
Abstract
BACKGROUND:
Hepatocellular carcinoma (HCC) is the sixth most common malignant tumor and second most common cause of tumor-related deaths worldwide. Activated platelets play a prominent role in tumor. Platelet distribution width (PDW) indicates platelets activation and is altered in malignancies. The aim of this study was to explore the prognostic value of PDW for overall survival (OS) in HCC patients.
METHODS:
We retrospectively reviewed 273 HCC patients at a single institution from 2010 to 2014. The relationship between PDW and clinicopathological characteristics was analyzed. Kaplan-Meier curves and multivariate Cox regression analyses were used to evaluate the relationship of PDW with OS.
RESULTS:
Low PDW levels were observed in 127 (46.5%) out of 273 patients. A significant correlation was found between PDW and liver cirrhosis. Median follow-up was 36 months, survival curves revealed that the patients with increased PDW had significantly shorter survival time than those with normal PDW (
CONCLUSION:
PDW is significantly associated with OS in HCC. This result suggests activated platelet may affect clinical outcome and warrant continued investigation.
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common malignant tumor and second most common cause of tumor-related deaths worldwide [1, 2]. Although surgical resection and liver transplantation are still the best options for HCC patients, the overall 5-year survival rate remains low due to high postoperative recurrence rate and metastasis [3, 4]. Thus, there is an urgent need of discovering new biomarkers aiding in prognosis and developing curative strategies against HCC.
There is abundant evidence that platelets are associated with tumor development and tumor progression. Pretreatment thrombocytosis is a poor prognostic factor as well and reflects aggressive tumor behavior in malignant mesothelioma, cervical, colon, and non-small cell lung cancer patients [5, 6]. There are accumulated data on the substantial influence of blood platelets in the process of blood vessel formation during malignancy [7]. Moreover, platelets contribute to early and late stages of angiogenesis through platelet-derived microparticles, microRNA, lipids, and variety of surface receptors [7].
Platelet distribution width (PDW), a platelet marker, indicates variation in platelet size [8]. Elevated PDW levels were associated with poor prognosis in a variety of tumors, such as gastric cancer, non-small cell lung cancer, laryngeal cancer, and melanoma [9, 10, 11, 12]. However, the clinical implication of PDW in HCC has not been well defined.
The current study aims to test whether pretreatment PDW could predict survival in HCC patients.
Methods
Study population
The present study retrospectively reviewed the clinical data of 273 patients histologically diagnosed with HCC from Harbin Medical University Cancer Hospital between January 2010 and December 2014 (Harbin, China). All patients underwent surgical resection. None of the patients received any adjuvant therapy before resection. We excluded patients with hematological disorders, hypertension, diabetes mellitus, and medical treatment with anticoagulant therapy, statins, and acetylic salicylic acid. Overall survival (OS) was defined as the interval from the date of diagnosis to date of death or last follow-up. Follow-up evaluations were performed every 3 months. Follow-up was completed on December 31, 2017. The follow-up duration was 36 months.
The clinicopathohistological data including age, sex, HbsAg, liver cirrhosis, tumor size, tumor number, tumor differentiation, regional lymph node metastasis, Child-pugh’s grade, and the therapy administered were all collected through medical records. Enhanced computed tomography or magnetic resonance imaging was performed to rule out distant metastases. In case of multiple tumors with different size, largest diameter was used. Cirrhosis was diagnosed based on the data from history or on a combination of endoscopic or radiological evidence, or of portal hypertension. All patients were confirmed to have liver cirrhosis by pathologic assessment at the time of surgery. The status of lymph nodes larger than 4.0 mm was reported pathologically. The removed lymph nodes were pathologically confirmed to be classified into a metastatic group or non-metastatic group. The information on blood tests was obtained from the test report from the Department of Clinical Laboratory at the Harbin Medical University Cancer Hospital. The normal range for
The present study is a retrospective study and was reviewed and approved by the Institutional Ethics Review Board of Harbin Medical University Cancer Hospital. All patients provided written informed consent.
Statistical analysis
Data are expressed as the mean
The ROC curve for PDW. The optimized cut-off value for PDW using standard ROC curve analysis.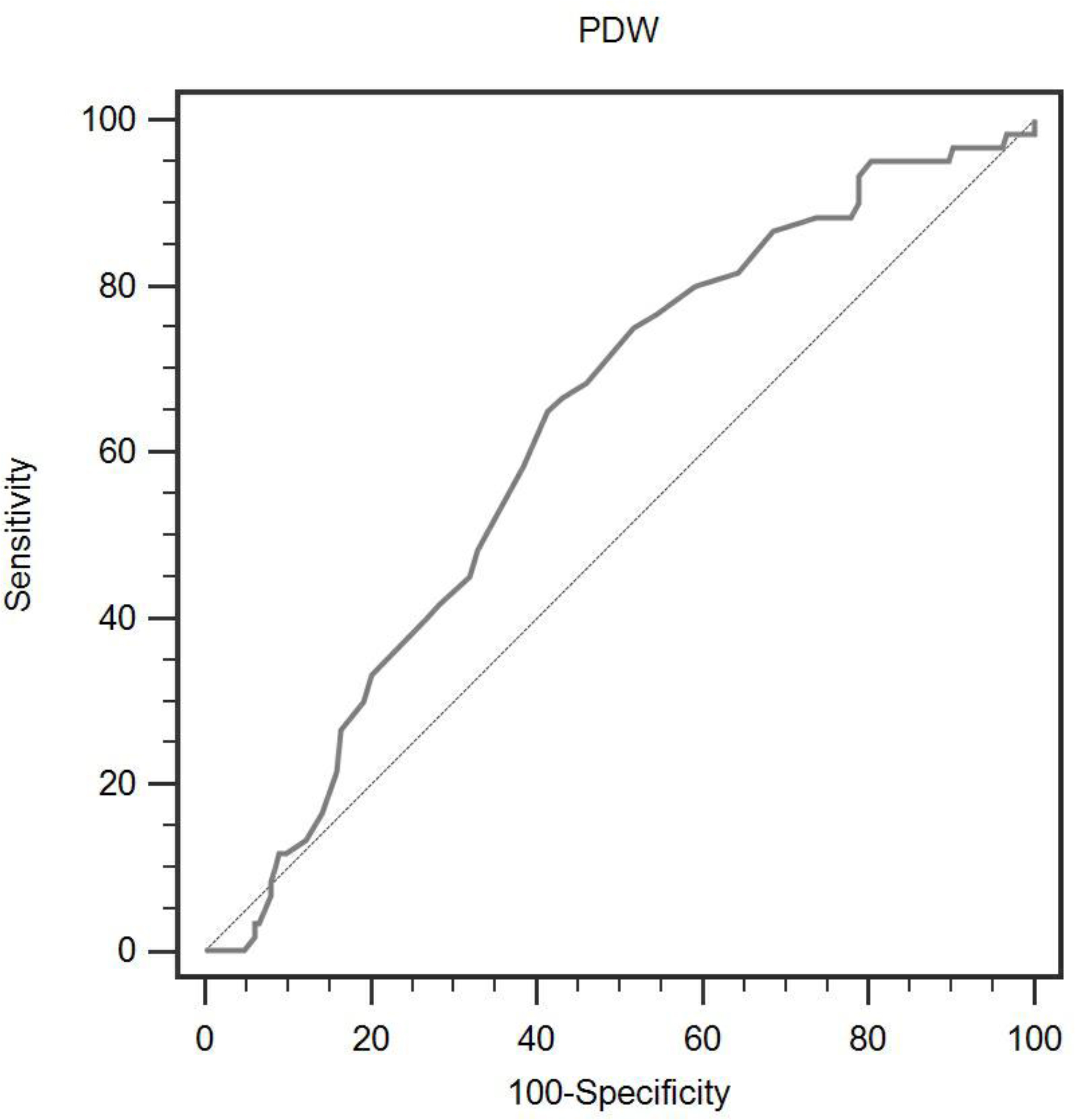
Baseline characteristics of HCC patients according to PDW levels
HCC, hepatocellular carcinoma; AFP,
Baseline characteristics of HCC patients according to PDW levels
Data are expressed as means (SD) or median (IQR). BMI, body mass index; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, gamma-glutamyl transpeptidase; TBIL, total bilirubin; FPG, fasting plasma glucose; WBC, white blood cell; RDW, red cell distribution width; NLR, neutrophil-to-lymphocyte ratio; MPV, mean platelet volume.
The univariate and multivariate analysis of overall survival in HCC patients
Variables that showed a
Among the 273 patients, the mean age was 52.5
According to the ROC curve analysis, we identified that the optimal cut-off value of 17.1 for PDW had a 65.0% sensitivity and 58.7% specificity for survival rate (
The relationships between PDW and clinical characteristics were summarized in Tables 1 and 2. Our study found that PDW was significantly associated with platelet count, WBC, and liver cirrhosis. However, there were no significant differences between the groups in terms of age, gender, smoking status, drinking status, BMI, hemoglobin, AFP, HbsAg, tumor size, tumor number, tumor differentiation, and regional lymph node metastasis.
With a follow up of 36 months, 60 (22.0%) patients had death events. Patients with
The correlation between PDW levels and overall survival in patients with HCC. The cumulative incidence of overall survival is significantly higher in patients with low PDW levels.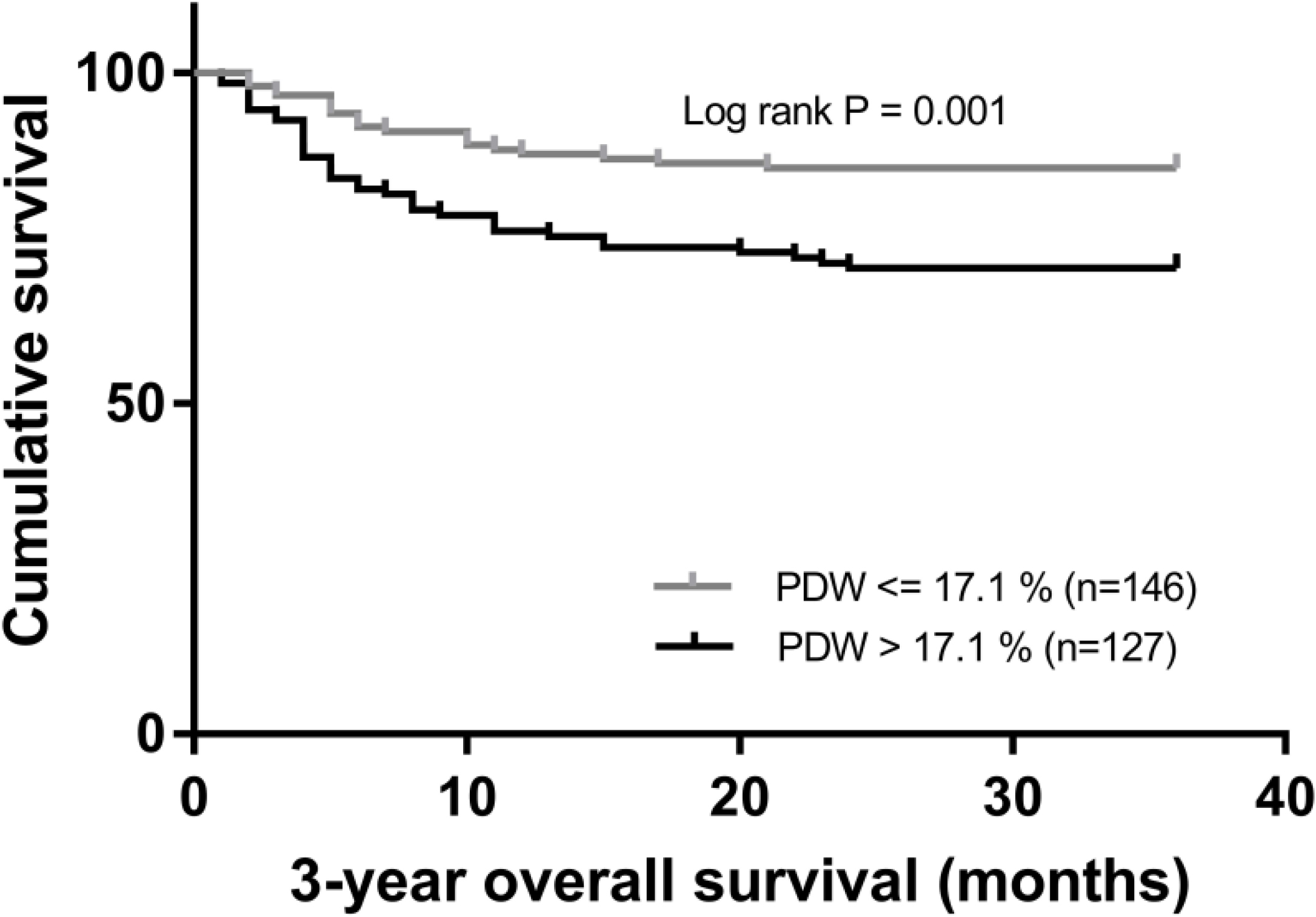
Cox univariate and multivariate regression analyses were performed for the factors that could impact survival. GGT, WBC, PDW, neutrophil-to-lymphocyte ratio, tumor size, regional lymph node metastasis, tumor differentiation, and Child-pugh’s grade were determined to be significant in univariate analyses. AFP showed weak associations. Other parameters were not found to be in correlation with OS (Table 3). Next, all the factors with a
Here is the first study to investigate the prognostic value of preoperative PDW in HCC. We revealed that increased PDW was associated with liver cirrhosis. In addition, elevated PDW was an independent indicator of overall survival in HCC.
Despite new advances in treatment, the 5-year survival of HCC patients after resection ranges between 50% and 70% with high recurrence rate and metastasis [3, 4]. Therefore, it is of great importance in identifying novel prognostic factors. More and more evidence has emerged showing a pro-metastatic role of platelets in cancer [13].
Activated platelets inhibit hepatocellular carcinoma cell differentiation and promote tumor progression via platelet-tumor cell binding [14]. Platelet granule contents promote the proliferation of HCC cells by suppressing the expression of Kruppel like factor 6 [15]. Clinical studies found that platelet-derived endothelial cell growth factor is an angiogenic factor and increased in HCC patients [16]. Moreover, a recent report confirmed that platelet-derived growth factor receptor alpha overexpression is a prognostic marker independent of liver fibrosis status in HCC [17]. Furthermore, antiplatelet therapy delays immune-mediated hepatocarcinogenesis and improves survival in a mouse model of chronic hepatitis B [18].
In accordance with the studies above, our report indirectly confirmed the results using a simple platelet marker. Furthermore, our study can form the basis for further mechanistic studies and ultimately help clinicians with better individualization of their therapeutic strategy.
The biologic mechanisms underlying the correlation between PDW and prognosis in HCC remains poorly understood. Altered PDW maybe related to bone marrow cells (including megakaryocytes) dys-function. PDW is a measure of platelet heterogeneity caused by heterogeneous demarcation of megakarocytes [19]. Recent reports found that several cytokines, such as interleukin-6 (IL-6), granulocytes colony stimulating factor (G-CSF) and macrophage colony stimulating factor (M-CSF), regulate megakaryocytic maturation, platelet production and platelet size [20]. IL-6 promotes tumor angiogenesis, metastasis and metabolism [21]. In addition, G-CSF and M-CSF secreted by tumor cells stimulate megakaryopoiesis and subsequent thrombopoiesis in cancer [22].
This study has several limitations. First, this study had a retrospective design and included a relatively small number of patients. Second, the mechanisms underlying the involvement of PDW in HCC should be clarified. Third, this study lacked of internal/external validation. Finally, the patients were composed of Chinese. Multicenter prospective studies with larger samples are needed to verify our results.
In conclusion, increased PDW may predict the clinical outcomes of HCC patients. Further studies are warranted.
Footnotes
Acknowledgments
This work was supported by grants from the Harbin Medical University Cancer Hospital (JJZD2017-05) and from Nn10 program of Harbin Medical University Cancer Hospital.