
Abstract
The choice of antibiotics and length of administration in the treatment of deep sternal wound infections (DSWI) is unclear. The reason for this is the lack of studies and local differences in resistance. An increase in resistance can be observed in gram-positive cocci, which are the most frequently detected in deep sternal infections. The duration of administration is often 2- 6 weeks or longer, although the benefit of prolonged antibiotic administration has not been confirmed by studies. We evaluated the antibiotic treatment during surgical treatment, consisting of surgical wound debridement and plastic chest reconstruction.
METHODS:
Retrospective analysis of patients (n = 260) who underwent reconstructive surgery in the Department of Plastic Surgery at Leipzig University Hospital from 01.05.2012 - 31.12.2020. The duration of intake, results of microbiological swabs and resistance were investigated.
RESULTS:
At the time of discharge, closed wound conditions were noted in 177 of 260 cases (68.1%). The largest proportion of patients (n = 238) was treated with a latissimus dorsi flap (91.5%).
Antibiotic treatment was conducted in 206 of 260 cases (79.2%). The mean duration of antibiotic administration was 21.4 days (±17.6). Prolonged treatment over 14 days did not alter outcome (p = 0.226), in contrast, the number of multidrug resistances (p < 0.001). There was no prove of resistance against linezolid which is effective against the most common found infectious agents Staphylococcus epidermidis (n = 93; 24.0 %) & Staphylococcus aureus (n = 47; 12.1 %).
CONCLUSION:
There is no evidence of benefit from antibiotic therapy over 14 days, whereas multidrug resistance increases with prolonged antibiotic use. In the absence of infectious agents or clinical signs of inflammation, surgical treatment without additional antibiotic treatment is effective.
Linezolid is a suitable antibiotic in the treatment of gram-positive infections which are the most frequent in DSWI.
Background
Deep sternal wound infection (DSWI) after cardiac surgery remains a severe and often lethal complication after cardiac surgery. While superficial infections can be treated sufficiently with antibiotics and minor surgery, DSWI is less common and associated with osteomyelitis and 100% lethal if left untreated [1–3]. Due to the increasing complexity of coronary operations and more elderly patients, DSWI continues to show a mortality of up to 30% [4–9]. In addition, there is a prolonged length of hospital stay and increased treatment costs [10]. Recent studies show an incidence of 1.5% to 1.6% [3, 6]. Thus, DSWI is a rare complication, but the severity results in a large cost and resource expenditure with an average of 2.5-3-fold cost increase [6, 11]. DSWI occur most frequently 8–10 days after surgery but may continue to occur up to one year postoperative [12]. Patient associated risk factors are diabetes mellitus, as well as obesity, COPD and smoking, intraoperative it is mainly the bilateral internal mammary artery grafting [13–15].
Efficient treatment consists of radical debridement followed by plastic reconstruction of the chest wall in combination with antibiotic therapy [16]. There are differing opinions as to whether a one- or two-stage approach is preferable [4]. However, studies have shown that immediate plastic flap coverage reduces mortality and morbidity, as well as the risk of chronic infection [17–19]. In addition, a well-perfused flap increases antibiotic concentration in the mediastinal region by improving vascular transport of the antibiotic to its target site [20, 21]. The choice of muscle flap is made depending on the size and location of the defect, as well as comorbidities, previous diseases, and general condition of the patient [22, 23]. The most commonly used flaps are vascular pedicled, such as the latissimus dorsi flap, pectoralis major flap, and less frequently rectus abdominis flap and omentum flap. If pedicled flaps are insufficient for wound closure, microvascular free tissue transfer is needed [24, 25].
If DSWI is suspected, calculated antibiotic therapy should be started immediately after collection of perioperative specimens. Therapy should include the most commonly causative bacteria, coagulase negative staphylococci (CoNS) and Staphylococcus aureus [26, 27]. To include methicillin-resistant bacteria, empiric therapy may be extended with vancomycin [28]. After receiving microbiological results and determination of the resistance situation, the antibiotic therapy must be adjusted accordingly [26, 29].
In general, there is only little information on adequate antibiotic therapy for DSWI, which is due to the locally varying resistances and to the insufficient number of studies. This concerns the empirical antibiotic therapy as well as the targeted therapy after microbiological detection. Initially, usually broad-spectrum antibiotics like ß-lactam antibiotics, quinolones, or aminoglycosides are administered [28, 30–32]. For perioperative prophylaxis during cardiac surgery cefuroxime is the recommended antibiotic treatment [33]. An increase in resistance can be observed in gram-positive cocci, which are the most frequently detected in deep sternal infections. Therefore, antibiotics with good efficacy against vancomycin-resistant gram-positive cocci, such as linezolid, daptomycin, and rifampicin are of particular interest [34, 35].
Weis et al. demonstrated the effectiveness of daptomycin in DSWI treatment in a small study in 2012, as did Popov et al. in 2011 [36, 37]. Khanlari et al. pointed out the improved outcome of patients with deep sternal infection when they received antibiotic therapy with rifampicin [38].
Data on the optimal duration of antibiotic treatment is also scarce. The intake period is often 2–8 weeks, or longer [32, 38–41]. The benefit of prolonged antibiotic administration has not been confirmed by studies. A recommended duration of therapy of 6 weeks is frequently described, of which the first 2 weeks should be intravenously and then orally [28, 41]. This is based on osteomyelitis treatment recommendations, but studies demonstrating the benefit of at least 6 weeks of therapy are lacking as well as comparative studies and studies with more than 100 evaluated cases. In the context of increasing multi-drug resistant bacteria, the duration of antibiotic treatment, as well as the empiric therapy & peri-operative prophylaxis must be questioned critically.
Material and methods
This study is a retrospective analysis of patients diagnosed with DSWI after cardiac surgery and median sternotomy at the Heart Center Leipzig (HZL), followed by plastic reconstruction at the University Hospital Leipzig, between May 2012 and December 2020. In case patients were suffering from DSWI, the Robiscsek cerclages were removed, followed by surgical debridement and temporary wound closure by VAC Therapy. Empiric antibiotic therapy consisting of cefazolin and rifampicin or, in case of possible contraindications to rifampicin, vancomycin was administered. Afterwards patients were referred to our hospital (University Hospital Leipzig, Germany) for plastic reconstruction of the mediastinal region.
Patients underwent revision after a standardized operating protocol for DSWI. This included the stoppage of antibiotic treatment 24 hours prior to the first operation. To achieve a radical debridement, bordering soft tissue was circumferentially incised to a width of about 1.0 cm down to the bone, osteosynthesis material was removed and all necrotic, infected tissue was resected, and wound lavage was performed. Microbiological samples were obtained prior, during and after debridement. Coverage of the chest wall was either performed during the same operative procedure, or in the case of any contraindications, in a second operation. Therefore, we used either a pedicled latissimus dorsi flap, a pectoralis major muscle flap, or an omentum-plasty with mesh graft.
A total of 260 patients were identified. Data collected from chart review included demographic characteristics, length of hospital stay, type and date of cardiac and plastic surgery, length of hospital stay, antibiotic treatment, microbiological swabs and resistances & postoperative complications (operative revision, septic shock, death). All patients met the criteria for DSWI of the U.S. Centers for Disease Control and Prevention (CDC) and were classified according to the criteria proposed by El Oakley and Wright [42, 43]. Patients with only superficial sternal wound infections were excluded. This study was approved by the local Ethics Committee (No. 406-16). All data were evaluated descriptively by a computer-based analysis using SPSS.
Results
From May 2012 until December 2020, 260 patients suffering from DSWI were treated by the Department of Orthopedic Surgery, Traumatology and Plastic Surgery; 156 male (60%) and 104 female (40%). The mean age at the time of revision was 67.6±9.4 The length of the hospital stay was 28.6±18.8 days. On average, the interval between cardiac surgery and the first revision due to deep sternal infection was 67.5 days (±171.0) but differed widely from 3 up to 854 days. Plastic flap coverage was performed on average 25.6 days (±42.5), after the first revision. Epidemiologic and patients’ characteristics are shown in Table 1.
Characteristics of 260 patients
Characteristics of 260 patients
The largest proportion of patients (n = 238) was treated with a latissimus dorsi flap (91.5%). This was followed by coverage with omentum majus flaps (n = 7; 2.7%) and pectoralis major flaps (n = 3 1.2%). In three cases, coverage by latissimus dorsi flap was performed first, followed by re-covering with an omentum majus flap (1.2%). One patient was covered by latissimus dorsi and in the course with a pectoralis major flap (0.4%). Surgical debridement & VAC therapy without pedicled flap coverage was performed in eight patients (3.1%).
Sternal wound healing disruption after plastic flap coverage requiring surgical revision occurred in 142 patients (54.6%). One revision surgery was sufficient in 62 patients (23.8%), at least two reoperations were necessary in 80 patients (30.8%). Wound healing disturbance at the flap harvest site occurred in 42 of 260 cases (16.2%); these were not counted as revisions.
Successful treatment was defined as the hospital discharge with closed wound conditions.
At the time of discharge, closed wound conditions were noted in 177 of 260 cases (68.1%). The remaining cases included deceased patients, findings of persistent wound healing disorder, or a palliative procedure. A total of 58 of the recorded cases died, representing a hospital mortality rate of 22.3%. Of these, 11 patients died within the first 30 days after the initial revision, corresponding to a 30-day mortality of 4.2%. In 27 of 260 cases, the cause of death was documented to be septic shock associated with deep sternal infection (10.4%).
Antibiotic treatment of deep sternal infection was documented in 206 of 260 cases (79.2%). Antibiotics prescribed for a secondary diagnosis and not for therapy of DSWI were excluded. Antibiotic treatment was given until clinical findings improved and/or inflammatory parameters decreased. In the absence of microbiological pathogen detection and clinical signs of persistent infection in 54 cases (20.8%) no antibiotics were administered. Intraoperative administration of single-shot antibiotics, mostly cefuroxime, was not evaluated. A total of 484 prescriptions of antibiotics were counted. On average, 1.9±1.6 antibiotics were prescribed per patient. The mean duration of treatment was 21.4 days (±17.6). A comparison of administered antibiotics with n > 10 is shown in Table 3.
Microbiological findings
The intra-operatively collected specimens showed bacterial growth in 199 cases (76.5%). In 96 of those, only one bacterial species was found (48.2%) (Table 2) The most often detected pathogen was Staphylococcus epidermidis (n = 93; 24.0%), followed by Staphylococcus aureus 47 (12.1%). These were also the most frequently only detectable pathogen (Staphylococcus epidermidis n = 44 (16.9%); Staphylococcus aureus n = 19 (7.3%)). A total of 40 different pathogens could be detected. Pathogens with n > 10 are shown in Table 2.
Infecting species with n > 10
Infecting species with n > 10
Comparison of antibiotics with n > 10
The resistograms of the specimen were evaluated. The percentage of tested isolates with resistance to the respective antibiotic is shown in Table 4.
Proportional specimen resistances (n = 192)
Multidrug-resistant bacteria included methicillin-resistant Staphylococcus aureus strains (MRSA), vancomycin-resistant enterococci (VRE), multi-resistant gram-negative bacteria (MRGN), and gram-negative pathogens with an extended spectrum to ß-lactam (ESBL). Multiple drug resistance was detected in 42 of 260 cases (16.2%). The most frequently detected multidrug- resistance was ESBL with 17 cases (4.4%), followed by VRE with (n = 10 (2.6%)), MRSA (n = 9 (2.3%)), 3MRGN (n = 5 (1.3%)), and 4MRGN (n = 2 (0.5%)).
Antibiotic therapy combined with a radical debridement and plastic reconstructive surgery of the mediastinal region is the key to successful treatment of DSWI [10, 44]. However, data on the optimal antibiotic treatment of DSWI remains scarce. Our study is to our knowledge the largest single-center study, which analyzed the application of antibiotics for DSWI after reconstructive surgery.
The spectrum of pathogens was dominated by the gram-positive bacteria Staphylococcus epidermidis (n = 93) and Staphylococcus aureus (n = 74), which together were detectable in 53.9% of cases. The most frequently detected gram-negative pathogen was E. coli (n = 29) (Table 2). These data are comparable to those reported in other studies [30, 45–47]. Especially, the already reported increase in CoNS could be confirmed [30, 48].
In opposite, the increase in vancomycin-resistant gram-positive cocci as shown in other studies could not be confirmed. Only Enterococcus faecium showed resistance in 56% of the isolates tested; no resistance to vancomycin was detected in the other gram-positive cocci such as Staphylococcus epidermidis or Staphylococcus aureus [34, 35].
The most frequently detected pathogen Staphylococcus epidermidis, showed a high percentage of resistance in general, except for linezolid, vancomycin and daptomycin. This confirmed its pathogenicity in DSWI, even though Staphylococcus epidermidis belongs to the physiological skin flora [31, 49]. This is being supported by our study, identifying in 96 (60,4 %) of the cases as mono-infection and Staphylococcus epidermidis as the only relevant pathogen in 44 (16,9%) of those cases.
Overall Staphylococcus epidermidis & Staphylococcus aureus were detectable in 131 patients (50,4 %) therefore, antibiotics with good efficacy against gram-positive cocci, such as vancomycin, linezolid, daptomycin, and rifampicin are of particular interest [34, 35]. Linezolid has been shown to be effective in the treatment of osteomyelitis and has the advantage of 100% oral bioavailability, lack of nephrotoxicity, and overall, less resistances than vancomycin [50, 51]. The risk of severe side effects, such as thrombocytopenia, is manageable, if regular blood counts are performed [52–54]. Because of its good penetration of the bone, its especially suitable in treatment of DSWI [55–57]. As there was no prove of linezolid resistance in our study, the reported increase in linezolid resistance could not be confirmed [58, 59]. Weis et al. demonstrated the effectiveness of daptomycin in DSWI treatment in a small study in 2012, as did Popov et al. in 2011 [36, 37]. Daptomycin has the disadvantage that it can only be given intravenously, but it is less likely to trigger serious side effects. Both linezolid and daptomycin are potentially more cost-effective in treatment of severe infections, compared to vancomycin [60, 61]. Furthermore linezolid & daptomycin both possess anti-inflammatory properties and have beneficial effects on microcirculation by increasing functional capillary density [62]. Regarding treatment success and complication rate, daptomycin, linezolid, rifampicin & vancomycin showed no significant difference. However, linezolid was the only antibiotic without detectable resistance against gram-positive cocci in our study (Table 4).
Since the group of gram-negative pathogens occurred less frequently overall the choice of suitable antibiotics is much more difficult here. Also, there were only few cases in which gram-negative pathogens occurred as mono-infection (n = 20, (7.7%)). Piperacillin/Tazobactam showed a low number of resistances against the most common gram-negative pathogen, E. coli and Pseudomonas aeruginosa. The overall resistance was high, with 49% of the specimens tested, comparable to other broad-spectrum antibiotics such as imipenem (43%).
Peri-operative antibiotic prophylaxis with cephalosporins is still the state of the art during cardiac operations [33, 63]. There have been recommendations to add vancomycin as perioperative prophylaxis [64]. This was affirmed by our study, as more than 50% of the pathogen were cephalosporin resistant. Moreover, enterococci are not within the spectrum of cephalosporin activity in general. In view of these data, prophylaxis with cephalosporins must be critically questioned and additional prophylaxis in high-risk patients with antibiotics effective against gram-positive cocci should be considered.
The mean duration of antibiotic therapy in UKL was 21.4 days (±17.6), which is comparable to the recommended period in other studies [32, 38–41]. However, in some cases, antibiotic therapy was already started in HZL, which we did not include. In cases where no pathogen could be detected and there were no signs of clinical or local infection, antibiotic therapy was not administered. This group had a higher successful treatment rate (p < 0.05) and less surgical revisions (p < 0.001). The duration of antibiotic treatment had no significant effect on treatment success (p = 0.056). In contrast, there was an increase in multidrug resistance when the duration of intake exceeded 14 days (p < 0.001) (Fig. 1). Thus, in the absence of evidence of pathogen and clinical signs of inflammation, additional empiric antibiotic treatment is not mandatory. This underlines the importance of an aggressive radical surgical debridement to achieve a sufficient eradication of pathogens to ensure a complication-free wound healing. Shortening of the duration of antibiotic treatment, may prevent further increase of antimicrobial resistance, without inferior treatment results. This has recently been shown for several types of infectious diseases [65–67]. For determination of involved microorganisms and local resistance pattern, generous tissue collection during debridement is mandatory [29].
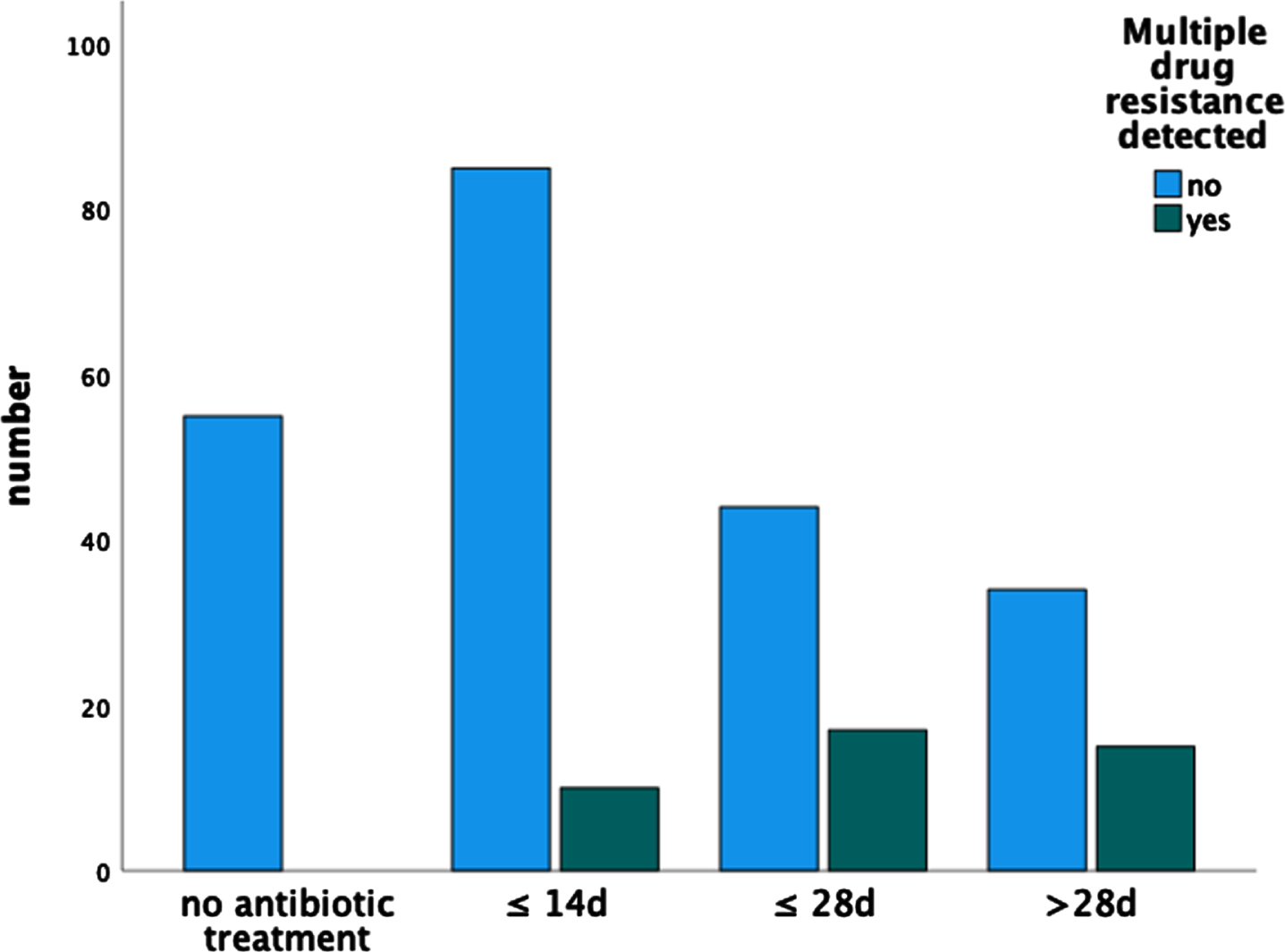
Number of multiple drug resistant pathogens without antibiotic treatment, up to 14 days, 28 days and over 28 days.
The weaknesses of this study are the retrospective evaluation with missing comparison groups a. In addition, this is a monocentric study. Furthermore, the specific regional spectrum of resistance represented in this study might not be generalizable to other cardiac and reconstructive surgical units. However, due to the large number of cases, important conclusions for future treatment in DSWI can be drawn from the above results.
In conclusion, the choice of antibiotics must take account of efficacy against Staphylococcus epidermidis and aureus. In our study, linezolid was a suitable antibiotic in the therapy of DSWI. In case of DSWI, radical debridement and knowledge of the local resistance pattern is the basis of successful treatment. There is no evidence of benefit from prolonged antibiotic therapy, in contrast the risk of resistance development increases. According to our results, prophylaxis with cephalosporins in cardiac surgery must be critically questioned.