combined. 9 The economic burden of opioid overdose and abuse has estimated total financial costs of $55.7 billion in 2007, and $78.5 billion in 2013. 10,11 Multimodal anesthesia, including narcotic, dexamethasone, muscle relaxant, and acetaminophen has been shown to reduce postoperative inpatient opioid consumption as compared with historical patient-controlled analgesia controls in MIS TLIF patients. 12 But there is a paucity of data on the effect of open versus MIS technique on long-term postoperative narcotic usage. Moreover, it has been described that opioid naivete is a protective factor against long-term narcotic use in the general spine surgery population. 13
Our study examines a population of patients who underwent either open or MIS TLIF. The objectives of this study are to (a) assess for difference in inpatient narcotic consumption in open versus MIS TLIF surgery, (b) query if technique resulted in different nonnarcotic analgesic consumption, (c) evaluate rates of narcotic dependence at 6 weeks, 3 months, and 6 months postoperatively, and (d) evaluate the relative effect of preoperative narcotic consumption on postoperative narcotic dependence in the MIS and open TLIF groups.
Methods
Institutional research board approval was obtained for this single center retrospective cohort study at a large academic institution. Patients who underwent a 1-, 2-, or 3-level primary TLIF between 2014 and 2017 were selected consecutively with the primary diagnosis of spondylolisthesis, lumbar spinal stenosis, severe degenerative disc disease, or pars defect that did not respond appropriately to conservative treatment modalities. Patients with a history of lumbar laminectomy or microdiscectomy were also included. Operative technique was at the discretion of the surgeon. The preinduction pain regimen is standardized across the institution, and postoperative infiltration of local anesthetic is standard procedure for both open and MIS TLIF. We thus examined the differences between MIS and open TLIF in terms of perioperative characteristics, inpatient opioid and nonopioid use, discharge opioid use, and postdischarge duration of narcotic usage using independent-samples t tests. Total oral morphine milligram equivalent (MME) for inpatient and discharge opioid use was calculated as the amount administered to the patient multiplied by the appropriate MME conversion factor as per the Centers for Medicare and Medicaid Services. 14
Total daily MME for discharge medications was calculated as the dosage prescribed to the patient taking into account the MME conversion factor and multiplied by the daily frequency of intended use. Total sum MME for discharge medications was calculated as the dosage prescribed to the patient taking into account the MME conversion factor and multiplied by the prescribed pill count. Outpatient narcotic use was tracked via the patient’s medication prescription record and clinic follow-up.
Statistical Analysis
Statistical analysis was conducted with the SPSS statistical software package (version 23.0; IBM). An initial multivariate logistic regression was run to determine significant predictors of opioid use at 6 months follow-up. Differences between the open and MIS TLIF cohorts in terms of continuous variables were assessed by Student’s t tests. Categorical variables were analyzed with a chi-square test. Significance was defined as P < .05 for all analyses.
Results
Baseline and Perioperative Characteristics
A total of 172 patients (109 open; 63 MIS) underwent a primary TLIF. Baseline characteristics such as age, gender, body mass index, ASA (American Society of Anesthesiologists) class, previous lumbar surgery, psychiatric/chronic pain diagnosis, and preoperative injections did not differ between the 2 groups (Table 1). The MIS TLIF cohort had a significantly shorter operative time (223 vs 251 min, P = .006) and length of stay (2.7 vs 3.7 days, P < .001) as well as less estimated blood loss (184 vs 648 mL, P < .001) (Table 1). There was no significant difference in postoperative complication rate (17% MIS vs 28% open, P = .14). Multilevel TLIF is more invasive than single level TLIF, though no subanalysis was performed in the multilevel group, both the open and MIS groups had a similar number of multilevel TLIF entries.
MIS Versus Open Surgery in Terms of Baseline and Perioperative Characteristics of 172 TLIFs.
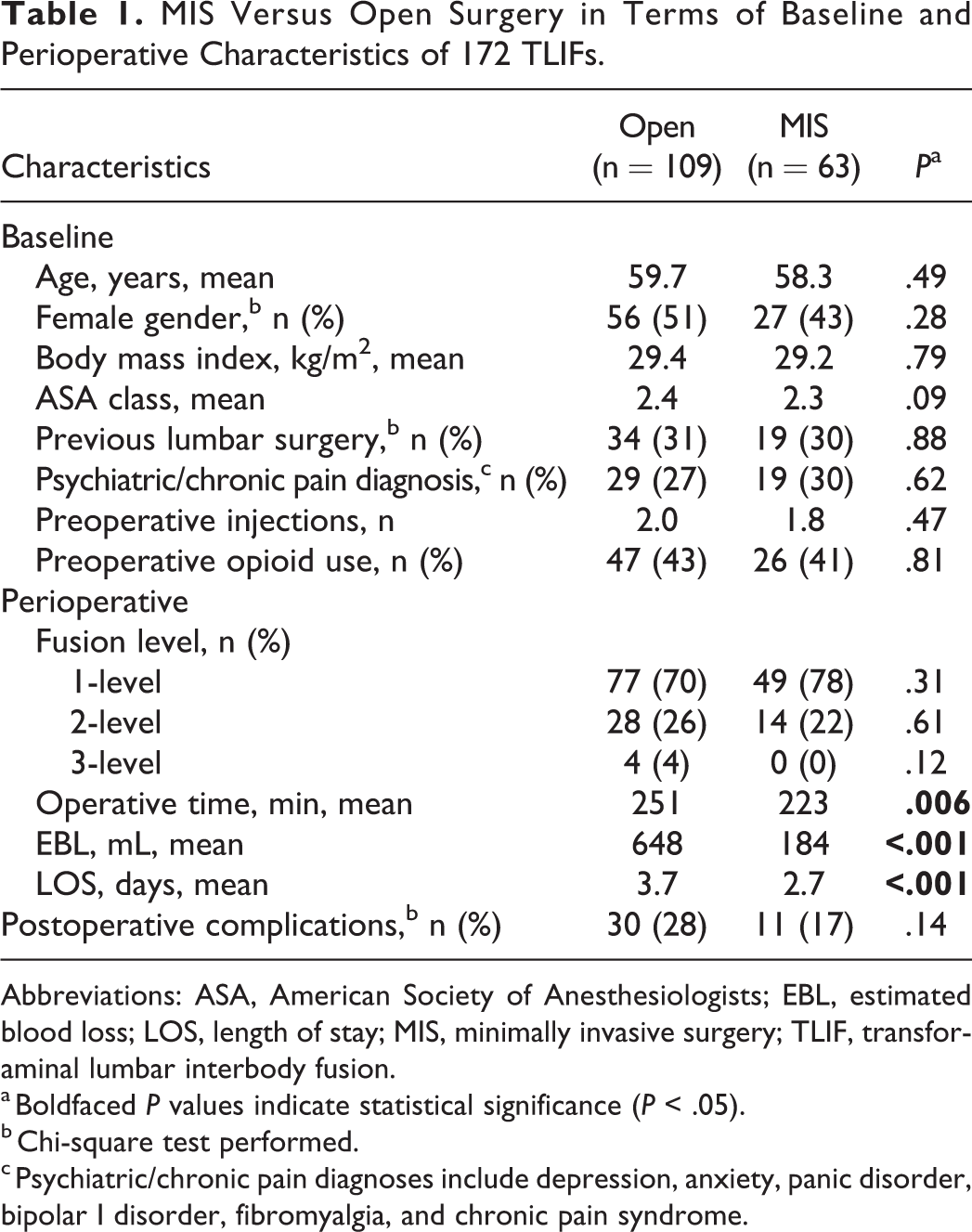
Abbreviations: ASA, American Society of Anesthesiologists; EBL, estimated blood loss; LOS, length of stay; MIS, minimally invasive surgery; TLIF, transforaminal lumbar interbody fusion.
a Boldfaced P values indicate statistical significance (P < .05).
b Chi-square test performed.
c Psychiatric/chronic pain diagnoses include depression, anxiety, panic disorder, bipolar I disorder, fibromyalgia, and chronic pain syndrome.
Inpatient Medication Usage
MIS TLIF patients had significantly less total inpatient opioid usage (167 vs 255 MME, P = .006) and inpatient oxycodone usage (71 vs 105 mg, P = .049). In terms of nonopioid analgesic use, only gabapentin yielded a significant difference (978 MIS vs 2630 open, P = .003) whereas acetaminophen, methocarbamol, cyclobenzaprine, pregabalin, and dexamethasone use were similar between groups (Table 2).
Open Versus MIS Medication Usage in 172 Patients Who Underwent TLIF.
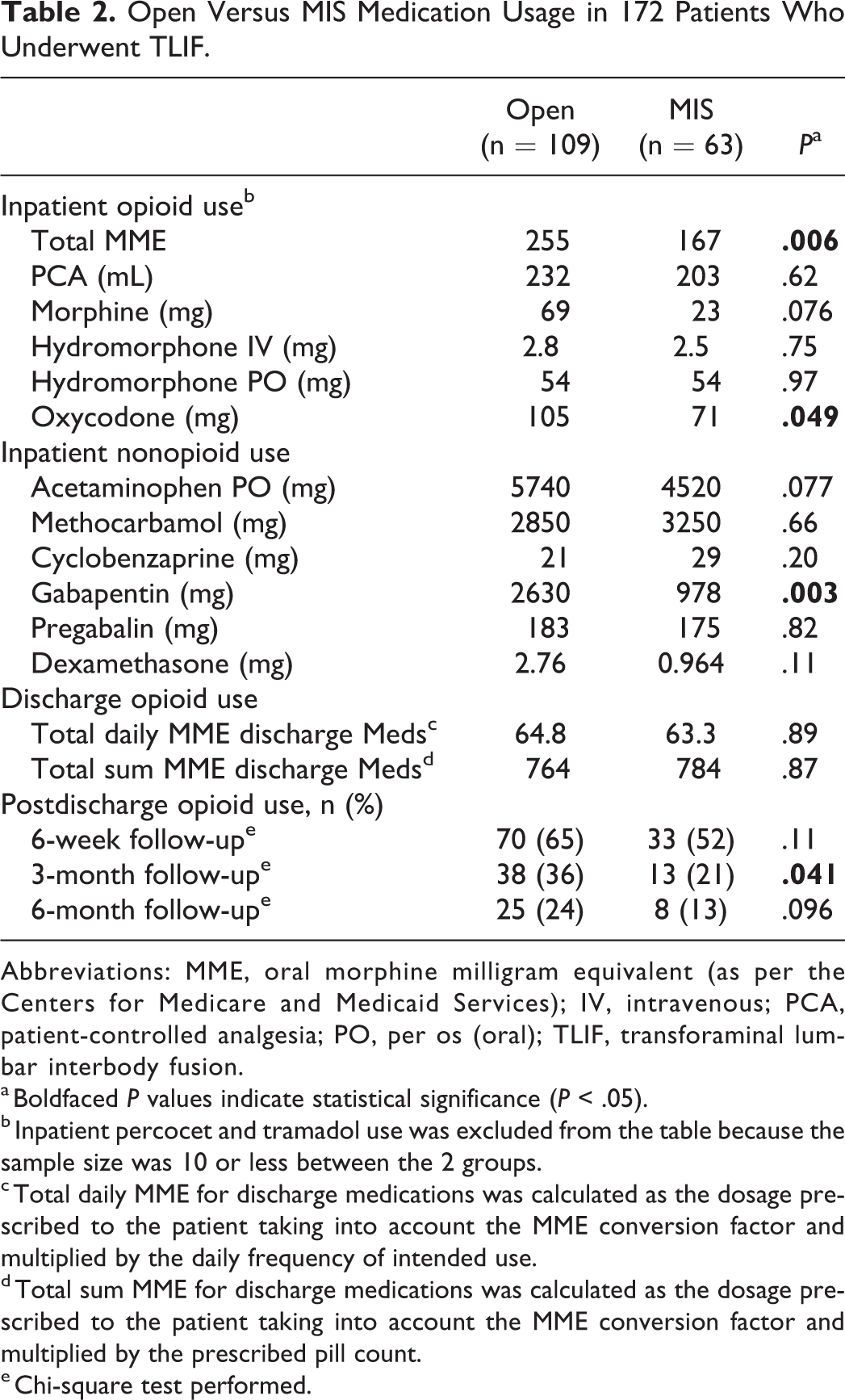
Abbreviations: MME, oral morphine milligram equivalent (as per the Centers for Medicare and Medicaid Services); IV, intravenous; PCA, patient-controlled analgesia; PO, per os (oral); TLIF, transforaminal lumbar interbody fusion.
a Boldfaced P values indicate statistical significance (P < .05).
b Inpatient percocet and tramadol use was excluded from the table because the sample size was 10 or less between the 2 groups.
c Total daily MME for discharge medications was calculated as the dosage prescribed to the patient taking into account the MME conversion factor and multiplied by the daily frequency of intended use.
d Total sum MME for discharge medications was calculated as the dosage prescribed to the patient taking into account the MME conversion factor and multiplied by the prescribed pill count.
e Chi-square test performed.
Postoperative Narcotic Dependence
Open TLIF cases required significantly more ongoing opiate usage at 3-month follow-up (36% open vs 21% MIS, P = .041), and trended toward higher narcotic dependence at 6-week follow-up (65% open vs 52% MIS, P = .11) and 6-month follow-up (24% open vs. 13% MIS, P = .096). In a subanalysis where the MIS and open groups were further subdivided into cohorts based on preoperative opioid usage, it was found that patients with a history of preoperative opioid use who underwent an open TLIF remain on opioids at 6-week follow-up (87% vs 65%, P = .027), 3-month follow-up (63% vs 31%, P = .008), and 6-month follow-up (50% vs 21%, P = .018) compared with patients with the same risk factor of preoperative opioid use who underwent a MIS TLIF (Table 3). On the other hand, patients who were opioid naïve and underwent an Open TLIF were no more likely to continue using opioids at 6-week follow-up (48% vs 43%, P = .68), 3-month follow-up (15% vs 14%, P = .87), or 6-month follow-up (3.4% vs 8.1%, P = .31) when compared with opioid-naïve patients undergoing MIS TLIF (Table 3).
Open Versus MIS Separated Out by Preoperative Opioid Usage in 172 Patients Who Underwent TLIF.
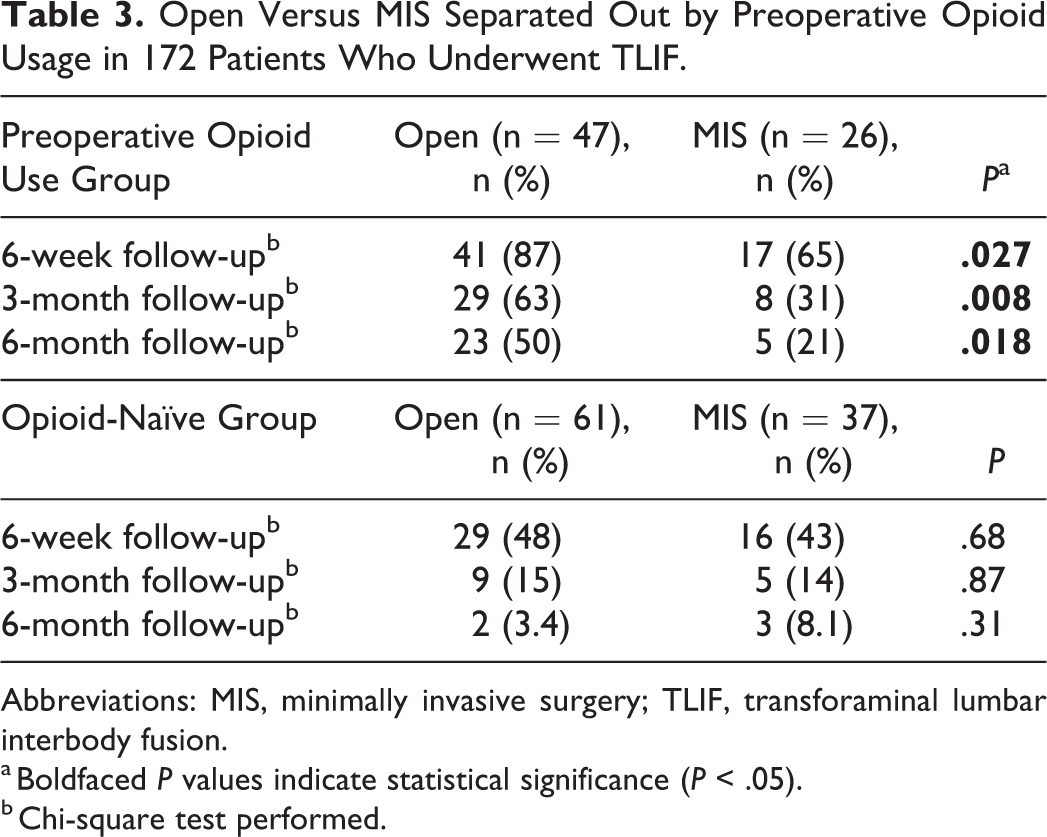
Abbreviations: MIS, minimally invasive surgery; TLIF, transforaminal lumbar interbody fusion.
a Boldfaced P values indicate statistical significance (P < .05).
b Chi-square test performed.
Discussion
Chronic opioid therapy is associated with worse outcomes after lumbar spine fusion including delayed return to work, higher rate of psychiatric comorbidity, and higher cost per patient. 15 To our knowledge, this is one of the only studies comparing the inpatient narcotic use among MIS and open TLIF surgery, conjointly we examined the effect on postoperative outpatient narcotic consumption.
To date, there exist limited data on narcotic consumption patterns of open versus MIS TLIF surgery. Schwender et al 16 studied an MIS TLIF cohort and had a time-to opiate independence of 2 to 4 weeks. Adogwa et al 7 compared open with MIS TLIF and found a significantly lower median interquartile range to opiate independence of 2 (1.0-3.0) versus 4 (1.5-6.5) weeks (P = .008). However, neither examined the inpatient consumption of narcotics, and neither study considered the effect of nonnarcotic in-hospital medications. Peng et al 6 found MIS TLIF consumed less PCA (patient-controlled analgesia) morphine than open technique but did not account for non-PCA narcotic administration. To the contrary, Schizas et al 17 found no difference in in-hospital narcotic or nonnarcotic consumption between the 2 techniques.
Baseline characteristics did not differ between groups and perioperative parameters such as operative time, length of hospital stay, and blood loss, were significantly in favor of MIS technique, which is in keeping with previously reported literature. 4
Our oral morphine equivalent calculation allows comparison of opiate utilization across interpractitioner prescription variability. MIS TLIF had significantly less inpatient hospital narcotic usage overall, as well as significantly less oxycodone usage—which was the principal oral narcotic administered amongst both groups. This is notable as it has been suggested that oxycodone may be a gateway drug to other narcotic drugs of abuse. 18
Outside of gabapentin, differing TLIF technique did not have a significant effect on the prescription and consumption of nonnarcotic analgesic medication. These medications such as gabapentin, pregabalin, muscle relaxants, acetaminophen, and benzodiazepines are often considered part of the multimodal analgesia pathway. There is evidence that multimodal analgesia decreases narcotic consumption in the immediate postoperative period for spine surgery in general, as well as specifically in MIS TLIF. 12,19 Unfortunately, the literature is heterogenous with differing findings. As an example, it has been shown that pre- and postoperative administration of pregabalin (a GABA analogue) can significantly reduce postoperative morphine requirement in patients undergoing elective decompressive spinal surgery, 20 yet in a recent report looking at lumbar spinal fusion, pregabalin neither decreased hospital narcotic consumption nor decreased postoperative pain, or length of hospital stay. 21 Numerous other studies have examined the beneficial effects of other categories of analgesic medications such as intravenous acetaminophen, but its administration did not reduce opioid requirement in the pediatric population. 22,23 To date, there are no universally accepted protocols or pathways to guide perioperative pain management in spine surgery. Some evidence exists for the use of gabapentinoids, acetaminophen, ketamine, neuraxial blockade, and extended-release local anesthetics to reduce postoperative pain and narcotic requirements. 24 -26 However, different pain management protocols are required for minor procedures (eg, microlumbar discectomy) versus major procedures (eg, multilevel spinal fusion) and the optimal combination of drugs is yet to be determined.
Similar rates of preoperative narcotic usage were noted among both groups with 41% of the open group and 43% of the MIS cohort requiring opiate therapy prior to surgery. Despite this, and nearly identical amounts of morphine equivalents at discharge prescription (764 vs 784, P = .87), we found that open TLIF had a higher rate of postoperative outpatient opiate use, which was significant at 3 months, and tended toward significance at 6 weeks and 6 months. This finding is conceptually similar to the observation by Adogwa et al 7 of faster time to opiate independence in MIS TLIF.
Our subgroup analysis accounted for the presence or absence of pre-operative opiate consumption. Patients who used narcotics preoperatively and underwent open TLIF, had a significant incidence of being narcotic dependent at every time point postoperatively when compared with those who used narcotics preoperatively and underwent MIS TLIF. However, this was not true for patients who were opioid naïve. That is, patients who were opioid naïve prior to open TLIF did not have a significantly higher incidence of short- or long-term postoperative narcotic use relative to their MIS TLIF counterparts. Interestingly, it has been shown that patients expect open surgery to be more painful, have longer recovery, and a higher complication risk, as when compared to open surgery. 27 Though pain scores are also subjective, this must be taken into consideration when interpreting our results. Moreover, the subgroup division inherently decreases the number of patients in each group, thus caution is required when weighting the results.
Limitations of this study include study design and data collection. Using narcotic prescriptions as a surrogate marker for usage is more accurate than self-reporting but less accurate than prospective pill counting. Moreover, though we found nearly identical rates of preoperative narcotic usage between the open and MIS groups, we did not quantify the amount of narcotic usage between groups. This is a retrospective design with the inherent associated flaws, a multisurgeon cohort with the incumbent differences in skill and technique, as well as potential interprescriber differences in postoperative pain regimens—though this is mitigated to some extent because all patients are managed by the same group of allied health care practitioners.
Conclusion
Prescription narcotic abuse is a burgeoning public health problem with disastrous socioeconomic fallout. This study demonstrates that patients undergoing MIS TLIF required less inpatient opioids and had a decreased incidence of opioid dependence at 3-month follow-up than open TLIF, and trended toward significantly lower opioid dependence at 6 weeks and 6 months. The data corroborates previous studies that report shorter operative time, shorter length of stay, and less estimated blood loss for MIS versus open TLIF. There was not a significant difference in nonnarcotic analgesic use between open and MIS TLIF. Patients with a history of preoperative opioid use who undergo a MIS TLIF are less likely to require long-term opioids compared with patients with a history of narcotic use who undergo open TLIF, which is an important consideration in the current context of increasing narcotic abuse.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Protopsaltis reports grants from DePuy Synthes, during the conduct of the study; other from Medicrea, other from NuVasive, other from Globus, other from Innovasis, other from Zimmer, and other from Cervical Spine Research Society, outside the submitted work. Dr Errico reports personal fees from K2M, other from Fastenetix, grants and personal fees from Pfizer, grants from Medtronic, other from Harms Study Group, grants from OMEGA, grants from ISSGF, and grants from Paradigm Spine, outside the submitted work. Dr Passias reports personal fees from Zimmer Biomet, personal fees from Medicrea, personal fees from Spinewave, and grants from CSRS, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.