
Abstract
BACKGROUND:
It is reported that prothrombin induced by vitamin K absence-II (PIVKA-II) has a better performance of diagnosis for HCC, and has also been known to be an independent risk factor for vascular invasion. Few studies study the relationship between PIVKA-II and HBV DNA.
OBJECTIVE:
To determine the clinical value of serum Prothrombin induced by vitamin K absence-II (PIVKA-II) in early hepatocellular carcinoma (HCC), and to explore its relationship with vascular invasion and HBV DNA.
METHODS:
In a Chinese cohort, we conducted a case-control study to compare the performances of a-fetoprotein (AFP) and PIVKA-II serum levels for diagnosis of HCC and early HCC. Fifty one healthy controls, 37 chronic hepatitis patients, 43 cirrhotic patients and 143 HCC cases of which 48 (33.57%) had early stage HCC (
RESULTS:
The serum levels of both PIVKA-II and AFP in HCC group were higher than that in chronic hepatitis, cirrhosis and healthy control groups. The sensitivity, specificity, positive predictive value, negative predictive value and kappa of PIVKA-II were higher than AFP in the diagnosis of HCC. Serum PIVKA-II level was correlated with tumor size, tumor cell differentiation and BCLC staging (
CONCLUSIONS:
PIVKA-II was more efficient than AFP for the diagnosis of early HCC and has no correlation with serum HBV DNA levels.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is currently the fourth most common malignant cancer and the third most common cause of cancer related death worldwide [1, 2]. Approximately 75% of liver cancers occur in Asia, with China accounting for more than 50% of the world’s burden [3]. Although we have known more and more comprehension of HCC and the treatment is more advanced, its prognosis is still poor. It’s reported that 1 year survival rate of HCC is 47% [4]. Five-year survival rate is less than 10% [5]. The mortality rate has been a high trend [6].
Screening of the high risk population of HCC could contribute to early detection, early diagnosis and early treatment, which are the key to improve the efficacy of hepatocellular carcinoma. The serum alpha-fetoprotein (AFP) and ultrasound (US) are the primary means of early screening. Current guidelines recommend that US should be performed every 6 months for surveillance of high-risk groups [7]. However, it is reported that US is not reliable for detecting HCC at the early stage [8]. Although AFP is the most regularly used serum biomarker for HCC diagnosis and surveillance worldwide, it was found to be normal or low concentrations in about 30% of the HCC patients, while increasing levels could be seen in patients with chronic hepatitis and cirrhosis [9, 10]. Thus, it is important to search for new serum markers for the early diagnosis of HCC.
Prothrombin induced by vitamin K absence-II (PIVKA-II) is a serum biomarker with highly sensitivity and specificity, used for the diagnosis and prognosis monitoring of HCC. PIVKA-II is also superior to AFP in diagnosis of the early stages of HCC [11, 12, 13]. Moreover, it has been suggested that elevated PIVKA-II serum levels is associated with vascular invasion, a major risk factor for recurrence and mortality in HCC [14, 15, 16], therefore, predicting vascular invasion is important in prognosis management. Hepatitis B virus (HBV) is an important cause of the development of HCC. Although the development of vaccines and antimicrobial therapy can control the infection of HBV to a certain extent, the failure of the control of HBV infection due to a variety of factors has set new obstacles and difficulties for HCC prevention and treatment.
The aim of this study was to compare the accuracy of serum PIVKA-II and AFP levels in the diagnosis of early HCC, and to detect relevance of PIVKA-II and HBV DNA.
Materials and methods
Study subjects
The study was performed in the second Xiangya Hospital of Central South University from November 2016 to March 2017. The diameter of the tumor was measured by ultrasound and/or CT. The tumor differentiation was determined using Edmondson-Steiner grade. HCC staging was determined using the Barcelona Clinic Liver Cancer (BCLC) staging system [7]. Very early HCC (BCLC stage 0) is defined as the presence of a single tumor
Controls were 37 patients with chronic hepatitis, 43 patients with cirrhosis and enrolled during the same period as HCC cases. Healthy controls included 51 healthy volunteers. All patients (chronic hepatitis, cirrhosis and HCC patients) had chronic HBV infection. The study protocol was reviewed and approved by The Second Xiangya Hospital Investigational Review Board. Informed consent was obtained from all participants.
Sample and assay
Peripheral blood was obtained from each patient prior to any HCC treatment. The serum was obtained by centrifuging for 5 min at 3000 rpm and stored at
Baseline characteristics of controls and HCC cases
Baseline characteristics of controls and HCC cases
AST, aspartate aminotransferase; ALT, alanine aminotransferase; n.s., not significant; DBIL, Direct Bilirubin; Alb, Albumin; HC, health control; HCC, hepatocellular carcinoma.
Serum levels of PIVKA-II and AFP among controls and hepatocellular carcinoma cases. #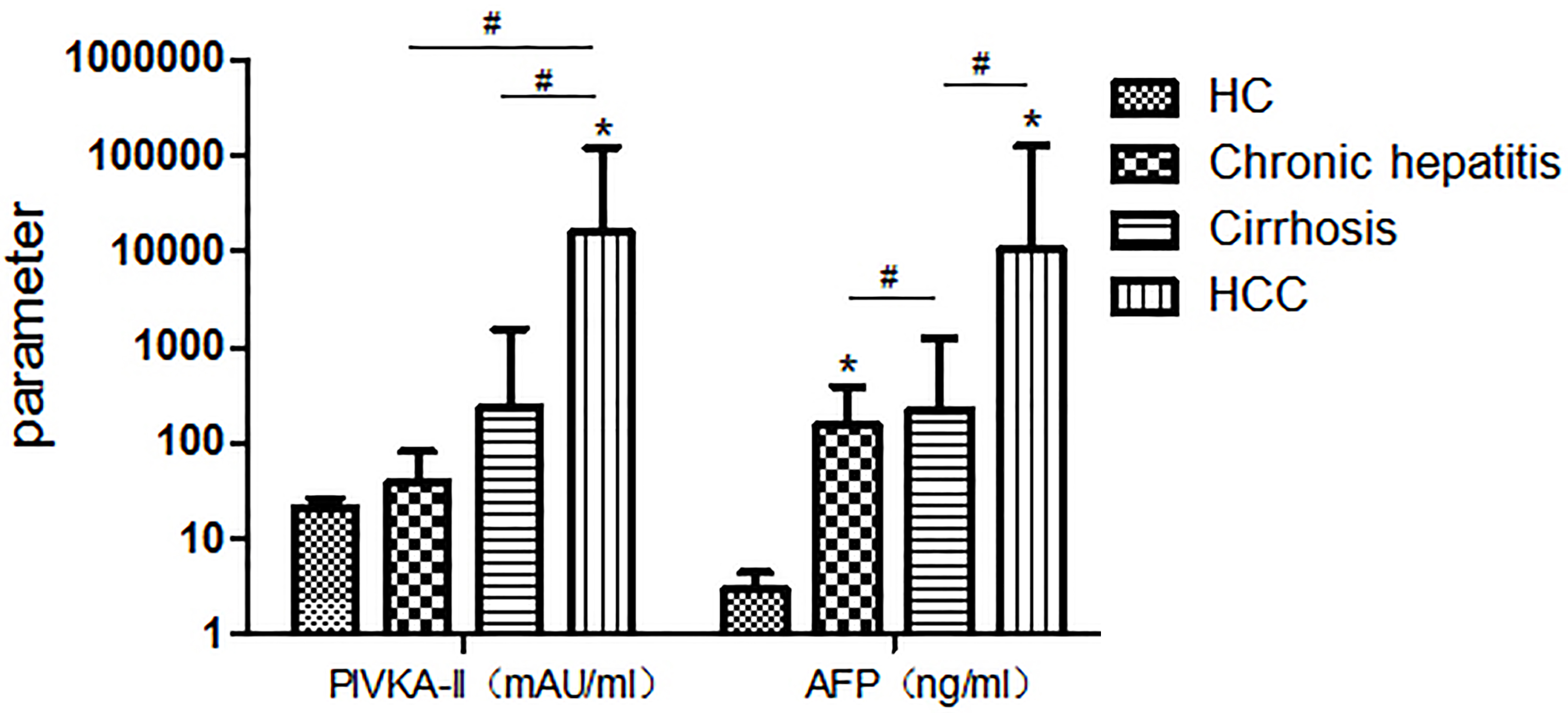
All statistical analyses were carried out with IBM SPSS software (SPSS version 22.0, IBM, USA).
Results
Patient characteristics
Two hundred seventy four participants were divided into four groups: (1) Healthy controls (
PIVKA-II and AFP serum levels in controls and HCC patients
The median PIVKA-II level was significantly higher in HCC patients than in healthy control patients, non-cirrhotic chronic hepatitis patients, cirrhosis without HCC patients (286 (44.5–4540.5) vs. 22 (17.5–25) vs. 25 (14–39) vs. 16 (12–28.5) mAU/ml,
Diagnostic accuracy of the markers to differentiate between malignant cases and controls
Diagnostic accuracy of the markers to differentiate between malignant cases and controls
PPV, positive predictive value; NPV, negative predictive value.
Correlation between AFP and PIVKA-II serum levels and pathological characteristics of hepatocellular carcinomas
PIVKA-II, prothrombin induced by vitamin-K-absence-II; AFP, a-fetoprotein; HCC, hepatocellular carcinoma; *
When the usual clinical cut-offs (40 mAU/ml for PIVKA-II, 10 ng/ml for AFP) were used , the PIVKA-II of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and Kappa were 76.92%, 86.26%, 85.94%, 77.39% and 0.629 and 64.34%, 73.28%, 72.44%, 65.31% and 0.374 for AFP. PIVKA-II had a better performance than AFP for diagnosis of early HCC, with sensitivity of 58.54%, specificity of 82.61%, PPV of 50% and NPV of 87.2%. For AFP, sensitivity, specificity, PPV and NPV were 47.37%, 88.35%, 75%, and 69.47%, respectively (Table 2). According to the cut-off levels (40 mAU/ml for PIVKA-II), 8 cases of 19 patients with very early stage and 16 cases of 29 patients with early stage had elevated PIVKA-II levels.
Performance of PIVKA-II, AFP and a combination of markers in differentiating HCC cases from controls
Receiver operating characteristics (ROC) curve comparing serum levels of PIVKA-II, AFP and a combination of PIVKA-II and AFP in patients with early hepatocellular carcinomas vs. controls.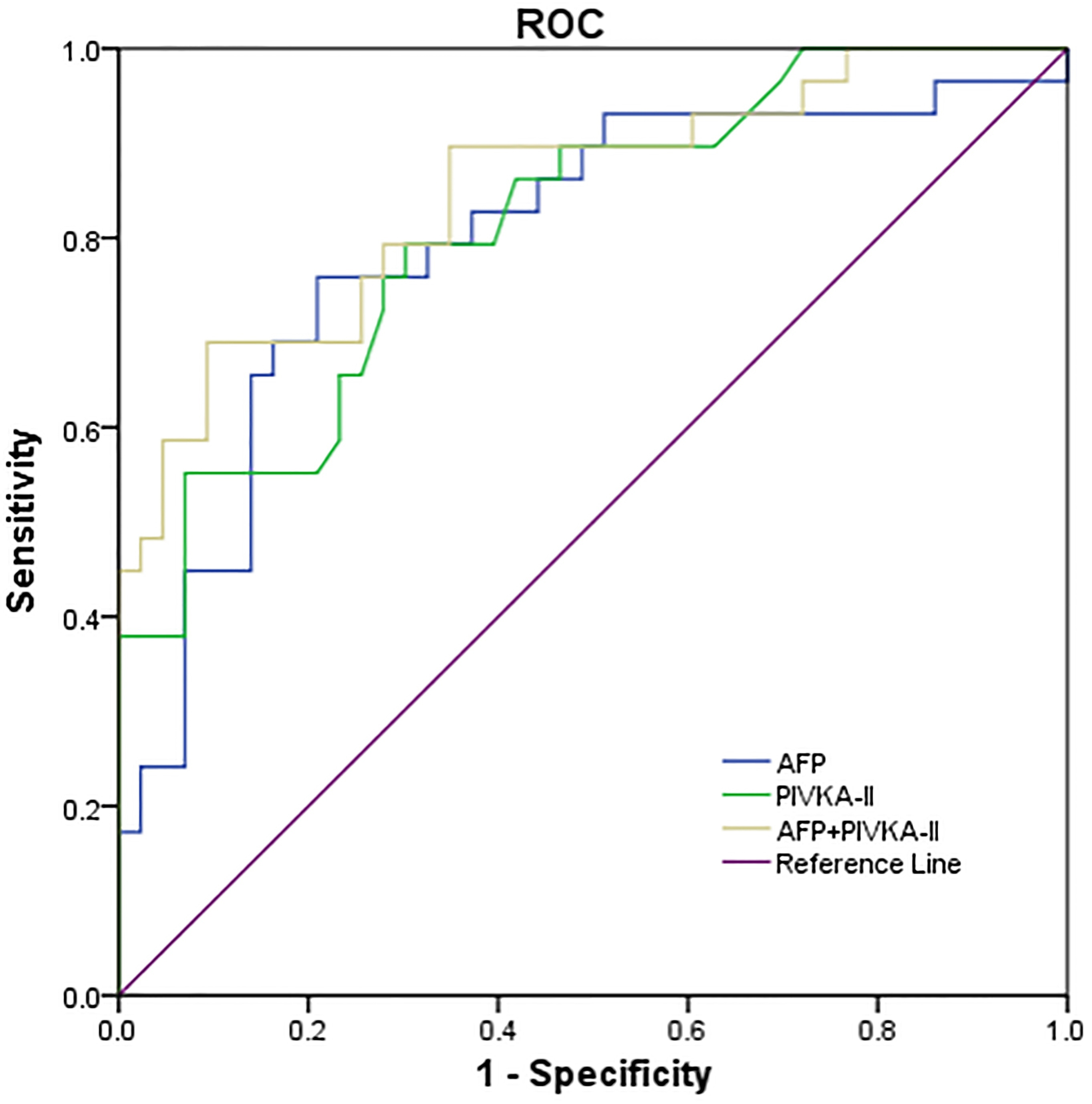
Predictive factors of vascular invasion in hepatocellular carcinomas
PT, prothrombin time; INR, international normalized ratio.
Correlation between serum PIVKA-II and HBV DNA. There was a negative correlation between the serum HBV DNA and the serum PIVKA-II levels in (a) chronic hepatitis patients (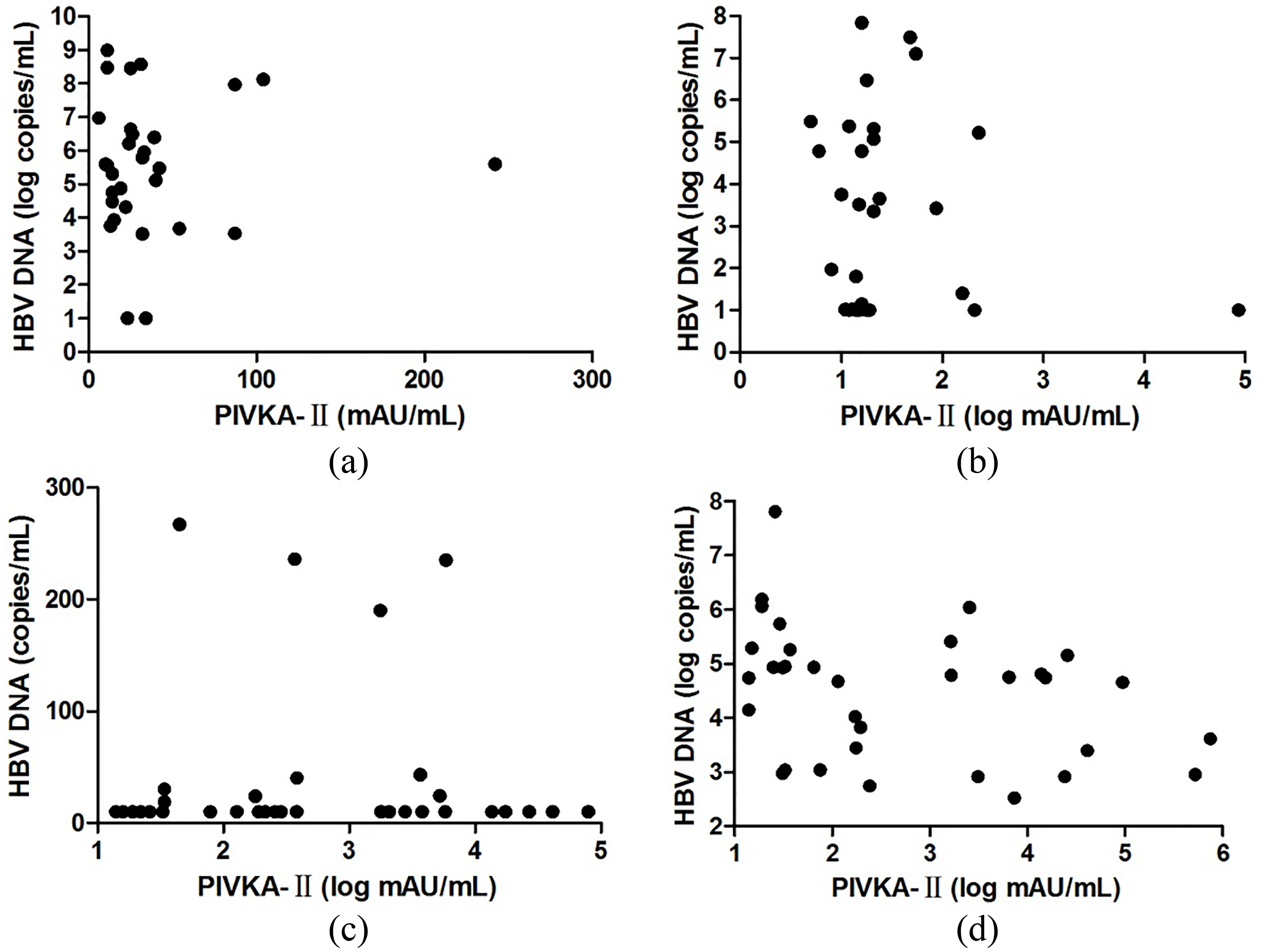
The optimal cutoff values for PIVKA-II and AFP in differentiating HCC cases from non-cirrhotic chronic hepatitis and cirrhosis without HCC controls were 104 mAU/ml and 209.2 ng/ml, respectively. The sensitivity and specificity at these cutoff values were 65.73% and 92.5% for PIVKA-II (AUC 0.862; 95% CI, 0.810–0.904) and 39.86% and 87.5% for AFP (AUC 0.671; 95% CI, 0.606–0.733), respectively. The optimal cutoff values for PIVKA-II and AFP in differentiating HCC cases from cirrhosis without HCC controls were 26 mAU/ml and 7.66 ng/ml, respectively. The sensitivity and specificity at these cutoff values were 74.42% and 86.01% for PIVKA-II (AUC 0.803 ; 95% CI, 0.738–0.857) and 79.1% and 76.2% for AFP (AUC 0.873 ; 95% CI, 0.817–0.917), respectively.
The performance of PIVKA-II in differentiating early HCC cases from cirrhosis without HCC controls was also better than that of AFP (AUC 0.812; 95% CI, 0.702–0.894 vs. 0.797; 95% CI, 0.686–0.883), with a sensitivity of 69.77% and a specificity of 79.31% at a cut-off of 21 mAU/ml. For AFP, sensitivity and specificity for a cut-off of 7.66 ng/ml were 75.86% and 79.07%, respectively. The combination of PIVKA-II and AFP slightly improve the diagnostic performance for early HCC (AUC 0.849; 95% CI, 0.745–0.923) , and slightly improved performance of the overall HCC diagnosis (AUC 0.924; 95% CI, 0.876–0.958) (Fig. 2).
In the HCC group, the PIVKA-II serum level was significantly higher in moderately/poorly differentiated HCC. In the tumor size group, the PIVKA-II serum level showed significant differences between any two subgroups. In the BCLC staging group, the PIVKA-II serum level was significantly higher in the early stage and late stage compared to the very early stage group. In the number of nodules group, the PIVKA-II and AFP serum level had no significant differences. The AFP serum level showed no significant differences in the tumor size group, tumor differentiation group and BCLC staging group (Table 3).
Predictive factors for vascular invasion
In this study, we collected the vascular invasion result of 91 HCC patients in, which 31 patients have vascular invasion. As summarized in Table 4, the PIVKA-II serum level and Direct Bilirubin were statistically significant predictors of vascular invasion in univariate analysis. On multivariate analysis, a PIVKA-II level
The serum level of HBV DNA and he association of serum PIVKA-II and HBV DNA
In the chronic hepatitis group, there is no correlation between serum PIVKA-II and serum HBV DNA (
In HCC patients, we collected the serum level of HBV DNA in 68 patients among 143 HCC patients. We detected a negative association between serum PIVKA-II and serum HBV DNA levels in the HBeAg-negative HCC group (
Discussion
In this study, we evaluated the performance of PIVKA-II for the diagnosis of HCC and explored the relationship between PIVKA and different clinic-pathologic features. Our study showed that the serum PIVKA-II level had a better performance than AFP in distinguishing patients with HCC from the patients with nonmalignant disease. For the diagnosis of early HCC and the overall HCC, the combination of PIVKA-II and AFP slightly improve the diagnostic performance. In addition, the PIVKA-II serum level
PIVKA-II was found originally in patients with HCC by Liebman in 1984 [17]. Prothrombin is usually synthesized by the liver in the body. The Gla region, one of the functional domains has 10
In recent years, many studies were conducted in Asian countries, and proved the PIVKA-II had an excellent performance on the diagnosis of HCC. Our results are consistent with them [7, 21, 22, 23, 24, 25]. In this study, the serum levels of PIVKA-II and AFP in serum samples were measured in 143 HCC patients, 37 patients with chronic hepatitis, 43 patients with liver cirrhosis and 51 healthy subjects. The results showed that PIVKA-II was more sensitive and specific than AFP in the diagnosis of HCC, and its consistency with the gold standard was better than that of AFP, included early HCC. The combination of the AFP and PIVKA-II could compensate for the deficiency of single marker. In different clinic-pathologic features, the performance of PIVKA-II was still better than AFP. It is worth noting that according to the cut-off levels (40 mAU/ml for PIVKA-II), 8 cases of 19 patients with very early stage and 16 cases of 29 patients with early stage had elevated PIVKA-II levels. In the very early and early HCC group, PIVKA-II has the sensitivity of 58.54% and the specificity of 82.61%, respectively. In this experiment, the sensitivity of PIVKA-II to early and very early HCC is still not ideal, may be related to too few cases, or we may observe only a single result. Continuous monitoring of serum PIVKA-II levels may be important to the diagnosis of early HCC. We found the correlation between serum PIVKA-II level and several HCC prognostic factors, such as tumor size, tumor differentiation and BCLC staging. We detected a negative association between serum PIVKA-II and serum HBV DNA levels.
Some studies have shown that persistent HBV infection may be the main cause of liver cancer. HBV infection may be related to liver cell damage and cancer, vascular proliferation and cancer tissue infiltration have been HBV-related [26].Recent studies have shown that HBV-DNA load is closely related to the recurrence of HCC, so it is important to detect HBV-DNA in the blood of patients [27, 28]. However, in this study, we detected a negative association between serum PIVKA-II and serum HBV DNA levels. The reason may be that persistent infection of HBV causes normal function of liver cells, causing abnormal elevation of PIVKA-II.
More and more studies quested the accuracy of PIVKA-II in European patients [29, 30, 31], with different demography and the etiology of liver diseases from Asian patients. These studies also proved PIVKA-II was more sensitive than AFP for differentiating HCC from patients with cirrhosis or chronic hepatitis. The present study showed that the PIVKA-II level was an independent predictor of vascular invasion and high PIVKA-II serum and tissue expression are associated with vascular invasion. As reported, PIVKA-II promotes proliferation and migration [32], and stimulates overexpression of vascular endothelial growth factor (VEGF) [33].
However, there are still some shortcomings in this study. First, this study is a retrospective study and a prospective study are needed to examine the changes in serum PIVKA-II levels in high risk population, such as cirrhosis, to assess the applicability of PIVKA-II in HCC monitoring. Second, there are many kinds of the liver-related diseases. In order to observe the clinical value of PIVKA-II, the more disease control groups should be added. Third, this study included only 143 patients with HCC who had no BCLC stage D patients. Fourth, false-positive elevated PIVKA-II concentrations are found in patients with the presence of vitamin K deficiency, the use of anticoagulants, or poor nutritional status associated with alcoholic abuse or jaundice [31]. With the continuous improvement of detection assays, NX-DCP, detected by P-11 and P-16 monoclonal antibody, was proved to have better performance than conventional PIVKA-II [35, 36, 37, 38].
In conclusion, our study shows that PIVKA-II is currently the better serum biomarker for early and very-early HCC diagnosis than AFP. Although prospective studies in a large cohort of patients are needed, the existing research results suggest that PIVKA-II could be used as a screening biomarker for HCC in high risk population. Moreover, we found that high PIVKA-II serum levels are significantly associated with the presence of vascular invasion and other pathological characteristics.
Footnotes
Acknowledgments
This work was supported by the Hunan Science and Technology Project (Grant No. 2014FJ3096).
Conflict of interest
The authors declare no competing financial interests.