Modeling the time-related fluctuations of AFP and PIVKA-II serum levels in patients with cirrhosis undergoing surveillance for hepatocellular carcinoma
Free accessResearch articleFirst published online May, 2020
Modeling the time-related fluctuations of AFP and PIVKA-II serum levels in patients with cirrhosis undergoing surveillance for hepatocellular carcinoma
The time-related variability of HCC biomarkers has not been investigated so far.
OBJECTIVE:
To assess the changes of alpha-fetoprotein (AFP) and protein induced by vitamin-K absence/antagonist-II (PIVKA-II) in patients with HCC (HCC) as compared to patients without HCC (HCC).
METHODS:
AFP and PIVKA-II were measured by a single laboratory using an automated chemiluminescent-enzyme-immunoassay (Fujirebio Inc., Tokyo, Japan) in 1163 sera of 418 cirrhotics (31.1% HBV, 58.6% HCV, 10.3% non-viral etiology) undergoing ultrasound HCC surveillance. The mean (range) number of effective time-points available for analysis was 2.8 (2.0 to 3.0); 124 patients with HCC were matched with 294 who remained HCC free for at least 12 months after the last specimen. AFP and PIVKA-II changes were estimated over time by means of a random-effect generalized least squares (RE-GLS) regression model under the missingness at random assumption.
RESULTS:
Patients with and without HCC had comparable chronic liver disease etiology and staging. AFP/PIVKA-II median (25; 75 percentile) values at the latest time-point were 4.2 (2.6; 8.6) ng/mL/32 (25; 42) mAU/mL in HCC and 8.4 (4.4; 32.1) ng/mL/66 (32; 192) mAU/mL in HCC ( 0.001). LogAFP and logPIVKA-II time-changes differed in HCC and HCC patients. In HCC patients, both logAFP and logPIVKA-II showed an increasing trend over time. In HCC patients, logPIVKA-II variations were minimal as compared to logAFP variations. The percent increase of logAFP at 6 months vs. baseline was 11% (95%CI 5 to 17%) and 5% (95%CI 1 to 8%) for logPIVKA-II in HCCvs. HCC patients.
CONCLUSIONS:
The present retrospective study of the biological variability of AFP and PIVKA-II suggests that their time-related changes may serve as potential predictors of HCC. This topic needs to be addressed by longitudinal studies.
Hepatocellular carcinoma (HCC) has a worldwide incidence ranging from 5 to 20 per 100,000 individuals and is the 5 most common cancer in men and the 9 in women [1, 2, 3]. The incidence rate 1.5% per year in at-risk populations such as cirrhotic patients recommends performing surveillance and several evidences suggest that early diagnosis improves HCC management [4].
HCC surveillance is mainly based on ultrasound scan (US) whose effectiveness is highly operator-dependent [4, 5, 6, 7]. Alpha-fetoprotein (AFP) and protein induced by vitamin-K absence/antagonist-II (PIVKA-II) are the best available circulating biomarkers for the diagnosis of HCC [8, 9, 10, 11]. However, they have some limitations as diagnostic tools for HCC because the etiology and the activity of the undergoing liver disease affect their diagnostic performance [12, 13]. To date there is no agreement among international guidelines about the use of biomarkers in HCC surveillance; they are not recommended by the European Association for the Study of the Liver (EASL) [6], while AFP testing every six months can be performed together with periodic US according to the American Association for the Study of Liver Disease (AASLD) [4].
AFP serum levels are influenced by liver regeneration following necrosis and inflammation [14] and fluctuate differently in patients with active liver disease and in those responding to antiviral therapy. PIVKA-II is an immature form of prothrombin whose serum levels increase in the presence of HCC following a defect in a post-translational vitamin-K-dependent carboxylation of ten glutamic acid residues at the amino-terminal [15]. Although PIVKA-II shows a higher specificity to HCC ( 80%), the presence of factors affecting the cycle of vitamin-K, such as drugs or impaired absorption, can lead to non-specific elevations [16].
As a consequence, the fluctuations of these biomarkers in several pathophysiological non-malignant conditions can be relevant and the identification of specific univocal cut-offs to detect HCC might be suboptimal because of their biological variability. More recently, some studies have shown that the analysis of single-point continuous values of HCC biomarkers by means of statistical models could improve the diagnostic accuracy rather than the application of specific cut-offs [17, 18]. However, the use of serial measures of biomarkers might improve their performance for HCC screening since multiple testing would allow to compute their kinetics and the magnitude and rate of their change over time. Both the kinetics and the rate of change of the biomarkers’ serum levels over time (velocity) might have advantages over a single measurement in differentiating patients with cirrhosis and benign regeneration nodules from patients with nodules progressing to HCC.
The aim of the present case-control study was to assess the time-related variations of serum AFP and PIVKA-II levels in cirrhotic patients who did or did not develop HCC during surveillance.
Patients and methods
Study design
We performed a retrospective repeated-measure case-control study on cirrhotic patients undergoing surveillance for HCC. Cases were patients with HCC development and controls were patients who had not developed HCC for at least 12 months from the last available serum sample. We enrolled 418 consecutive cirrhotic patients with chronic liver disease (CLD) of different etiology undergoing HCC surveillance in three Italian Hepatology centers [200 (47.8%) in Pisa, 162 (38.8%) in Naples, 56 (13.4%) in Padua] for whom at least two serum samples were available. In 124 patients with HCC development (HCC) one serum specimen was obtained at the time of HCC diagnosis and one or two serum specimens were available before HCC diagnosis. Two or three serum specimens were available also from the remaining 294 patients who did not developed HCC for at least 12 months after the collection of the last serum (HCC). Liver cirrhosis was diagnosed at histology or based on unequivocal ultrasound/transient elastography/endoscopic features (liver morphology suggestive of cirrhosis, esophageal varices and/or other signs of portal hypertension) and/or clinical history of liver decompensation (ascites and/or hepatic encephalopathy). HCC was diagnosed on the basis of a typical vascular pattern of focal liver lesions obtained at imaging [computed tomography (CT), magnetic resonance imaging (MRI), contrast-enhanced ultrasound imaging (CEUS)], according to the EASL current guidelines for HCC [6]. The study was approved by the local Ethical Committee and conforms with The Code of Ethics of the World Medical Association (Declaration of Helsinki). All patients gave their written informed consent.
Laboratory assessment
Sera were stored at 20C until they were tested for AFP and PIVKA-II by means of two quantitative fully automated chemiluminescent-enzyme-immunoassays (CLEIA) on Lumipulse G1200 (Fujirebio Inc., Tokyo, Japan). The analytical sensitivity of the method was 0.8 ng/mL for the AFP assay (dynamic range 0.8 to 22451 ng/mL and upper normal limit 7.4 ng/mL) and 1.37 mAU/mL for the PIVKA-II assay (dynamic range 1.37 to 75000 and upper normal limit 48 mAU/mL). The coefficient of variation (CV) is 3.3% for AFP and 4.0% for PIVKA-II measurement [19]. All tests were performed in a single run at the reference laboratory of the University Hospital of Padua. Samples with results exceeding the dynamic range values were retested following appropriate dilution.
Statistical analysis
Most continuous variables were not Gaussian- distributed and reported as median (25; 75 percentile). Categorical variables are reported as numbers and proportions. Differences between HCC and HCC were analyzed using median regression and Pearson’s Chi-square test for continuous and categorical variables, respectively. The time-related changes of AFP and PIVKA-II in cases (HCC) and controls (HCC) were retrospectively estimated using a random-effect generalized least squares (RE-GLS) regression model [20]. The response variable of the RE-GLS model were log-transformed AFP or log-transformed PIVKA-II. The log-transformation was used to reduce the expected skewness of the response variable. The pre-specified predictors of the RE-GLS model were time (continuous, years), squared time (continuous), HCC (dichotomous, 0 no; 1 yes), an HCC*time (dichotomous*continuous) interaction, and an HCC*squared time (dichotomous*continuous) interaction. The RE-GLS model was pre-specified because this is the best strategy to test a study hypothesis via regression analysis [20]. In particular, we did not explore other transformations of time besides squared time because of the availability of just three time-points and of the varying distance between them. Coherently with the pre-specified nature of the model, predictors were kept into it independently of their statistical significance [20]. It should be noted that, in the presence of significant interactions, the main effects cannot be interpreted as such and estimates made by the regression model have to be used [20]. We plotted these estimates to aid the clinical interpretation of the findings. The random effect of the RE-GLS was assigned to the patient. Internal cross-validation was performed using bootstrap on 1000 samples with replacement. This is expected to correct for over-optimism and make the model more generalizable [20]. We also run the RE-GLS model using the study center as cluster (0 Pisa; 1 Naples; 2 Padua), i.e. by bootstrapping the patients with replacement within each center [20] but this did not change the findings and is not reported here. The RE-GLS is robust to missing data provided that they are missing at random, which is a reasonable assumption for the present study. The mean (range) number of effective time-points available for analysis was 2.8 (2.0 to 3.0) for both logAFP and logPIVKA-II. Bootstrapped 95% confidence intervals (95% CIs) are reported for the regression coefficients and the estimates obtained from the RE-GLS model [20]. Statistical analysis was performed using Stata 15.1 (Stata Corporation, College Station, TX, USA).
Main characteristics of HCC cases
(%) or median (25; 75 percentile)
Sex
F
21 (16.9)
M
103 (83.1)
Age at diagnosis
Years
65.9 (59.5; 72.7)
Center
Pisa
93 (75.0)
Naples
23 (18.5)
Padua
8 (6.5)
Etiology
HBV
37 (29.8)
HCV
75 (60.5)
Non-viral
12 (9.7)
Child-pugh score
5 (5; 5)
Child-pugh class
A
115 (92.7)
B
9 (7.3)
Description HCC
Single nodule
102 (82.3)
2–3 nodules
17 (13.7)
3 nodules/diffuse
5 (4.0)
Max diameter lesion
mm
21 (8; 120)
BCLC stage
0
50 (40.3)
A
51 (41.1)
B
2 (1.6)
C
12 (9.7)
D
9 (7.3)
Notes: BCLC: Barcelona Clinic Liver Cancer.
Demographic and laboratory data
HCC ( 294)
HCC ( 124)
Overall ( 418)
values
Sex
F
77 (26.2)
21 (16.9)
98 (23.4)
0.056
M
217 (73.8)
103 (83.1)
320 (76.6)
Etiology
HBV
93 (31.6)
37 (29.8)
130 (31.1)
0.880
HCV
170 (57.8)
75 (60.5)
245 (58.6)
Non-viral
31 (10.5)
12 (9.7)
43 (10.3)
Center
Pisa
107 (36.4)
93 (75.0)
200 (47.8)
0.001
Naples
139 (47.3)
23 (18.5)
162 (38.8)
Padua
48 (16.3)
8 (6.5)
56 (13.4)
Age
(Years)
63.5 (56.5; 69.7)
65.9 (59.5; 72.7)
64.2 (56.7; 70.8)
0.019
AFP
(ng/mL)
4.2 (2.6; 8.6)
8.4 (4.4; 32.1)
5.0 (3.0; 10.2)
0.001
PIVKA-II
(mAU/mL)
32 (25; 42)
66 (32; 192)
35 (26; 61)
0.001
AST
(U/L)
26 (22; 36)
43 (25; 78)
29 (22; 46)
0.001
ALT
(U/L)
22 (17; 33)
34 (22; 83)
26 (18; 47.2)
0.001
GGT
(U/L)
31 (19; 57)
60 (33; 105)
38 (22; 74.7)
0.001
ALP
(U/L)
77 (62; 98)
103 (82; 133)
85 (65; 115.5)
0.001
Albumin
(g/dL)
4.3 (4.0; 4.5)
4.1 (3.8; 4.4)
4.2 (3.9; 4.5)
0.038
PT
(%)
82 (60; 97)
83 (73; 93)
82 (68.2; 94)
0.439
INR
1.10 (1.02; 1.24)
1.11 (1.06; 1.21)
1.10 (1.03; 1.21)
0.531
Total bilirubin
(mg/dL)
0.96 (0.60; 1.48)
0.79 (0.59; 1.20)
0.90 (0.59; 1.37)
0.195
PLTs
( 10/L)
120 (89; 165)
111 (77; 155)
114 (82; 157)
0.198
Child-pugh score
5 (5; 5)
5 (5; 5)
5 (5; 5)
0.674
Child-pugh class
A
272 (92.5)
115 (92.7)
387 (92.6)
0.940
B
22 (7.5)
9 (7.3)
31 (7.4)
Notes: AFP, alpha-fetoprotein; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; INR, International normalized ratio; PIVKA-II, Protein induced by Vitamin K Absence/Antagonist-II; PT, Prothrombin time; PLTs, platelets. Laboratory data refer to the last serum specimen collected. Continuous variables are reported as median (25; 75 percentile).
Results
Patients characteristics
Four hundred and eighteen patients were selected for the present study: 124 HCC cases and 294 HCC controls. The main characteristics of HCC cases are reported in Table 1. The majority of HCC were diagnosed at a very early or early stage [BCLC 0 in 50 (40.3%), BCLC A in 51 (41.1%)]. Demographic and laboratory data are reported in Table 2 stratified by HCC status. Continuous variables are expressed as median (25; 75 percentile) and refer to the last serum specimen collected, which is the nearest to the diagnosis in patients who developed HCC. HCC patients were 93/200 (46.5%) in Pisa, 23/162 (14.2%) in Naples and 8/56 (14.3%) in Padua. Men were more common than women both among HCC (103/124, 83.1%) and HCC patients (217/294, 73.8%). The etiology of chronic liver disease was HBV in 37 (29.8%) of HCC and 93 (31.6%) of HCC patients; HCV in 75 (60.5%) of HCC and 170 (57.8%) of HCC patients; non-viral in 12 (9.7%) of HCC and 31 (10.5%) of HCC patients.
AFP and PIVKA-II serum levels were higher in HCC than HCC ( 0.001). HCC patients showed higher levels of liver enzymes and albumin. Nevertheless, the majority of patients showed a preserved liver function (Child-Pugh A in 92.6%), without differences between groups (92.5% in HCC and 92.7% in HCC).
Modeling analysis
A total of 1163 serum samples were evaluated. Two serum samples were available for 91 patients (29 HCC and 62 HCC) and three for 327 patients (95 HCC and 232 HCC). The median (minimum; maximum) time elapsed between the first and the last serum collection was 13.1 (3.2; 96.0) in HCC and 22.8 (2.0; 74.5) months in HCC patients.
The median (minimum; maximum) time at which the last serum specimen was collected in the 124 HCC patients was 0.1 (3.6; 4.7) months within the diagnosis of HCC. The 297 HCC patients remained free from HCC for a median (minimum; maximum) time of 14.2 (12.1; 71.7) months after the last serum specimen.
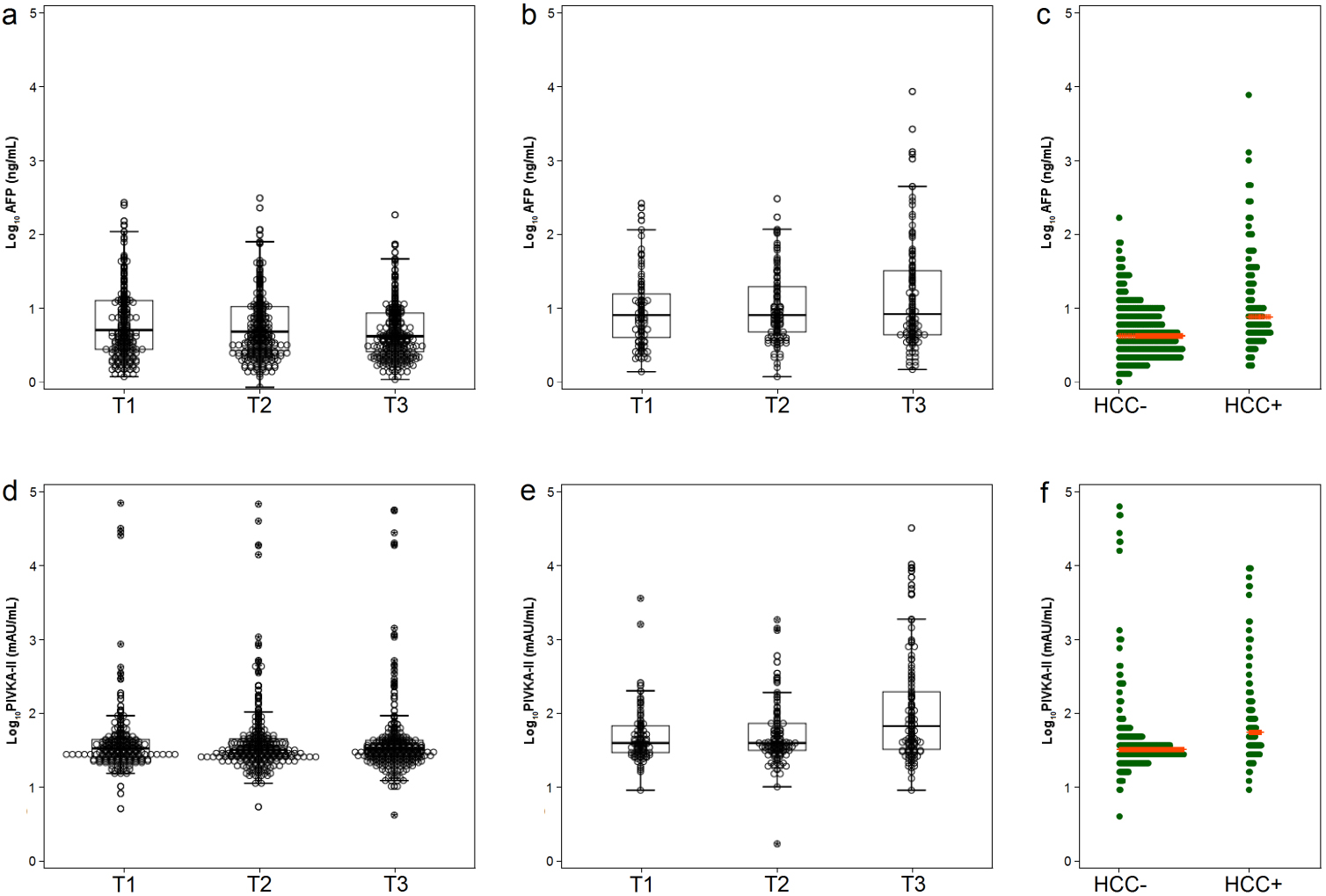
The distribution of the two biomarkers in HCC and HCC is given in Fig. 1. Overall, median values (25; 75 percentile) of AFP and PIVKA-II were 5.6 (3.1; 11.8) ng/mL and 34 (26; 51) mAU/mL, respectively.
Concentrations of biomarkers at different time-points in HCC (panel a and d) and HCC (panel b and e). Dotplot distribution of AFP (panel c) and PIVKA-II (panel f) in HCC and HCC. The red line is the median.
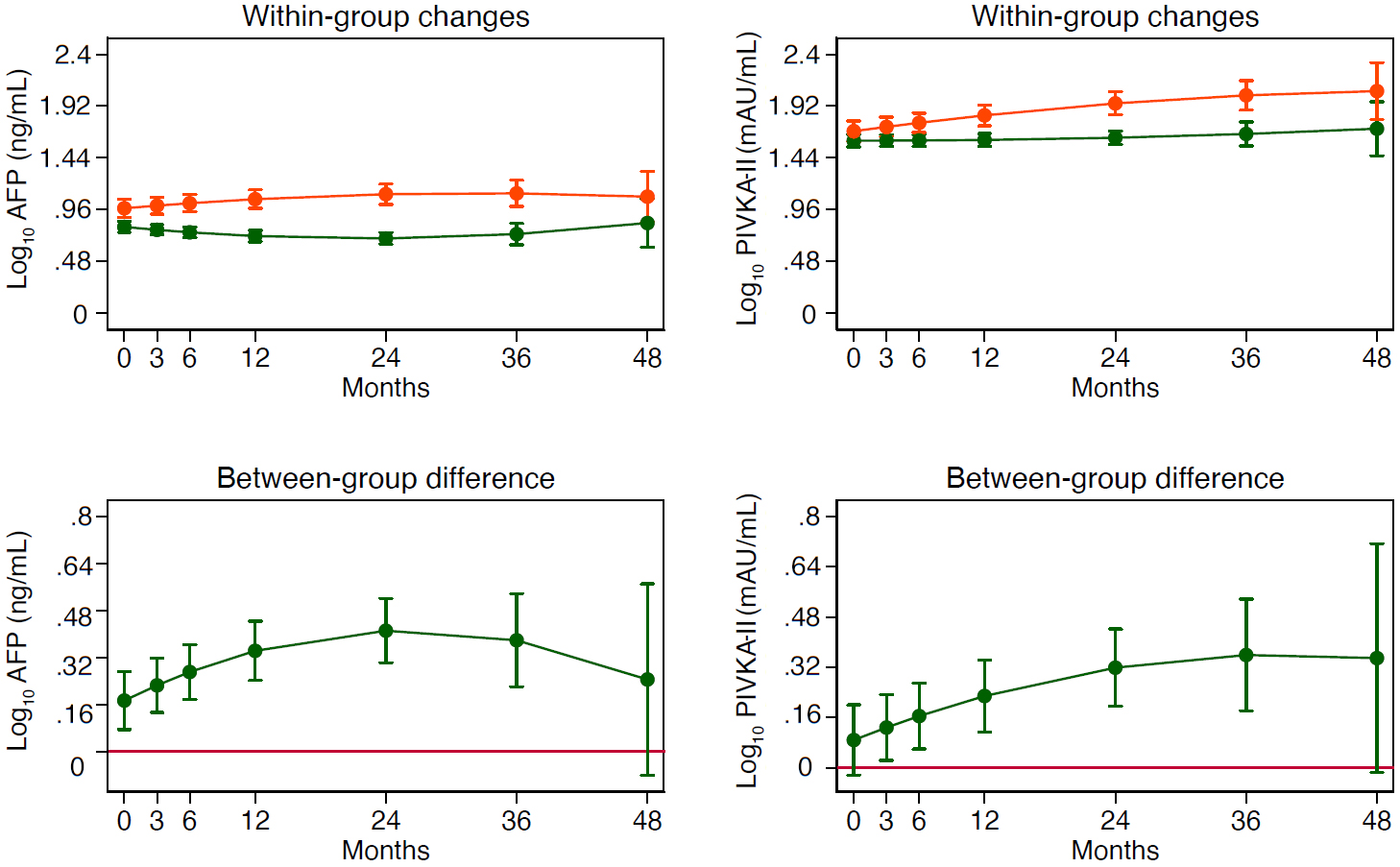
Changes in logAFP and logPIVKA-II as estimated by the RE-GLS model in HCC (red line) and HCC (green line). Values are means and 95% bootstrapped confidence intervals (see statistical analysis for details). Between-group differences are obtained by subtracting HCC minus HCC.
The time-related changes of logAFP and logPIVKA-II as estimated by the RE-GLS model are plotted in Fig. 2. Both logAFP and logPIVKA-II differ in HCCvs. HCC patients at all time-points except at 48 months where the precision of the model decreases due to a greater dispersion of data points. An identical pattern is obtained by modeling male and female data separately (not shown). The regression coefficients for the fixed part of the RE-GLS model used to investigate the changes of logAFP and logPIVKA-II in HCCvs. HCC patients are reported in Table 3.
Regression coefficients for the fixed part of the RE-GLS model used to investigate the changes of AFP and PIVKA-II in HCC and HCC
LogAFP
LogPIVKA-II
HCC
0.173 [0.074; 0.272]
0.088 [0.024; 0.200]
Month
0.010 [0.016; 0.004]
0.000 [0.007; 0.006]
HCC *Month
0.17 [0.05; 0.30]
0.18 [0.05; 0.31]
Month*Month
0.018 [0.008; 0.028]
0.014 [0.002; 0.025]
HCC *Month*Month
0.000 [0.000; 0.000]
0.000 [0.000; 0.000]
HCC *Month*Month
0.000 [0.001; 0.000]
0.000 [0.001; 0.000]
Intercept
0.799 [0.748; 0.850]
1.599 [1.542; 1.656]
95% bootstrapped confidence intervals in brackets. 0.05, 0.01, 0.001.
Ratios between the value of logAFP and logPIVKA-II at selected time-points (3, 6, 12, 24, 36 and 48 months) vs. the baseline as estimated from the RE-GLS model by means of non-linear contrasts in and HCC (panel a) and HCC (panel b) patients (see statistical analysis for details). Values higher or lower than 1 indicate increasing or decreasing trends respectively. Shaded areas are 95% CI confidence intervals.
Figure 3 shows the ratios between a given time-point (3, 6, 12, 24, 36 and 48 months) and the baseline of logAFP and logPIVKA-II in HCC and HCC patients as estimated from the RE-GLS model by means of non-linear contrasts. In HCC patients, logAFP and logPIVKA-II show different time-courses, with the latter being highly stable over time and showing lower 95% CIs compared to logAFP (panel a). In HCC patients, the ratios become increasingly greater than 1 with time (panel b). The precision of the estimate as conveyed by 95% CI is higher for PIVKA-II and greatly decreases for both markers after 24 months because of the lower number of available time-points.
To further characterize the variability of AFP and PIVKA-II, we computed the percent change estimated from the RE-GLS model using non-linear contrasts at a given time-point (3, 6, 12, 24, 36 and 48 months) versus the baseline value in HCC compared to HCC patients (Table 4). The analysis shows that the percentage variability of logAFP is higher than the variability of logPIVKA-II. The width of 95% CIs indicates that the accuracy of the estimate is higher for logPIVKA-II than logAFP.
Percent change vs. baseline at given time-points in HCC versus HCC patients
Time (months)
LogAFP (%)
LogPIVKA-II (%)
3
6 (3 to 9) 0.001
2 (0 to 4) 0.017
6
11 (5 to 17) 0.001
5 (1 to 8) 0.012
12
19 (10 to 29) 0.001
8 (3 to 14) 0.005
24
27 (15 to 38) 0.001
14 (6 to 21) 0.001
36
23 (6 to 39) 0.009
16 (5 to 26) 0.003
48
7 (29 to 42) 0.717
15 (6 to 36) 0.163
95% bootstrapped confidence intervals in brackets.
Discussion
The time-changes of any biomarker are the result of both the analytical and biological variability. When the analytical imprecision of the assay is sufficiently low, the biological variation retains a potential clinical value that needs to be addressed. In particular, when dealing with biomarkers for cancer surveillance, it would be crucial to discriminate the extent of variability that is the expression of non-malignant conditions from a variability that is likely to indicate an ongoing neoplastic process.
In the present case-control study, we aimed to estimate the time-changes of AFP and PIVKA-II in patients with and without HCC development. Interestingly, in HCC patients both AFP and PIVKA-II were estimated to increase over time, confirming their potential usefulness during periodic surveillance. On the other hand, among HCC patients the time-related changes of PIVKA-II were more stable than those of AFP. The different trajectories of PIVKA-II in HCC and HCC patients are likely to reflect the mechanism of PIVKA-II production, which, contrarily to AFP, is not affected by liver disease activity [21].
The design of the present retrospective study was not intended to quantify the extent of the clinically relevant variability for HCC diagnosis. We computed, however, the percent time-related changes of logAFP and logPIVKA-II in HCCvs. HCC patients using a RE-GLS regression model. At 6 months, i.e. the first reference time-point for US surveillance of patients at risk of HCC development, we found a 11% (95% CI 5 to 17%) increase of logAFP and a 5% (95% CI 1 to 8%) increase of logPIVKA-II compared to baseline in HCCvs. HCC patients. The 95% CIs of logPIVKA-II were narrower than those of logAFP (not only at 6 months but at any time-point). According to these data, any increase of serum PIVKA-II levels above 2 standard deviations of the analytical variability of the assay is likely to be clinically relevant for the diagnosis of HCC while AFP changes are expected to be much more variable.
These findings are consistent with the notion that disease activity affects the diagnostic performance of AFP more than that of PIVKA-II [22]. Accordingly, disease activity was highly variable in our population; ninety percent of our patients with HBV-related CLD were in fact undergoing antiviral treatment with nucleos(t)ide analogues and had a suppressed viremia and normal liver enzymes. On the contrary, only 31% of our patients with HCV-related CLD were undergoing antiviral treatment and 43% of them had normal liver enzymes. Since a prolonged remission of disease limits the confounding effect of necro-inflammation on AFP serum levels, future analyses are needed to reconsider AFP diagnostic performance in patients with sustained virologic response.
The present study has several limitations. The major limitation is the fact that the time-points which were used to model the time-course of AFP and PIVKA-II were not equally spaced. To account for this fact, we used a RE-GLS with a pre-specified shape for time and the time*HCC interaction and a random effect at the patient-level (see statistical analysis for details). Although this is acceptable on theoretical grounds, it would be much better to analyze equally spaced time-points (e.g. 6, 12 and 24 months) because a program of HCC surveillance is usually based on such fixed time frame. Another limitation is the aforementioned heterogeneity of the study patients, who had liver cirrhosis of different etiology and different disease activity. On the other hand, such population is ideal for performing a general proof-of-concept study of the variability of HCC markers, as we did here, because it offers a different case-mix of patients. Another limitation is that HCC frequency differed substantially among the three study centers, being 46.5% in Pisa, 14.2% in Naples and 14.3% in Padua. There was certainly a selection bias due to the inclusion criterion specifying that at least two repeated sera per patient were needed for inclusion into the present analysis. However, bootstrapping the RE-GLS model with replacement within each center did not change our findings (data not shown).
In conclusion, we found that time-changes of PIVKA-II and AFP have the potential for being employed as early markers of HCC. The evidence provided by this proof-of-concept study suggests performing prospective studies of the time-course of AFP and PIVKA-II to identify their specific time-related variations to be used as early marker of HCC.
References
1.
BoschF.X. et al., Primary liver cancer worldwide incidence and trends, Gastroenterology127(5 Suppl 1) (2004), S5–S16.
2.
El-SeragH.B., Epidemiology of viral hepatitis and hepatocellular carcinoma, Gastroenterology142(6) (2012), 1264–1273.
3.
El-SeragH.B., Surveillance for hepatocellular carcinoma: in whom and how? Therap Adv Gastroenterol4(1) (2011), 5–10.
4.
HeimbachJ.K. et al., AASLD guidelines for the treatment of hepatocellular carcinoma, Hepatology67(1) (2018), 358–380.
5.
SingalA. et al., Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis, Aliment Pharmacol Ther30 (2009), 30–47.
6.
European Association for the Study of Liver, EASL clinical practice guidelines: management of hepatocellular carcinoma, J Hepatol69(1) (2018), 182–236.
7.
KudoM. et al., JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the liver cancer study group of japan, Liver Cancer3(3–4) (2014), 458–468.
8.
LokA.S. et al., Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma, Gastroenterology138 (2010), 493–502.
9.
LiC. et al., Diagnostic accuracy of des-gamma-carboxy prothrombin versus alpha-fetoprotein for hepatocellular carcinoma: a systematic review, Hepatol Res44(10) (2014), 11–25.
10.
JangE.S. et al., Diagnostic performance of alpha-fetoprotein, protein induced by vitamin K absence, osteopontin, dickkopf-1 and its combinations for hepatocellular carcinoma, PLoS One11(3) (2016), e0151069.
11.
LimT.S. et al., Combined use of AFP, PIVKA-II, and AFP-L3 as tumor markers enhances diagnostic accuracy for hepatocellular carcinoma in cirrhotic patients, Scand J Gastroenterol51(3) (2016), 344–353.
12.
HuoT.I. et al., The predictive ability of serum alpha-fetoprotein for hepatocellular carcinoma is linked with the characteristics of the target population at surveillance, Journal of Surgical Oncology95 (2007), 645–651.
13.
RiccoG. et al., Impact of etiology of chronic liver disease on hepatocellular carcinoma biomarkers, Cancer Biomark21(3) (2018), 603–612.
14.
GopalP. et al., Factors that affect accuracy of a-fetoprotein test in detection of hepatocellular carcinoma in patients with cirrhosis, Clin Gastroenterol Hepatol12(5) (2014), 870–877.
15.
LiebmanH.A. et al., Des-gamma-carboxy (abnormal) prothrombin as a serum marker of primary hepatocellular carcinoma, N Engl J Med310 (1984), 1427–1431.
16.
XingH. et al., Clinical application of protein induced by vitamin K antagonist-II as a biomarker in hepatocellular carcinoma, Tumour Biol37 (2016), 15447–15456.
17.
JohnsonP.J. et al., The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers, Cancer Epidemiol Biomarkers Prev23(1) (2014), 144–153.
18.
HemkenP.M. et al., Validation of a novel model for the early detection of hepatocellular carcinoma, Clin Proteomics16(2) (2019), 1–9.
19.
ChoiJ. et al., Evaluation of automated serum des-gammacarboxyprothrombin (DCP) assays for detecting hepatocellular carcinoma, Clin Biochem44(17–18) (2011), 1464–1468.
20.
HarrellF.E., Regression modeling strategies: with applications to linear models, logistic and ordinal regression, and survival analysis. Springer, Switzerland, 2015.
21.
MurataK. et al., Cytoskeletal changes during epithelial-to-fibroblastoid conversion as a crucial mechanism of des-gamma-carboxy prothrombin production in hepatocellular carcinoma, Int J Oncol35(5) (2009), 1005–1014.
22.
KimG.A. et al., Reappraisal of serum alpha-foetoprotein as a surveillance test for hepatocellular carcinoma during entecavir treatment, Liver Int35(1) (2015), 232–239.