
Abstract
Background and aims:
A deep sternal wound infection is a life-threatening complication after cardiac surgery. This study was conducted to describe the mortality associated with postoperative deep sternal wound infections after cardiac surgery and to find risk factors linked to increased mortality in 1 year follow-up.
Material and Methods:
A total of 7973 open-heart surgeries were performed at Tampere University Hospital. Deep sternal wound infection patients were identified, their 1-year mortality status was recorded, and the related risk factors were analyzed.
Results:
We detected a total of 129 (1.6%) postoperative deep sternal wound infection patients. The 1-year mortality associated with a postoperative deep sternal wound infection was 20.2%. No preoperative or perioperative, statistically significant factors associated with increased 1-year mortality were found. A prolonged stay in an intensive care unit after surgery as well as stroke, delirium, wound secretion, and co-infection were associated with increased 1-year mortality.
Conclusion:
The risk factors found for increased 1-year mortality were all postoperative. The quality of surgical treatment as well as precise postoperative care and evaluation remain the most important factors to decrease later mortality due to deep sternal wound infections.
Introduction
A deep sternal wound infection (DSWI) is a rare but life-threating complication after median sternotomy. The incidence varies between 0.4% and 2.5%.1,2 Coagulase-negative Staphylococci are the most common pathogen to cause a DSWI.3,4 The treatment of a DSWI consists of long-term antimicrobial treatment, often followed by a re-operation for mediastinal debridement. 4 Tissue flaps using plastic surgery techniques are often needed for reconstruction of the sternum.5,6 Many risk factors for a DSWI, including diabetes mellitus (DM), obesity, higher age, and peripheral arterial disease, have been recognized earlier.4,7
Although the risk factors and epidemiology of DSWIs are largely known, there is less knowledge about prognostic factors related to survival. Previous studies suggest that some of the established risk factors for a DSWI, including higher age, DM, and a higher preoperative risk of death, also seem to be prognostic of a poor outcome after the treatment of a DSWI.5,8 It is also reported that female sex, a longer intensive care unit (ICU) stay, co-infection, a long primary operation and the use of the internal thoracic artery (ITA) decrease the survival in the case of a DSWI.5,9–13
The aim of this study was to evaluate the incidence and mortality associated with postoperative DSWIs and to find factors that suggest a lethal treatment outcome in 1-year follow-up period.
Material and methods
This retrospective longitudinal single-center study data contain 7673 open-heart surgery patients treated with median sternotomy at Tampere University Hospital (Tays) during the 10-year study period between 1 January 2007 and 31 December 2016. The data were collected from the patient records of Tays Heart Hospital, and DSWI patients were identified in collaboration with the Tampere University Hospital’s infection register. DSWI was defined as a clinical wound infection combined with a positive microbiological samples from the sternotomy wound or in the blood culture or a macroscopic infection with pus in the mediastinum during reopening of the sternal wound. Primary microbiological findings and blood culture findings were collected from the first reoperation to minimize bias due to later contamination during the treatment of the infection. These findings were categorized into three different groups of micro-organisms: Staphylococcus aureus, coagulase-negative Staphylococci (CoNS) and other/negative. In addition, candida findings were collected.
All patients underwent the same preoperative preparative protocol during the study period. The protocol included the control of blood glucose, trimming of any facial hair and the identification and treatment of observed dental problems before surgery. The antibiotic prophylaxis, administered 1 h before the incision, constituted 3 g of intravenous cefuroxime given once. If the surgery continued longer than 4 h, supplementary doses of cefuroxime were administered every 4 h for as long as the surgery continued. All procedures were performed through a midline sternotomy.
If the signs or symptoms of DSWI occurred after the open-heart surgery, blood culture and microbiological samples from the wound were collected. Also, chest computer tomography (CT) scan was taken. The primary antimicrobial treatment was 1.5 g of intravenous cefuroxime administered in every 8 h. Cefuroxime is preferred as it covers the most common pathogens. Also, the antibiotic prophylaxis used in Tampere University Heart Hospital is short (usually single dose), and therefore, infection does not occur through the antimicrobial treatment. The antimicrobial treatment was corrected after the microbe and its sensitivity was analyzed, if necessary. The treatment also consisted of a reoperation for debris/pus removal from the mediastinum. The surgery was followed by secondary closure. During the study period, two surgical treatment modalities for DSWI were used in Tampere University Hearth Hospital. From the start, surgeons mostly used re-sternotomy accompanied with substernal flushing with drains and sternum rewiring, combined with intravenous antibiotic treatment. Later in the period, vacuum-assisted closure (VAC) was adapted as the first-line treatment for DSWI (Fig. 1). VAC-treatment included re-sternotomy, installation of VAC-device, and changes of the VAC-sponges generally every 2 days. VAC changes were continued repetitively until the wound swap cultures were negative, and there was no macroscopic infection in the sternal bone or mediastinum. If necessary, tissue flaps were applied for sternum reconstruction in cooperation with plastic surgeons.
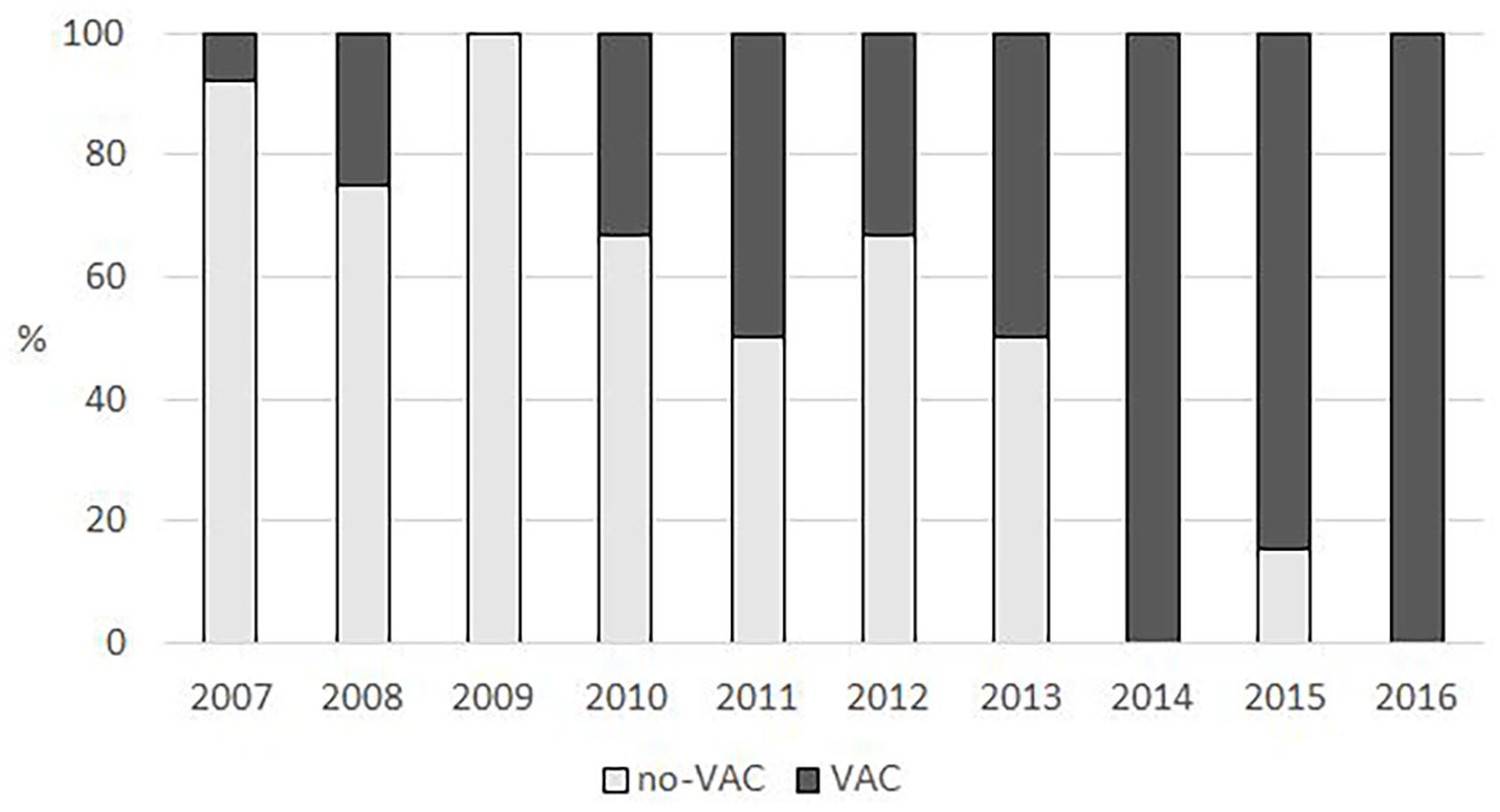
Proportion of DSWI treatment modalities between 2007 and 2016.
All patients were traced, and their survival status 1 year after the surgery was recorded and analyzed with the Kaplan–Meier method. Survival was further analyzed in univariate model by using Cox regression univariate analysis including either categorical (sex, obesity, smoking, peripheral arterial disease, diabetes, and New York Heart Association (NYHA) score) or continuous variables (age, EuroScore II, and left ventricle (LV) ejection fraction) as covariates to the mortality. Categorical variables were reported as counts and percentages. Continuous variables were reported using median and interquartile range (Q1–Q3). All statistical analyses were performed using IBM SPSS Statistics for Mac, version 26.0 (Armonk, NY, USA).
Results
There were a total of 129 DSWI patients between 2007 and 2016. Out of these, 103 (79.8%) were male. The patients’ age varied between 40 and 87 years, with a median of 71 years. The annual incidence of DSWIs showed no change over time, remaining steady at 1.6%. The median time between the primary open-heart surgery and the onset of the DSWI was 12 days. There were 26 deaths during the follow-up period of 1 year, and the overall 1-year mortality rate was 20.2% (Fig. 2). The annual mortality varied from 0.0% to 37.5%.
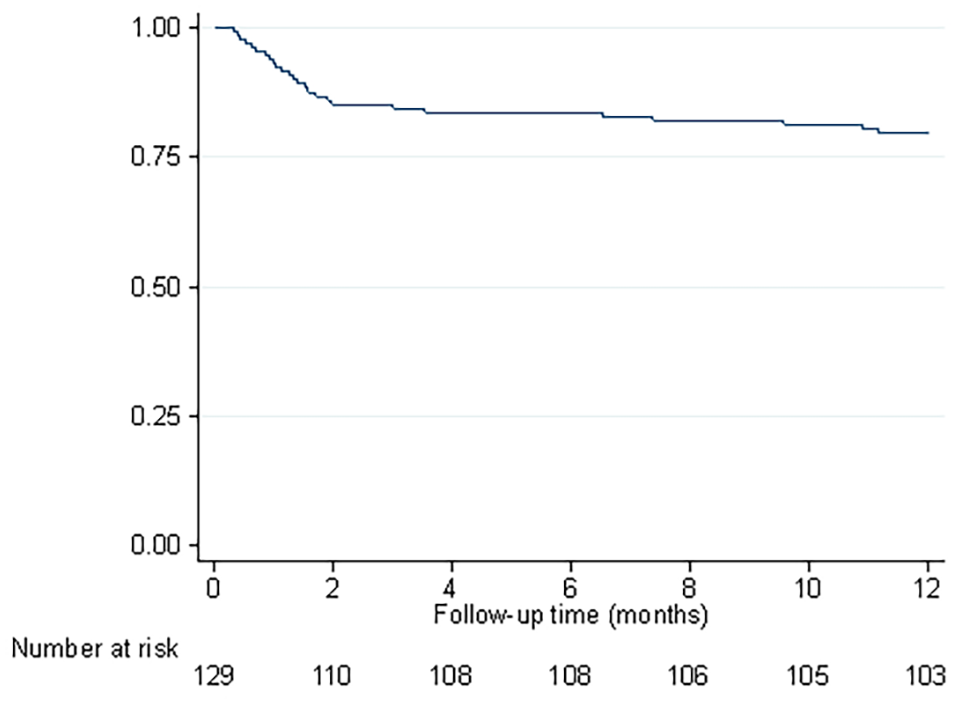
Postoperative 1-year survival of DSWI patients.
In the univariate analysis of preoperative characteristics, the median age was slightly higher among patients who died during the 1-year follow-up compared to survivors (75.5 and 71.0 years, respectively, p = 0.064). The preoperative factors showed no statistically significant differences between those who survived and those who died. There was a larger proportion of female patients among the patients who died, and the median EuroScore II was also higher among them. Equal proportions of the patients were smokers, and the median of the NYHA classification scores was also similar. Patients who did not survive the first year after surgery more frequently suffered from peripheral artery disease, and their median ejection fraction was lower. There were more obese patients (body mass index (BMI) ⩾ 30) and patients suffering from diabetes in those who survived (Table 1).
Characteristics of preoperative risk determinants and their effects on mortality in patients with a DSWI until the end of the follow-up period of 1 year in a univariate Cox proportional hazards regression model.
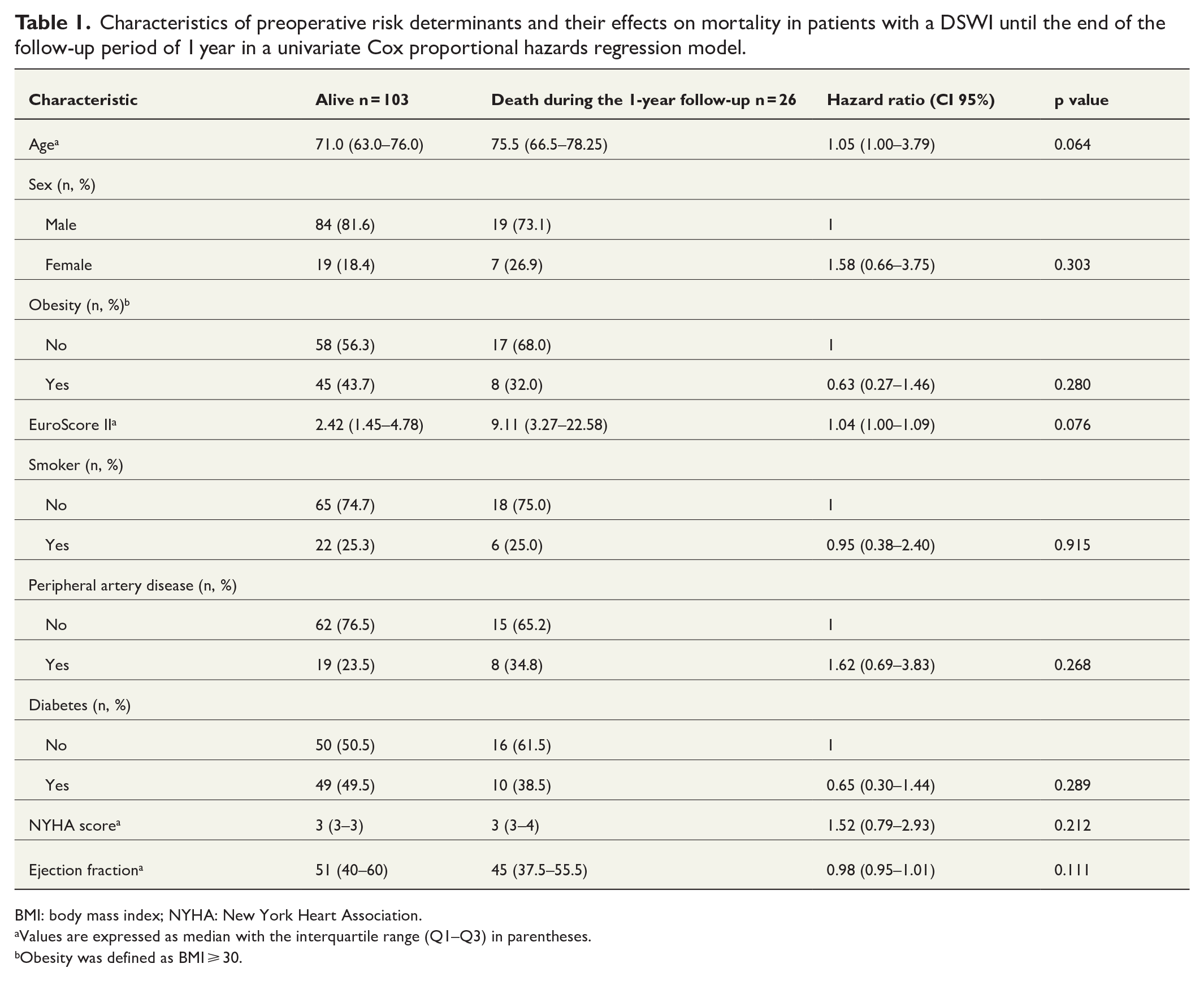
BMI: body mass index; NYHA: New York Heart Association.
Values are expressed as median with the interquartile range (Q1–Q3) in parentheses.
Obesity was defined as BMI ⩾ 30.
With regard to perioperative characteristics, there were no statistically significant differences between survivors and non-survivors. Closely equal proportion of patients went through an urgent or emergent surgery (65.4% vs 50.5%, p = 0.201) and the frequency of ITA graft use was roughly similar in both groups. The aortic cross clamp time did not differ between the groups and the type of the operations performed did not differ between the survivors and non-survivors (Table 2).
Characteristics of perioperative risk determinants and their effects on mortality in patients with a DSWI until the end of the follow-up period of 1 year in a univariate Cox proportional hazards regression model.
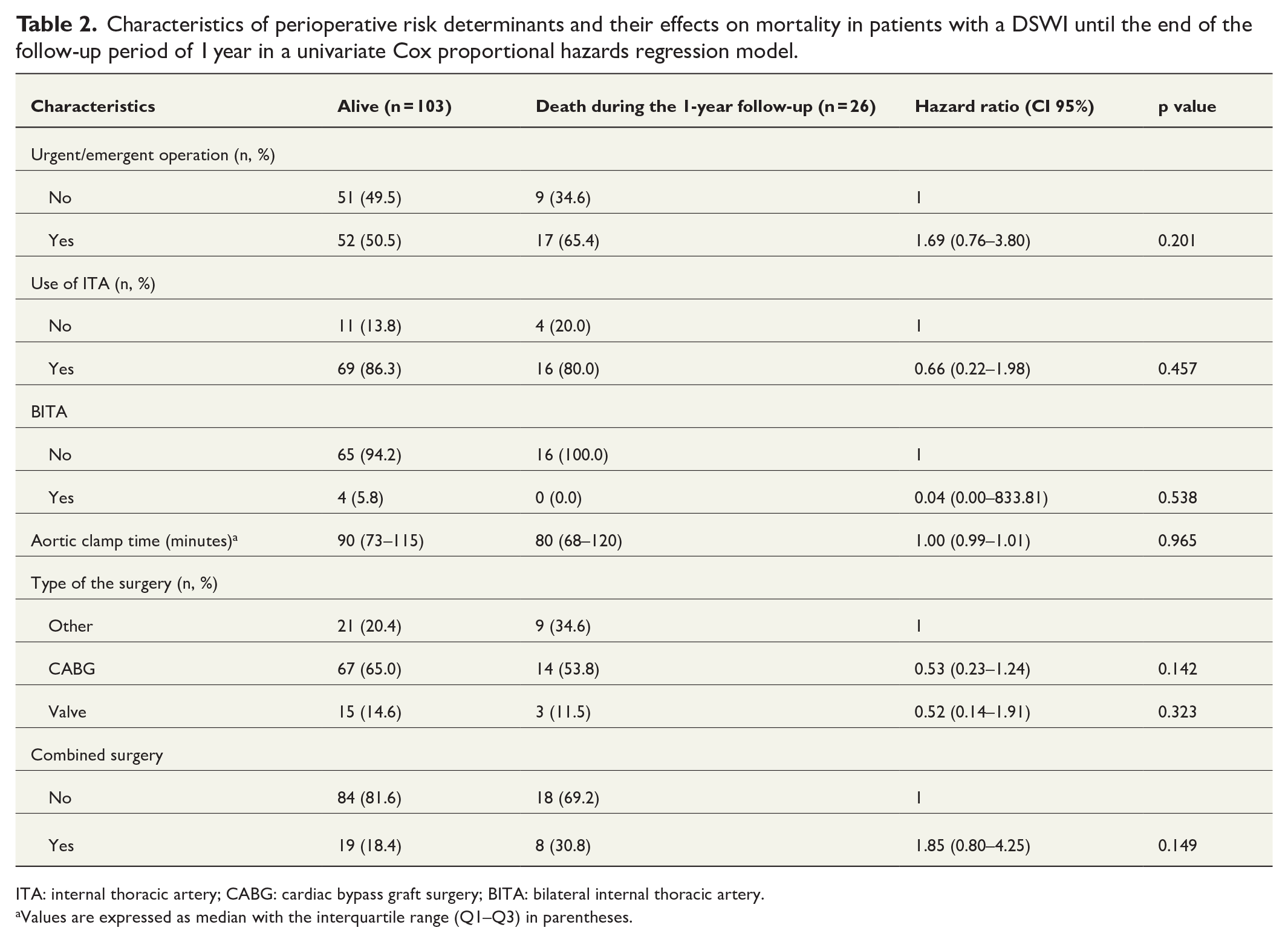
ITA: internal thoracic artery; CABG: cardiac bypass graft surgery; BITA: bilateral internal thoracic artery.
Values are expressed as median with the interquartile range (Q1–Q3) in parentheses.
With regard to the postoperative factors, we could find statistically significant differences between the survivors and the decreased. The median primary ICU stay was longer for the patients who died later during the study period (ICU stay 3 vs 1 days, p = 0.001). The non-survivors more often suffered a stroke (19.2% vs 5.9%, p = 0.037) and had more episodes of delirium during their treatment period (61.5% vs 32.4%, p = 0.008) than survivors. Furthermore, co-infection in any other anatomic region during the DSWI treatment was more common among the patients who died than among the survivors (43.5% vs 19.2%, p = 0.012). Reported wound secretion was seen more often among the non-survivors (84.0%) than in the surviving group of the patients (58.3%, p = 0.023). There were no statistically significant differences in the types of microbial pathogens in the wound culture findings for those who died and those who survived (Table 3).
Characteristics of postoperative risk determinants and their effects on mortality in patients with a DSWI until the end of the follow-up period of 1 year in a univariate Cox proportional hazards regression model.
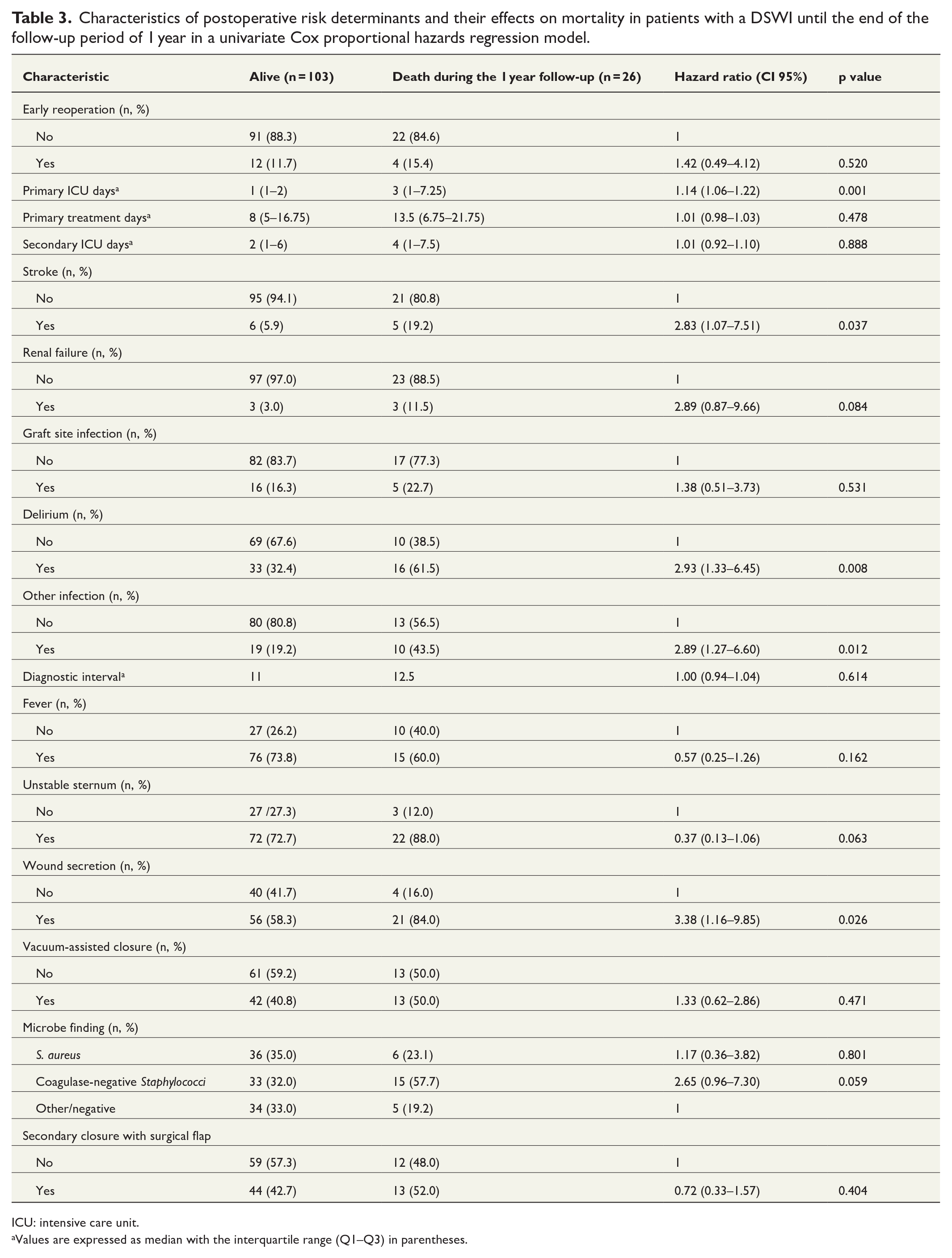
ICU: intensive care unit.
Values are expressed as median with the interquartile range (Q1–Q3) in parentheses.
The results of the pre-, peri-, and post-operative risk determinants have been summarized in Tables 1–3.
Discussion
This study intended to identify risk factors for poor 1-year outcome of DSWI treatment after open-heart surgery on unselected DSWI patients. The study includes a large single-institution material from Tampere University Heart Hospital, with a study population of 7673 patients during the 10-year study period. We observed risk factors for early mortality in DSWI patients.
To the best of our knowledge, publications on prognostic factors that promote later mortality among DSWI patients are scarce. This may be because the occurrence of postoperative DSWIs is low,1,2 which makes it a challenging topic of study. Some established risk-factors for a DSWI, including higher age at the time of the surgery, DM and a higher preoperative risk of death, have been suggested to promote a poor outcome in the treatment of a DSWI.5,8 These findings are in conflict with our results, as none of the above-mentioned factors were associated with an increased risk of 1-year mortality in our study population. Also, it is not clear which DSWI-derived factors really affect later survival, and the co-existing cardiovascular conditions tend to cause competing causes of death. A higher number of primary ICU days, a stroke during the treatment, delirium, infection in another anatomical region and wound secretion emerged as risk-factors for a poor outcome in our study population. Previous studies suggest a longer ICU stay and co-infection to be risk-factors for a poor outcome, which is in line with our results.11,12
An infection in another anatomical region was associated with increased 1-year mortality in our cohort. In the study by Lepelletier et al., the results were similar to those of our study. Especially pneumonia caused by a mechanical ventilator increased the mortality risk significantly. 11 In our material, we observed a prolonged primary ICU stay to be linked to increased mortality in DSWI patients. Patients with a prolonged ICU stay are kept on the mechanical ventilator longer, which could further lead to an increased frequency of pneumonia in the DSWI patients. Furthermore, a prolonged ICU stay could lead to an increased number of delirium episodes as patients receive several and intense medications and may have a compromised nutritional status. A prolonged primary ICU stay may result from a complication during the surgery or from a poor general condition before surgery. We cannot emphasize the importance of elaborate surgical care and preoperative preparations enough, as these factors affect the outcome of surgery considerably.
Wound secretion was defined as pus or debris secretion from the sternal wounds at any time during the treatment. It was associated with increased mortality related to DSWI. There are factors which could explain this result. If the secretion is the first clinical sign observed before starting the DSWI treatment, it may suggest that the infection has progressed further, the sternum has separated, pericardial fluid has entered the wound and a macroscopic deep infection has also occurred. There was no significant difference in the diagnostic interval between the groups in our material. If the secretion occurs after the beginning of the antimicrobial treatment and reoperation, the primary antibiotic chosen may not have been effective for the pathogen causing the infection. This may lead to a further progression of the infection, as the initiation of effective treatment is delayed. We do not have data on the sensitivity of the microbes isolated prior to the empirical antimicrobial treatment. However, cefuroxime was the first-line antibiotic of choice in our regimen for postoperative DSWIs before sensitivity analyses were available. Patients could also have a compromised immune response due to an unknown reason. This again may lead to a further progression of the infection, but we had no means of investigating the immune status prior to surgery.
The difference between the results of our study and the previous studies could be explained with potential differences in the protocols of cardiac surgery and treatment regimens of DSWIs between different institutions. When it comes to dental hygiene and care, the protocol at Tampere University Heart Hospital is strict. Only emergent surgeries are performed without first addressing potential dental problems, such as caries and gingivitis. Other institutions may have different protocols in this regard. The differences in treatment protocols for DSWIs could also explain the observed differences to other earlier studies. At Tampere University Heart Hospital, vacuum-assisted closure combined with antimicrobial treatment is the primary choice of DSWI treatment, and previous studies suggest that it may reduce the mortality associated with DSWIs.7,14 It was adopted as the primary treatment protocol during the study period, and approximately 43% of the patients were treated with vacuum-assisted closure. Vacuum-assisted closure treatment did not have impact on the 1-year mortality, as was also shown in another study. 15 Instead, VAC-treatment increased the treatment time in the hospital wards and in the ICU. 16 In our institution, a heart team approach to decision-making was adopted early on, including interventional and conservative cardiologists, cardiac surgeons and cardiothoracic anesthetists, who plan the surgical treatment and, when necessary, the treatment of any related complications. This multi-professional cooperation is thought to improve the outcome, as several professionals address the cardiac surgical problem from different points of view.
The strength of this study was a relatively large study population compared to previous studies, as well as a long follow-up time and study period. An important observation was the increasing effect of a prolonged primary ICU stay on mortality. This highlights the importance of careful preoperative preparations and of the procedure itself to keep the rate of surgical complications low and further to decrease the mean time spend in an ICU after surgery.
The retrospective approach can be considered as a limitation of this study, exposing it to bias. We managed and minimized the pre-trial bias by triple-checking that patients had a DSWI. We used three different sources of data collection to verify the DSWI diagnosis. Also, we included all patients diagnosed with a postoperative DSWI in our analyses, which makes our study population reasonably comparable with other cardiac surgical institutions in Western countries, particularly those in Northern Europe. The endpoint of this study was death within 1-year from the primary surgery. In Finland, as in other Nordic Countries, complete information concerning all deaths of Finnish residents is collected into a national population register. Furthermore, emigration from Finland is minor. This makes complete follow-up as regards mortality possible.
In this study, we found a fairly steady incidence of DSWI and DSWI-associated mortality after cardiac surgery during 2007–2016 in a single-center tertiary cardiac care center in Finland. We found significant risk factors that are associated with mortality in DSWI patients. Some of the discovered risk factors can be controlled with specific treatment. Hopefully, these findings also lead to better a prognosis for DSWI patients.
Footnotes
Acknowledgements
The authors kindly acknowledge the skillful work of their research coordinator Kati Helleharju at Tampere University Heart Hospital.
Author contributions
Eero Hämäläinen: Study concept, study design, data acquisition, statistical analysis, writing of original draft, review and editing of manuscript.
Jari Laurikka: Study concept, study design, review and editing of manuscript, supervision.
Heini Huhtala: Statistical analysis, review and editing of manuscript.
Otso Järvinen: Study concept, study design, data acquisition, review and editing of manuscript, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the City of Tampere science grant committee.