
Abstract
BACKGROUND:
Neutrophil-Lymphocyte Ratio (NLR) and Platelet-Lymphocyte Ratio (PLR) have been considered as indicators for prognosis in various cancers. However, the prognostic values of NLR and PLR have never been tested in gallbladder carcinoma (GBC) with hepatic involvement.
OBJECTIVE:
The aim of the current study was to assess the prognostic significance of NLR, PLR, and other candidate biomarkers in GBC with liver involvement.
METHODS:
Receiver operating characteristic (ROC) curve analyses were utilized to pinpoint the cut-off values for NLR, PLR, and Monocyte-Lymphocyte Ratio (MLR). Univariate analyses were employed to estimate the impact of NLR, PLR, MLR, and other inflammatory indexes on median survival. Multivariate analyses were used to verify the independent prognostic predictors.
RESULTS:
Eighty four patients were enrolled from 2009 to 2017. The cut-off values for NLR, PLR, and MLR were 3.20, 117.75, and 0.25, respectively. Univariate analyses revealed that TNM stage, NLR, PLR, MLR, lactate dehydrogenase, alkaline phosphatase, and carcinoembryonic antigen were significantly associated with decreased survival in GBC with hepatic involvement. Advanced TNM stage (
CONCLUSIONS:
These findings suggest that preoperative NLR may be an independent prognostic factor in evaluating prognosis in GBC with liver involvement.
Introduction
Gallbladder cancer (GBC) is the predominant malignant tumor of the biliary system, with a poor overall 5-year survival rate, ranging from 5% to 10% [1, 2]. The sole potential curative treatment for GBC is to completely remove the gallbladder through surgery (cholecystectomy). Improvements in imaging technology including multi-slice spiral computed tomography (MSCT) and biliary magnetic-resonance imaging (MRI) have allowed moderately accurate preoperative staging of these diseases and have been helpful to surgeons for preoperative planning [3, 4]. Nonetheless, because GBC patients are often asymptomatic or initially describe nonspecific symptoms, detection of early-stage gallbladder cancer remains difficult [5, 6]. Patients are usually already at an advanced stage when diagnosed, thus complicating surgical management. As such, survival outcomes in GBC remain poor even in patients who undergo aggressive surgical treatment [7, 8]. Due to the anatomic position, GBC is likely to spread to the liver, either by direct invasion, hematogenous spread, and/or lymphatic spread. Previous studies have shown that liver involvement is a prognostic factor for decreased survival in GBC patients [9, 10, 11].
Inflammation is normally a protective reaction that aids in repairing tissue injury and in defending against pathogens. However, if inflammation becomes dysregulated, it can induce malignant transformation in the surrounding tissue [12, 13]. Indeed, the role of inflammation in cancer development is an important emerging area of study, and cancer-related inflammation has already been hailed as a hallmark of cancer [14]. Recent research has linked chronic inflammation to the development of GBC [15, 16], as well as other digestive system cancers, including stomach, intestine, and liver [17, 18, 19]. The relative abundance of immune-related cells, including neutrophils, lymphocytes, and platelets, can provide information about the state of a patient’s immune system and inflammatory state. Due to the low cost and ease of access, pretreatment Neutrophil-Lymphocyte Ratio (NLR) and Platelet-Lymphocyte Ratio (PLR) have been widely used as indicators of systemic inflammation in cancer patients. Neutrophils and platelets have been demonstrated to promote tumor development and protect cancer cells from the normal anti-cancer immune response mediated by lymphocytes, and thus elevated NLR and PLR ratios are thought to reflect a pro-cancer shifted inflammatory environment (see Discussion for more).
The prognostic significance of NLR and PLR has previously been demonstrated in non-small cell lung cancer (NSCLC), metastatic melanoma, and colorectal cancer [20, 21, 22]. Recently, NLR and PLR have also been examined as candidate biomarkers for GBC prognosis [23, 24]. However, there is still a need for further investigation of specific biomarkers associated with overall survival in GBC that involves the liver. The aim of the present study was to assess the merits of several inflammatory markers, including NLR, PLR, and Monocyte-Lymphocyte Ratio (MLR), as prognostic indicators of survival in patients with GBC with liver involvement.
Materials and methods
Patients
A retrospective review of all patients with histologically confirmed diagnosis of GBC in West China Hospital of Sichuan University from September 2009 to July 2017 was performed, excluding all those without hepatic involvement. Hepatic involvement was confirmed by radiological methods, including endoscopic ultrasonography, MRI and MSCT, and/or by pathological findings. Patients who were less than 18 years of age, had a recent infection, or had received any medication that might alter inflammatory markers, were excluded from further study. Approval for this retrospective study was obtained from the institution ethics commission of Sichuan University. Written informed consent was obtained from all included patients.
Data extraction and follow-up
Patients were regularly evaluated with radiological examinations and laboratory tests in West China Hospital of Sichuan University. The last follow up was June 30, 2017. All data were obtained from electronic medical records. Specifically, the following data were obtained: patient demographics, imaging results, pathology reports, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, lactate dehydrogenase (LDH), carcinoembryonic antigen (CEA), alkaline phosphatase (ALP), triglycerides, cholesterol, and peripheral blood cell counts including neutrophils, platelets, monocytes, and lymphocytes. The data were analyzed by both univariate and multivariate analyses to identify potential markers of prognosis in GBC patients with hepatic involvement.
Statistical analysis
The Pearson Chi squared test was performed to determine whether or not the differences between patients grouped by NLR, PLR, and MLR were significant. ROC curve analyses were used to determine the optimal cut-off values of pretreatment NLR, PLR, and MLR according to the maximum joint specificity and sensitivity. Survival curves were estimated by Kaplan-Meier univariate analyses and the differences between survival curves were compared with the log-rank test. Cox regression models were used to perform univariate analyses as well as multivariate analyses on potential prognostic factors. SPSS version 21.0 was used for data analysis.
Clinicopathological demographic features stratified by NLR, PLR, and MLR
Clinicopathological demographic features stratified by NLR, PLR, and MLR
NLR
From a total of 560 patients, 84 (15%) met the inclusion criteria for further study. The median (range) age was 62 (40–96) years and 56 (67%) patients were female. Following ROC analyses, the optimal cut-off values of NLR, PLR, and MLR were found to be 3.20, 117.75, 0.25 with a sensitivity of 0.813, 0.833, 0.896 and a specificity of 0.639, 0.472, 0.472 respectively. The corresponding areas under the curve for NLR, PLR, and MLR were, respectively, 0.683 (95% CI: 0.562–0.805,
Univariate and multivariate analyses of the prognostic utility of candidate biomarkers for survival in GBC with liver involvement
Univariate and multivariate analyses of the prognostic utility of candidate biomarkers for survival in GBC with liver involvement
GBC
The univariate survival analysis for the survival time of patients in the low (
The univariate survival analysis for the survival time of patients in the low (
The univariate survival analysis for the survival time of patients in the low (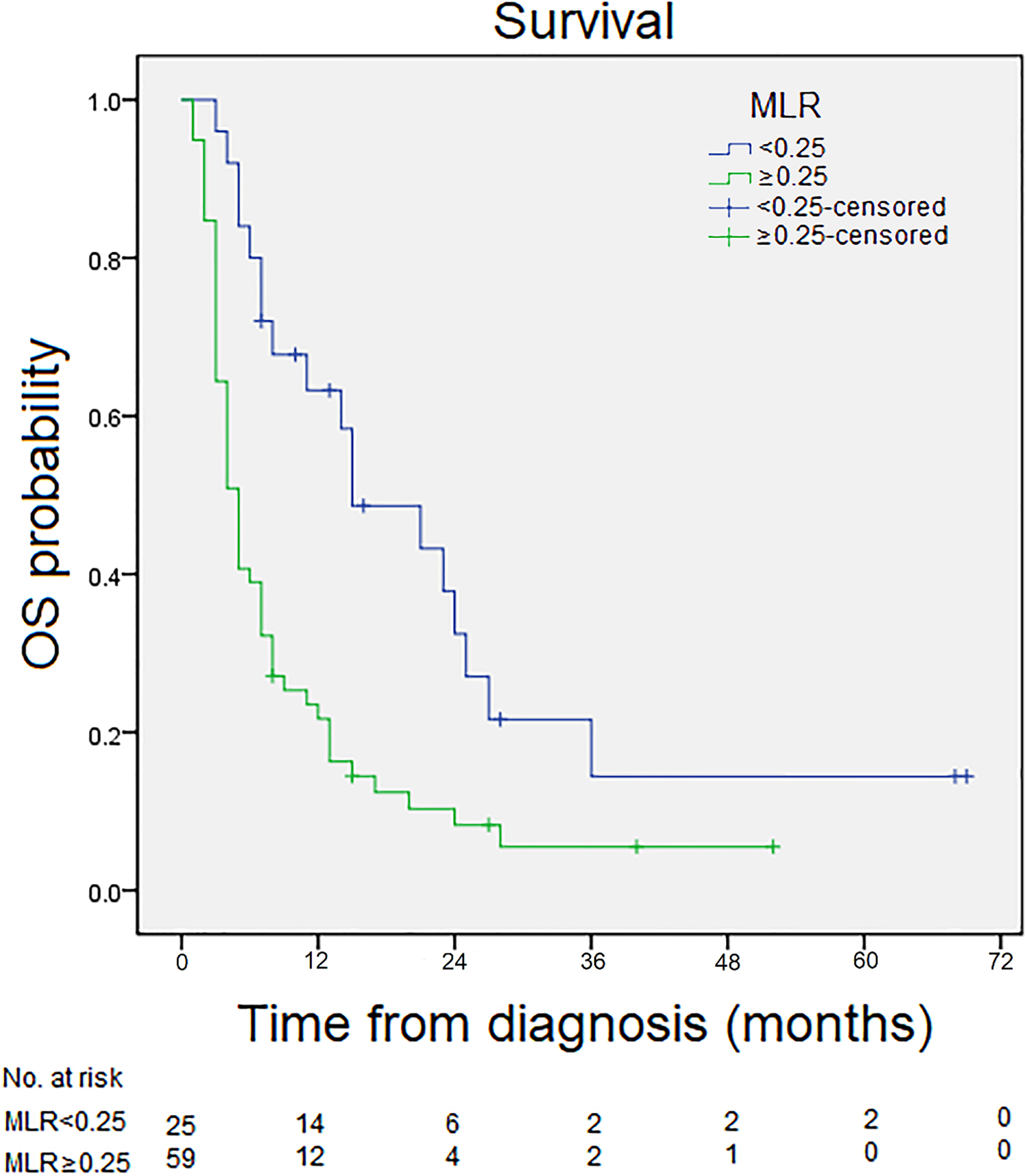
During follow-up, 72 (86%) patients died and 12 were censored at the last follow-up. The demographic baseline data and comparisons of clinicopathological parameters, stratified by NLR, PLR, and MLR threshold value, are listed in Table 1. All patients included in the current study were at TNM stages III or IV. Significant differences were found in LDH, ALP, and AST among all NLR, PLR, and MLR subgroups (
TNM stage, NLR, PLR, MLR, LDH, ALP, and CEA were significantly associated with the survival outcomes of liver involvement GBC in the univariate analyses (Table 2). The median survival time of participants in the low NLR group was 17 months, compared with 4 months in the high NLR group (
Pathological TNM staging has been considered to be the most accurate index of long-term survival in cancer patients. Indeed, its utility as an independent prognostic index for survival in GBC with liver involvement has been confirmed here. However, a major limitation of TNM staging is that it can only be properly estimated after surgery. The aim of the present study was to explore the merits of several pretreatment inflammatory biomarkers as prognostic indicators of survival outcomes for GBC patients with hepatic involvement. Unlike TNM staging, these inflammatory indexes can be determined prior to performing surgery, and they may be valuable tools to supplement TNM staging for determining prognosis for patients with GBC with liver involvement.
Historically, NLR was employed as an indicator of systemic inflammation in critically ill patients (such as multiple trauma or major surgery) [25]. Subsequent studies found that reactive oxygen species generated by neutrophils are mutagenic, leading to premalignant lesions [26, 27]. Recent studies have demonstrated that tumor-associated neutrophils (TANs) can regulate the tumor microenvironment by producing various cytokines and/or chemokines that participate in immunosculpting and immunoediting [28, 29]. TANs, together with tumor-associated macrophages, encourage tumor cells to extravasate from the circulation and embed into a new tissue site [29]. In GBC, neutrophil-bound tumor cells engage integrins and induce ICAM-1 clustering on the tumor cell, stimulating a cellular migration towards the liver [30, 31].
In contrast to the reported pro-tumor functions of neutrophils, lymphocytes play an essential role in cancer immune surveillance, which suppresses the maturation of tumor cells [32]. Thus, the Neutrophil-Lymphocyte Ratio may be interpreted as reflecting the balance between deleterious inflammation and proper immune surveillance, with a high NLR suggesting a pro-cancer inflammatory environment, and a low NLR suggesting a protective, anti-tumor inflammatory environment. The present finding of increased NLR being associated with significantly decreased survival time is consistent with this interpretation of NLR, and supports the utility of NLR as a prognostic biomarker of survival in patients with GBC with liver involvement. Furthermore, NLR was the only independent prognostic biomarker, suggesting that it may be superior to PLR and MLR in the absence of other biomarkers.
There are several ways that platelets can promote tumor development. Platelets facilitate the arrest of tumor cells at the endothelium, which promotes the establishment of secondary lesions [33, 34]. In addition, the release of VEGF and other angiogenic factors by platelets during platelet-endothelium interaction modifies the angiogenic balance in the tumor microenvironment [35]. Platelets also protect tumor cells from the immune response through various mechanisms, including steric shielding from NK cells, inhibiting NK cell-mediated cytolysis, and altering MHC I expression [36]. Platelet-tumor cell interaction results in extensive membrane changes that suppress immune cytotoxicity and support the survival and spread of tumor cells [37]. The presence of tumor-infiltrating lymphocytes (TILs) is an important prognostic factor associated with superior clinical outcomes [38, 39], but platelets can shield tumor cells from being accessed by TILs [36]. The present finding that PLR is associated with decreased survival time in GBC with hepatic involvement is consistent with the previously described pro-cancer role of platelets, and we speculate that some of these mechanisms may be at play in the context of GBC with liver involvement.
Representing the relative levels of peripheral monocytes and lymphocytes, MLR was found to have an inverse relationship with survival in GBC with hepatic involvement. This finding is consistent with reports of various pro-cancer processes mediated by tumor-associated macrophages (TAMs), which are a major component of the infiltrate found within the stroma of many tumors. Derived from circulating monocytes, most TAMs are considered to have an M2 phenotype, meaning they can produce growth and angiogenic factors as well as proteases to degrade the extracellular matrix [40]. Thus, it has been speculated that TAMs can stimulate tumor cell proliferation, promote angiogenesis, and enhance invasion and metastasis [41].
Since our results showed that GBC patients with increased NLR tend to have a poorer prognostic outlook, these patients may benefit from more intensive postoperative care and careful follow-up.
A few limitations of the current study should be noted. First of all, although patients from 2009 to 2017 were analyzed, the sample size of available participants was still relatively small. Hence, larger prospective cohorts are still required to more completely investigate the values of NLR, PLR, and MLR as predictors of survival in GBC patients with liver involvement. Secondly, since the study was restricted to a Chinese population, the results may not apply to other ethnic populations.