
Abstract
Background:
Several studies have been conducted to evaluate the prognostic value of prothrombin induced by vitamin K absence-II (PIVKA-II) overexpression in hepatocellular carcinoma patients treated with curative ablation. However, the results remain controversial. The purpose of this meta-analysis was to explore the correlation between PIVKA-II expression and survival outcomes in these patients.
Methods:
We performed a systematic literature search in PubMed, EMBASE, Medline, Cochrane Library, and Web of Science to identify the relevant articles investigating the prognostic value of PIVKA-II in patients with hepatocellular carcinoma. Combined hazard ratios (HR) and their 95% confidence intervals (CI) for overall survival and recurrence-free survival were calculated as the analysis endpoints.
Results:
A total of 15 cohorts encompassing 5647 patients were included. The results indicated that elevated PIVKA-II was significantly associated with poorer overall survival (HR 1.59; 95% CI 1.40, 1.82; P < 0.001) and recurrence-free survival (HR 1.76; 95% CI 1.42, 2.17; P < 0.001). Similar results were observed in the subgroup analysis based on sample size, analytical method, treatment modality, and cut-off value.
Conclusions:
This meta-analysis suggests that elevated PIVKA-II is a predictor of unfavorable overall survival and recurrence-free survival in hepatocellular carcinoma patients receiving curative ablation. More rigorous studies are warranted to confirm the clinical utility of PIVKA-II in determining hepatocellular carcinoma prognosis.
Introduction
Hepatocellular carcinoma (HCC) is one of the most predominant and aggressive malignancies in the world. This type of carcinoma is the fifth most common cause of cancer-related death in males and the eighth in females. 1 During the last few decades, periodic surveillance in high-risk people has not only enabled the diagnosis of HCC at an early stage but also promoted the application of curative treatments, such as hepatic resection and percutaneous ablation. 2 Although hepatic resection is usually the first treatment option to consider, the application is still limited in the majority of patients owing to impaired liver function. 3 Recently, percutaneous ablation, including thermal ablation and percutaneous ethanol injection, has gained increasing popularity as a safe, less invasive, and easily repeated treatment modality in small HCC. These ablative therapies can be utilized in patients who are ineligible for hepatic resection and have shown favorable survival rates with excellent curability. 4
Despite the rapid progression in treatment modalities and early diagnostic techniques, the long-term outcome of HCC after ablation remains disappointing. Although serum alpha-fetoprotein (AFP) has been considered an important surveillance marker of HCC for several decades, its prognostic capability is not satisfactory. 4 It can be elevated in patients with chronic hepatitis or liver cirrhosis in the absence of cancer. 5 The expression of AFP is also found to have no prognostic effect in patients with single, small HCC receiving curative therapy. 6 Hence, the investigation of more efficient predictive makers for HCC is of great clinical importance.
Prothrombin, containing 10 γ-carboxyglutamic acid (Gla) residues in the amino-terminal domain, is synthesized in the liver. 7 Prothrombin is a vitamin K-dependent plasma coagulation factor. Vitamin K deficiency or ingestion of vitamin K antagonists can inhibit the activity of vitamin K-dependent carboxylase, leading to an acquired defect of post-translational carboxylation of the glutamic acid (Glu) residues on the prothrombin precursor. As a result, abnormal prothrombin (PIVKA-II), without γ-carboxylation of all its Glu residues, is released into the plasma. The correlation between PIVKA-II levels and HCC was first reported by Liebman et al. 8 in 1984. Since then, accumulating evidence has revealed that PIVKA-II may be a useful diagnostic and prognostic tumor marker for HCC.9-12
Unfortunately, the prognostic value of PIVKA-II in HCC patients treated with ablation is controversial and has not yet been methodically analyzed. Some studies concluded that high expression of PIVKA-II was associated with worse prognosis in patients with HCC,13-16 while others did not show any significant correlation between PIVKA-II and clinical outcomes.17-20 We therefore performed this meta-analysis to elucidate the prognostic value of increased PIVKA-II on overall survival (OS) and recurrence-free survival (RFS) in HCC patients receiving curative ablation by pooling outcomes from obtainable data.
Materials and methods
This systematic review and meta-analysis was performed strictly in accordance with PRISMA guidelines. Before the initiation of the review process, we registered a review protocol at PROSPERO.org with registration number CRD42017063996.
Search strategy
A comprehensive search of PubMed, EMBASE, Medline, Cochrane Library, and Web of Science databases was performed in March 2017 using the following terms: “hepatocellular carcinoma” or “liver cancer” or “hepatoma” or “HCC”; and “prognosis” or “prognostic” or “survival” or “recurrence”; and “decarboxyprothrombin” or “des-gamma-carboxy prothrombin” or “des-γ-carboxy prothrombin” or “DCP” or “PIVKA-II”; and ablation. The citations reported in selected studies were then carefully screened to seek potential eligible publications.
Inclusion and exclusion criteria
The included studies fulfilled the following criteria: (a) the study evaluated the prognostic role of PIVKA-II in HCC patients undergoing percutaneous ablation therapy; (b) PIVKA-II was detected using serum-based methods before treatment; (c) the study provided sufficient data of hazard ratios (HRs) and 95% confidence intervals (CIs) for OS and RFS; and (d) the study was published as a full paper in English. When multiple studies reported by the same institution or authors were identified, the most recent or most complete study was chosen. Conference records, case reports, reviews, letters, and non-English language studies were excluded. Two reviewers (Zhang and Liu) selected the studies in duplicate according to the criteria mentioned above. Inconsistencies were resolved by discussion or re-evaluation with the third author.
Data extraction and quality assessment
Data were extracted by two investigators independently. The details of each article were recorded as follows: first name of the author, publication year, sample size, median/mean age, cut-off value, PIVKA-II overexpression, outcome measures, analytical method, treatment modality, HR, and associated 95% CI. When the study provided both multivariable and univariate analysis for HR, only the result of multivariable analysis was selected.
The Newcastle-Ottawa Scale (NOS) is a quality assessment scale that was adopted to evaluate the quality of all primary studies. The scale consists of eight questions that focus on the assessment of cohort selection, study comparability, and outcome assessment. NOS scores ranged from zero to nine, and studies with scores above six were considered to have a high methodological quality.
Statistical analysis
Stata Version 14.0 (StataCorp, College Station, TX, USA) was utilized to carry out the statistical analyses. HRs with corresponding 95% CIs were aggregated to measure the prognostic significance of PIVKA-II in HCC patients. In the case that a study did not provide exploitable information, the statistics were extracted indirectly from available numerical data or Kaplan–Meier curves according to the methods suggested by Tierney et al. 21 A pooled HR value greater than one was indicative of a worse outcome for patients with high PIVKA-II levels. The heterogeneity across studies was evaluated by Higgins I2 statistic and Cochran’s Q test. A P value < 0.05 and/or I2 > 50% denoted studies of substantial heterogeneity. In that case, the random-effect model was employed to assess the pooled HRs; otherwise, the fixed-effect model was applied. Publication bias was evaluated using the funnel plot and Egger’s test. In order to estimate the reliability of the prognostic outcomes, we also performed the sensitivity analysis. All statistical tests with P < 0.05 were considered to indicate statistically significant.
Results
Study characteristics
The selection process of the included studies is shown in Figure 1. A total of 202 records were identified through the literature search. Among these records, 98 duplicate articles were removed. We then excluded 73 articles by scanning the title and abstract. Ultimately, 14 eligible studies (15 cohorts) containing 5674 participants were included in the data analyses after a full-text review. The study by Minami et al. 22 evaluated the prognostic role in two different cohorts and reported the HR and 95% CI separately.
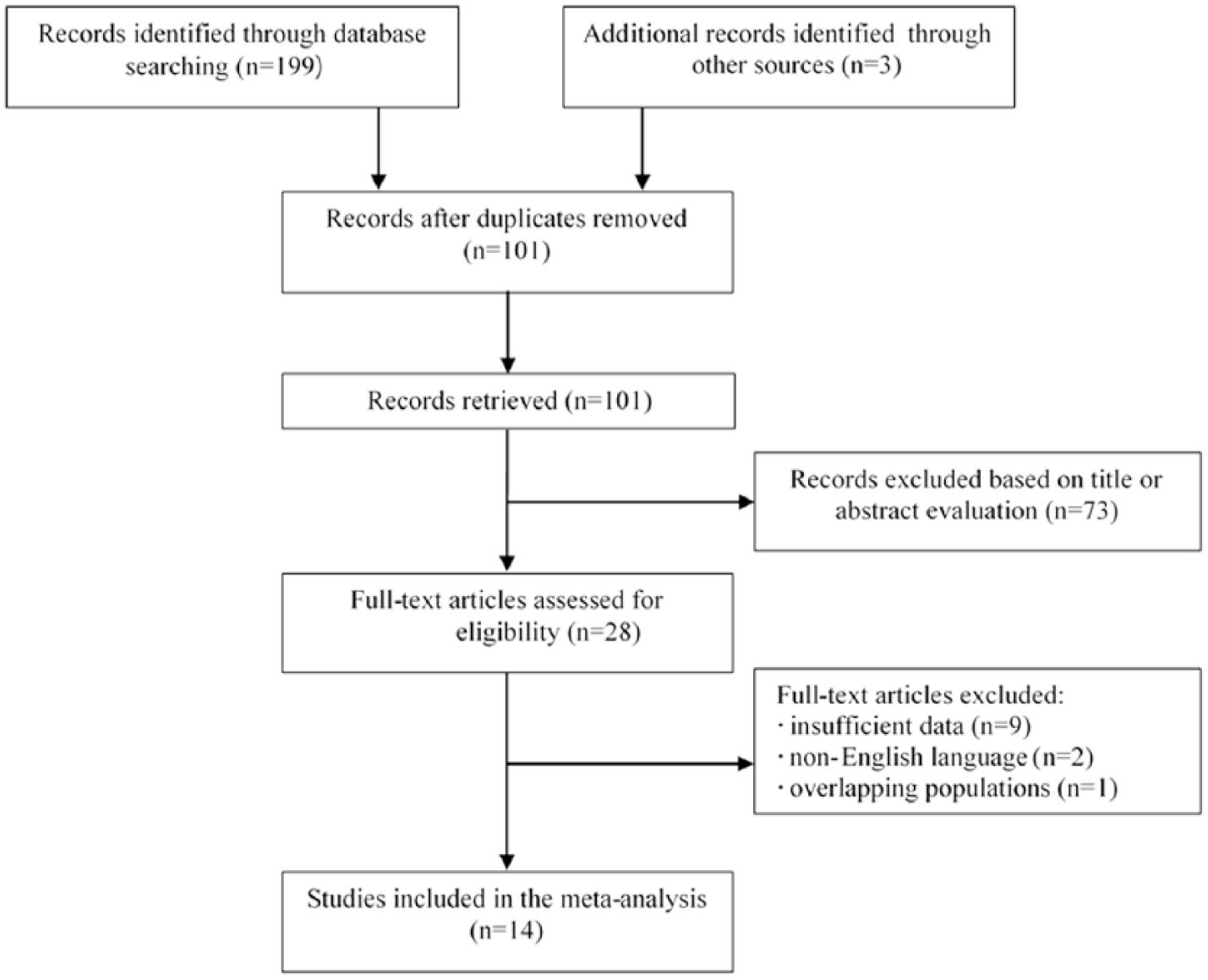
Flowchart of the study selection process.
The major characteristics of each study are presented in Table 1. The quality of the eligible studies was assessed by NOS scores, which ranged from six to eight for these studies. All eligible cohorts were conducted in Asian countries, including 1413-20,22-26 in Japan and one 27 in Korea. The sample size varied from 99 to 1219, and the mean (median) age of the study patients varied from 57 to 73 years old. Of the 15 cohorts, nine13,15,16,18-20,25-27 reported radiofrequency ablation (RFA) as the therapeutic intervention for HCC, whereas patients in the remaining six cohorts14,17,22-24 were treated with local ablation therapy (LAT), including percutaneous microwave coagulation therapy, percutaneous ethanol injection, and radiofrequency ablation. Nine cohorts13-17,22,26,27 focused on the prognostic role of PIVKA-II for OS, and 1114-16,18-20,23-27 for RFS. All the enrolled patients in two cohorts had hepatitis B virus (HBV)-related hepatocellular carcinoma. Among the 15 involved cohorts, 14 of them were retrospective in design, with only one 24 based on a prospective cohort. The cut-off values were determined by the investigators and were different in these studies.
Baseline characteristics of the included studies.
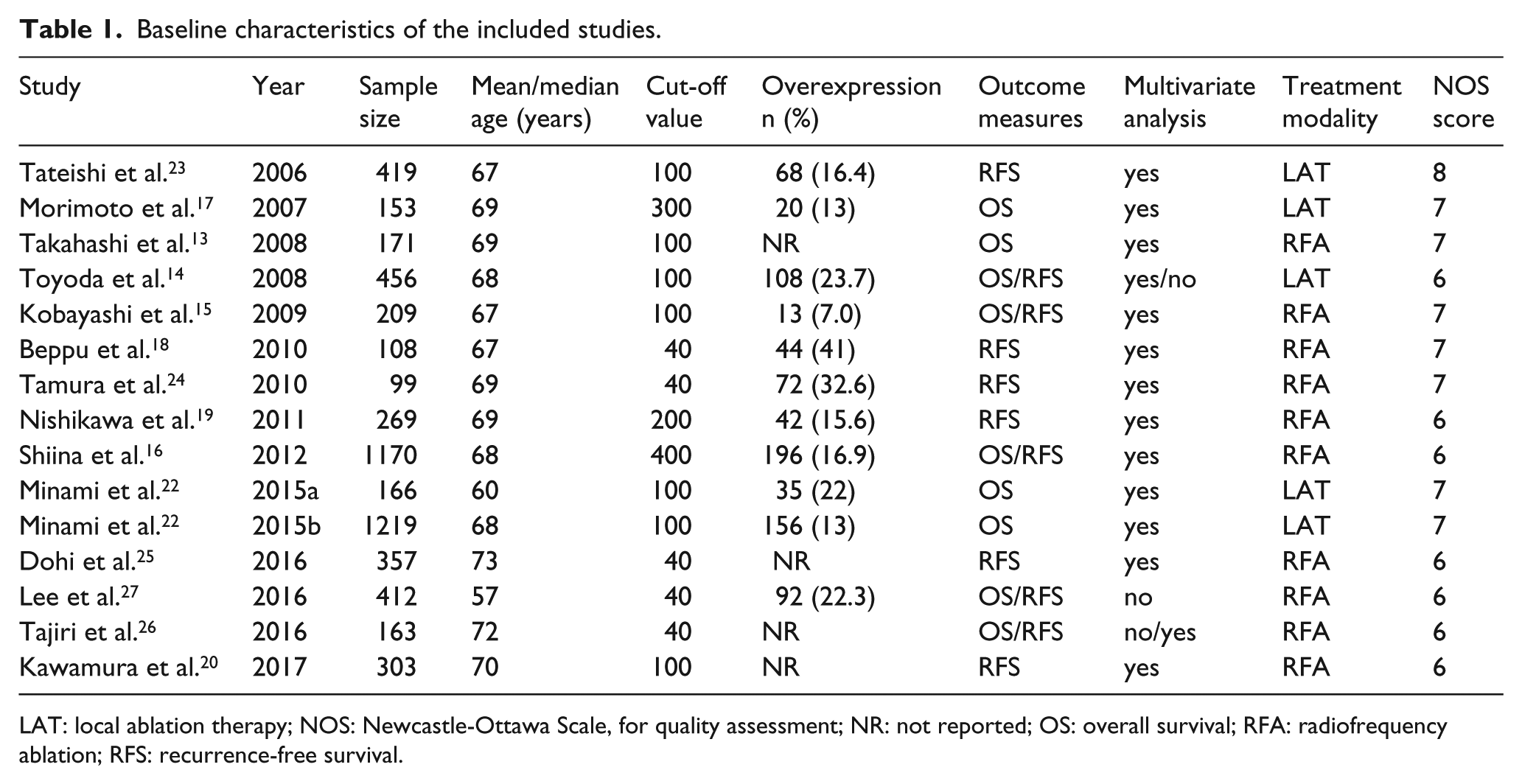
LAT: local ablation therapy; NOS: Newcastle-Ottawa Scale, for quality assessment; NR: not reported; OS: overall survival; RFA: radiofrequency ablation; RFS: recurrence-free survival.
PIVKA-II and OS in HCC
Nine cohorts involving 4149 patients provided sufficient data for OS analysis. As shown in Figure 2, the fixed-effect model was utilized to verify the relationship between PIVKA-II and OS. The combined data demonstrated that elevated PIVKA-II obviously correlated with a worse OS (HR 1.59; 95% CI 1.40, 1.82; P < 0.001; I2 = 47.9%, P = 0.052) when compared to a low PIVKA-II.
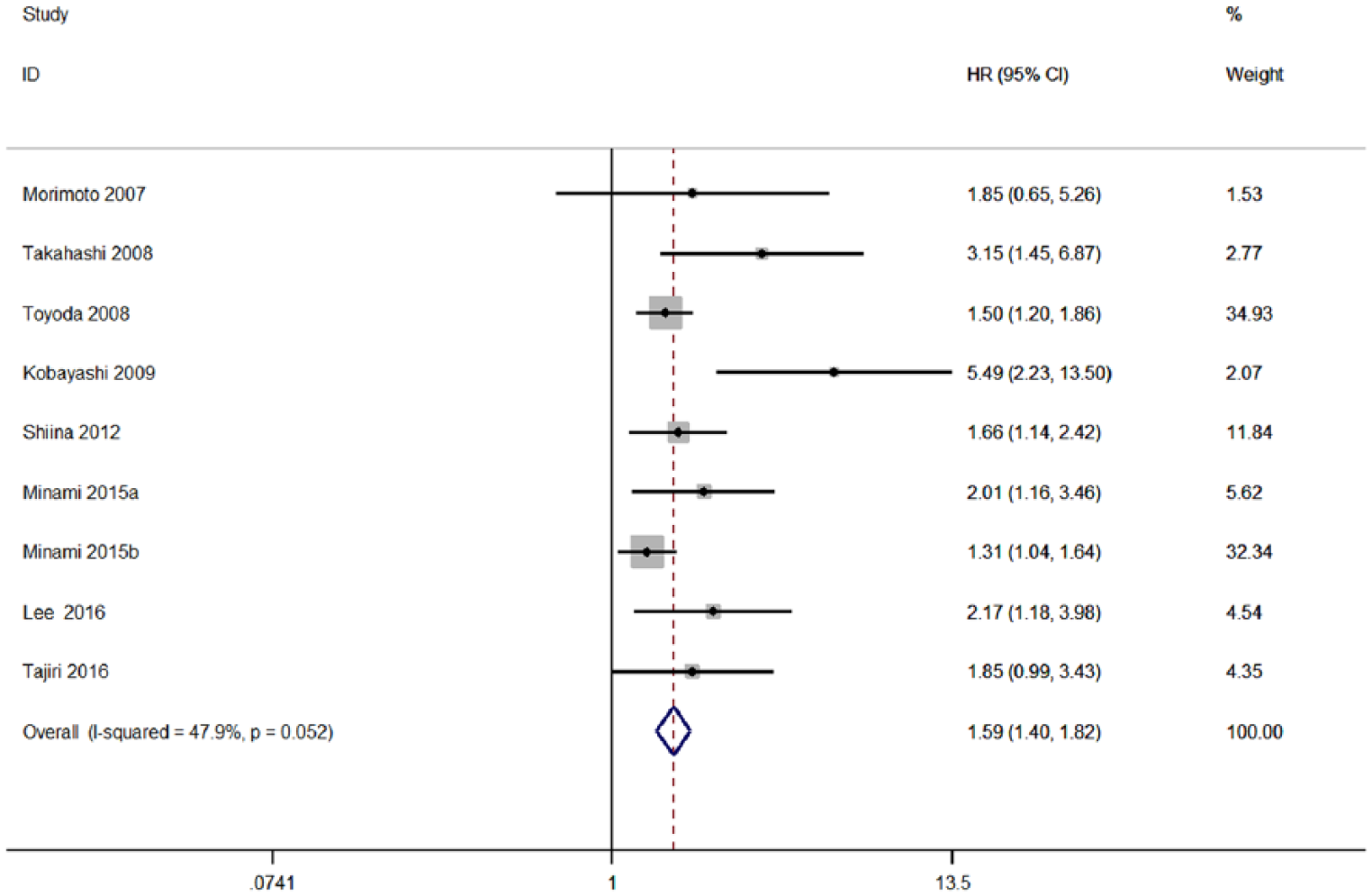
Forest plot of studies evaluating the association between high PIVKA-II levels and OS in HCC patients.
Subgroup analysis was conducted to further investigate the potential source responsible for the heterogeneity. As shown in Table 2, a significant relationship between high PIVKA-II and poor OS was detected in HCC both when sample size < 400 (HR 2.39; 95% CI 1.74, 3.29) and sample size ≧ 400 (HR 1.47; 95% CI 1.28, 1.70). In terms of treatment modality, the results indicated that PIVKA-II was an unfavorable predictor of prognostic in HCC patients initially treated by RFA with an HR of 1.59 (95% CI 1.40, 1.82) and LAT with an HR of 1.45 (95% CI 1.25, 1.69). Similar results were observed in the stratified analysis by cut-off value and treatment modality. The summary HRs for OS were significantly different when grouped according to the sample size (PD = 0.007) and treatment modality (PD = 0.016). In contrast, differences across subgroups of analytical method (PD = 0.151) and cut-off value (PD = 0.277) were not statistically significant.
Summary of the subgroup analyses.
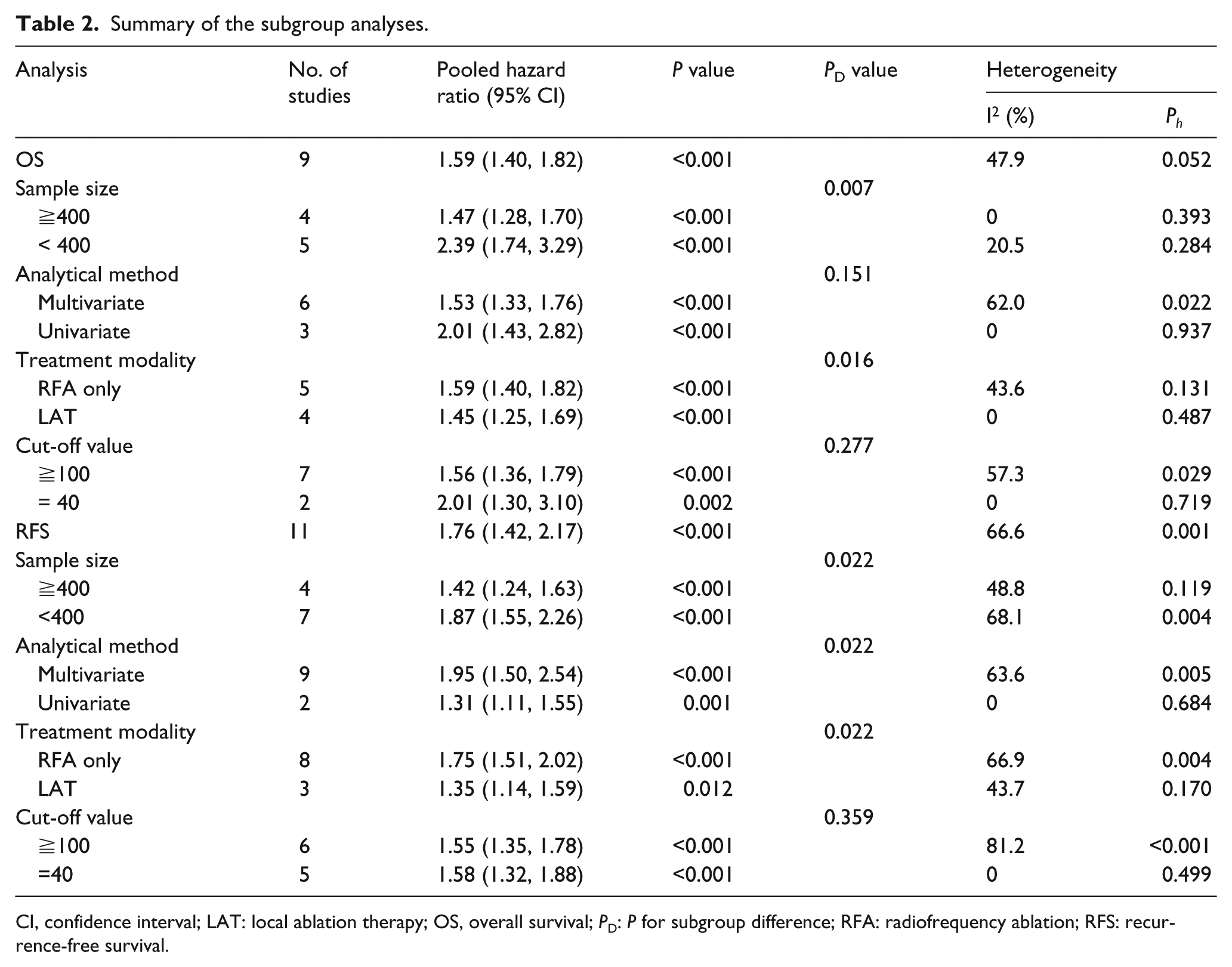
CI, confidence interval; LAT: local ablation therapy; OS, overall survival; PD: P for subgroup difference; RFA: radiofrequency ablation; RFS: recurrence-free survival.
PIVKA-II and RFS in HCC
Eleven cohorts were included to investigate the relationship between PIVKA-II and RFS in patients with HCC. Considering the significant heterogeneity (I2 = 66.6%; P = 0.001; Figure 3) between studies, we employed the random-effect model to pool the HR. Pooled data showed that patients with high PIVKA-II exhibited shortened RFS with a combined HR of 1.76 (95% CI 1.42, 2.17; P < 0.001). Subgroup analysis based on the number of patients indicated that studies with large sample size (HR 1.42; 95% CI 1.24, 1.63; P < 0.001) were correlated with a smaller effect when compared with small sample size (HR 1.87; 95% CI 1.55, 2.26; P < 0.001). In the analysis according to the analytical method, studies assessed by univariate analysis (HR 1.31; 95% CI 1.11, 1.55; P = 0.001) and multivariate analysis (HR 1.95; 95% CI 1.50, 2.54; P < 0.001) gave identical results. Significant HR was found in both RFA group (HR 1.75; 95% CI 1.51, 2.02; P < 0.001) and LAT group (HR 1.35; 95% CI 1.14-1.59; P = 0.012). Similarly, the results did not change in the subgroup analysis of cut-off value (≧100: HR 1.55; 95% CI 1.35, 1.78; P < 0.001; and = 40: HR 1.58; 95% CI 1.32, 1.88; P < 0.001).
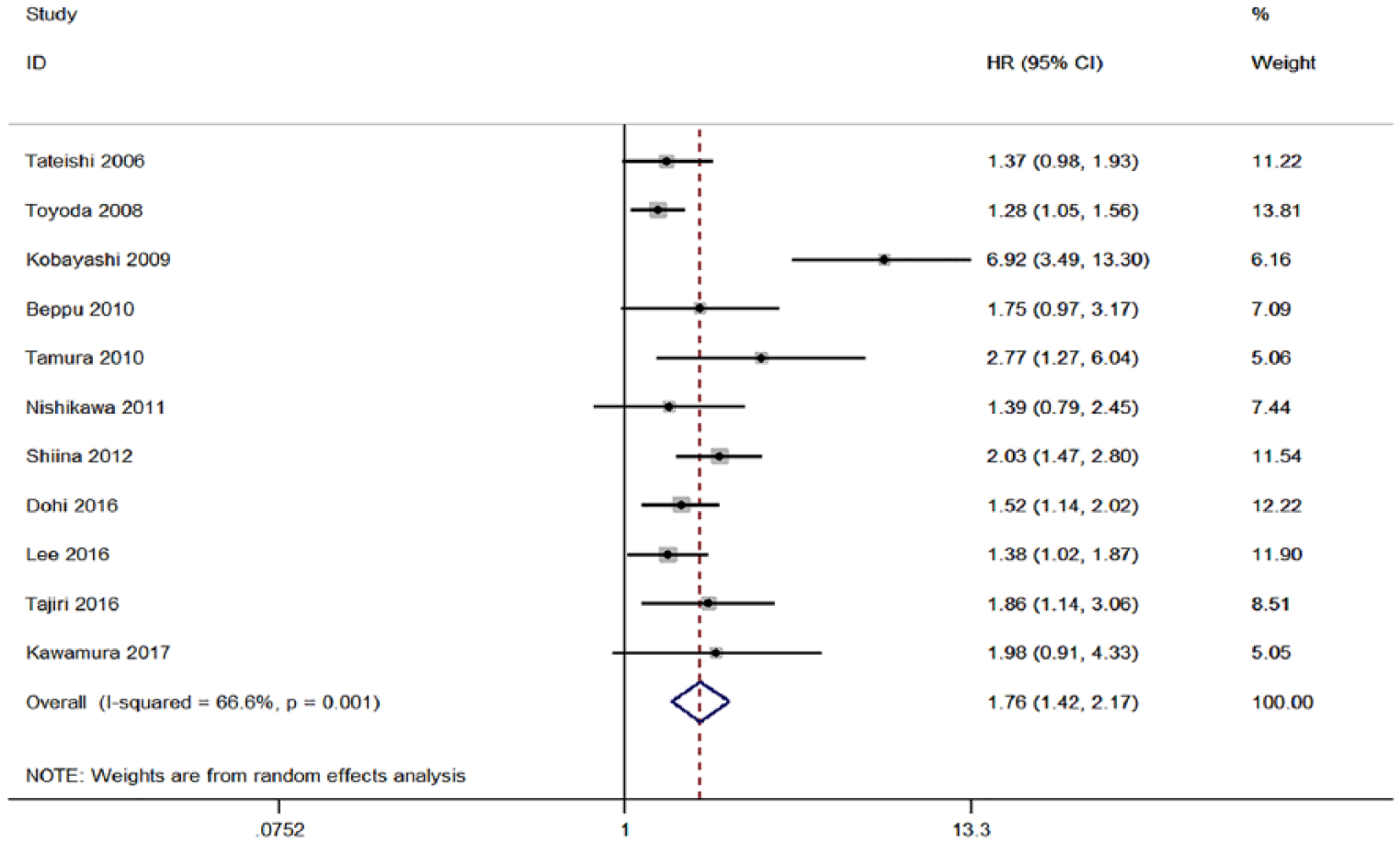
Forest plot of studies evaluating the association between high PIVKA-II levels and RFS in HCC patients.
Sensitivity analysis
Sensitivity analysis showed that the combined outcomes were not materially changed by eliminating any single study, indicating the robustness of our meta-analysis (Supplementary Figure1). It is important to note that the heterogeneity between the remaining studies was strikingly decreased when the study by Kobayashi et al. 15 was omitted (I2 = 12.2%; P = 0.335 for OS; and I2 = 13.1%; P = 0.323 for RFS), which meant this study might contribute to the heterogeneity in both OS and RFS analyses. Removing this over-weighted study, the elevated PIVKA-II levels still had a significant impact on the prognostic outcomes (HR 1.55; 95% CI 1.36, 1.77 for OS; and HR 1.50; 95% CI 1.34, 1.67 for RFS).
Publication bias
Visual inspection of the funnel plots exhibited asymmetry for both OS and RFS. Consistently, the P value of Egger’s test also implied the presence of publication bias among the included studies (P = 0.005 in OS and P=0.026 in RFS). We therefore conducted a trim-and-fill analysis to adjust the publication bias. The results indicated that the pooled analysis incorporating the unpublished studies did not alter the significant prognostic impact of elevated PIVKA-II, and the adjusted HR would be 1.46 (95% CI 1.30,1.65; P<0.001) for OS and 1.44 (95% CI 1.14, 1.83; P=0.003) for RFS.
Discussion
Recent advances in therapeutic interventions and imaging techniques have dramatically improved the survival outcomes of HCC patients. RFA, which has yielded comparable survival outcomes compared with surgical resection, is recommended in most instances as the main ablative therapy. Additionally, RFA was suggested to be the most cost-effective therapeutic strategy for early HCC. 28 However, recurrence and distant metastasis after ablation are still frequently encountered, which highlights the need for exploring a more efficient prognostic biomarker for patients with HCC.
PIVKA-II, also known as des-gamma-carboxy prothrombin (DCP), is an abnormal prothrombin lacking coagulant activities. PIVKA-II is a well-recognized biomarker in the diagnosis of HCC, and it has been suggested as a prognostic indicator for survival and recurrence after curative treatment.29,30 Nevertheless, the exact role of elevated PIVKA-II in HCC patients receiving percutaneous ablation remains obscure.
To the best of our knowledge, the present meta-analysis is the first one to comprehensively explore the prognostic significance of elevated PIVKA-II in HCC patients. In this meta-analysis, we included 15 cohorts encompassing 5647 patients to evaluate the usefulness of PIVKA-II in predicting the survival outcomes for HCC patients after curative ablation. It was demonstrated that the excessive production of PIVKA-II was significantly correlated with shortened OS and RFS in HCC patients. We also investigated the influence of sample size, analytical method, treatment modality, and cut-off value on the pooled outcomes by subgroup analysis. As a result, no substantial alteration was observed, suggesting that PIVKA-II is a promising predictive marker to assist clinicians in making optimal decisions regarding treatment and outcomes. Adjuvant chemotherapy and careful follow-up after curative ablation should be necessary for patients with a high PIVKA-II level.
Statistical heterogeneity was detected in this meta-analysis. It is most likely due to the study by Kobayashi et al. 15 in which the high levels of PIVKA-II played a more superior prognostic role in HCC patients. The sensitivity analysis showed that after removing this outlier study, the heterogeneity in the remaining publications was strikingly decreased. The most plausible explanation for this could be related to the sample size. As we all know, studies with a smaller sample size are more prone to obtain a higher effect value. It was found that the number of patients with elevated PIVKA-II in the Kobayashi et al. 15 study was much smaller compared with those in the other studies, which may lead to an overestimation of the prognostic value of PIVKA-II. Furthermore, the conclusion of our meta-analysis was not altered after the sensitivity analysis, which further confirmed the reliability of the results.
Many researchers noted that PIVKA-II appeared to be a better diagnostic marker in comparison with AFP for HCC patients.7,9,29,31 This finding is compatible with the results of a meta-analysis conducted by Li et al. 32 That meta-analysis included 49 studies and demonstrated that PIVKA-II showed more diagnostic accuracy than AFP, especially in diagnosing early-stage HCC. In our meta-analysis, we also attempted to compare the prognostic value of PIVKA-II with AFP in HCC patients treated with curative ablation. Among the 15 included cohorts, eight provided sufficient information to investigate the predictive ability of AFP, which indicated that pretreatment AFP values may have a worse prognostic effect than PIVKA-II in HCC patients. In addition, five of the included cohorts suggested that no difference was found in clinical outcomes between patients with and without elevated serum AFP, but they only offered the relevant P values. More effort should be made to validate whether PIVKA-II has more superior diagnostic and prognostic effect than AFP in HCC patients.
It is important to note that PIVKA-II does not always directly reflect the development of HCC. Serum PIVKA-II levels can be aberrantly elevated in patients with prolonged obstructive jaundice, vitamin K deficiency, or those taking vitamin K antagonists (e.g. warfarin) even in the absence of HCC. Hence, the prognostic value of PIVKA-II would be significantly diminished in these subpopulations. In order to improve the clinical utility of PIVKA-II, a novel PIVKA-II assay (NX-PVKA) measured by P-11 and P-16 antibodies has been developed. 33 It was reported that NX-PVKA could identify the elevation of PIVKA-II owing to HCC in patients taking anticoagulants. 34 Further studies are necessary to clarify the prognostic effect of NX-PVKA.
Although our meta-analysis revealed that the overexpression of PIVKA-II was an efficient prognostic marker for HCC, the exact mechanism of its correlation with survival outcomes has not been well understood. PIVKA-II is a novel type of vascular endothelial growth factor (VEGF) possessing potent mitogenic and migrative activities. 35 As reported in previous studies, PIVKA-II was identified to stimulate the proliferation of HCC cells through activating the Met-JAK1-STAT3 signaling pathway. 36 Fujikawa et al. 37 found that PIVKA-II induced both DNA synthesis and cell migration in human umbilical vein endothelial cells, and the biological effect was brought out by directly binding to the kinase insert domain receptor. Moreover, several studies showed that PIVKA-II significantly stimulated the expression of angiogenic factors in HCC cells, such as VEGF, epidermal growth factor receptor, and matrix metalloproteinase.38,39
Several limitations should be acknowledged in the present meta-analysis. First, most of the included studies were based on retrospective cohorts, and subject selection bias is unavoidable in these articles. Second, all the eligible studies were conducted in Asia, in which the demography and liver disease etiology for HCC are substantially different from those in Western societies. It is worth noting that in a study conducted in France, the investigators suggested that PIVKA-II could be used for prognostic assessment because increased PIVKA-II was strongly correlated with the presence of microvascular invasion. 12 However, more studies should be performed to shed light on the prognostic role of PIVKA-II in various geographic populations. Third, the association between elevated PIVKA-II and the clinicopathological parameters was not estimated, and the impact of these factors on the prognostic value of PIVKA-II failed to be illuminated due to the limited data. Furthermore, the cut-off values used in the included studies were not unified, which might influence the reliability of our results. Despite this, the prognostic significance of PIVKA-II was not affected by different cut-off values according to the subgroup analysis. Finally, the publication bias was a concern, although we tried to recognize all relevant data. Nonetheless, the trim-and-fill analysis showed that the pooled effect size was still significant even if the negative results were published.
In conclusion, it is indicated that the overexpression of PIVKA-II in pretreatment samples is correlated with a poor prognosis in HCC patients that receive curative ablation. This finding may be helpful in determining optimal treatment therapeutics for HCC patients. Considering the limitation of our analysis, further well-designed, large-scale, and multicenter prospective studies are warranted to validate the prognostic power of PIVKA-II.
Supplemental Material
Supplementary – Supplemental material for Prognostic value of PIVKA-II in hepatocellular carcinoma patients receiving curative ablation: A systematic review and meta-analysis
Supplemental material, Supplementary for Prognostic value of PIVKA-II in hepatocellular carcinoma patients receiving curative ablation: A systematic review and meta-analysis by Dongjing Zhang, Zhihong Liu, Xueru Yin, Xiaolong Qi, Bingyun Lu, Yuanyuan Liu and Jinlin Hou in The International Journal of Biological Markers
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.