
Abstract
We intended to investigate the functional role and clinical relevance of microRNA-125b in human gallbladder cancer. Quantitative real-time polymerase chain reaction was used to examine microRNA-125b expression in gallbladder cancer cell lines, and 79 pairs of gallbladder cancer and normal gallbladder clinical tissues. Clinical correlations between tumorous microRNA-125b expression and gallbladder cancer patients’ clinicopathological variances or overall survivals were statistically analyzed. In gallbladder cancer cell lines, TYGBK-8 and G-415 cells, microRNA-125b was upregulated to examine its regulatory effect on gallbladder cancer proliferation and migration in vitro. MicroRNA-125b was significantly downregulated in gallbladder cancer cell lines and human gallbladder cancer tumors. MicroRNA-125b in gallbladder cancer was significantly correlated with patients’ clinical stage, tumor differentiation, lymph metastasis, and tumor invasion. Low tumorous microRNA-125b expression was also found to be associated with poor overall survivals among gallbladder cancer patients. In vitro studies demonstrated that microRNA-125b upregulation significantly suppressed proliferation and migration in TYGBK-8 and G-415 cells. Tumorous microRNA-125b is an independent prognostic biomarker for patients with gallbladder cancer and possibly acts as a tumor suppressor in gallbladder cancer.
Introduction
Gallbladder cancer (GBC) is a rare cancer in human digestive system but with high mortality rate. 1 In the United States alone, approximately 12,000 new cases of GBC were diagnosed, and approximately 4000 patients died of GBC every year. 2 Despite recent advances in combined chemotherapy or surgery, the estimated 5-year survival rate of GBC patients remains relative low, between 20% and 30%.1,3–5 Most specifically, due to no obvious symptoms and lack of efficient diagnostic tools, most GBC patients, once diagnosed, were already at advanced stages. 5 Thus, it is critical to seek novel diagnostic biomarkers or therapeutic reagents to develop early diagnosis strategy and improve clinical outcomes for patients with GBC.
MicroRNAs (miRNAs) are families of short (18–22 nucleotides long), noncoding, evolutionarily conserved, single-stranded RNAs that attach to the complimentary binding site of 3′-untranslational region (3′-UTR) on their targeted genes, and thus exert various biological functions through post-transcriptional gene downregulation.6–8 Recently, many miRNAs have been shown to be aberrantly deregulated, thus acting as useful biomarkers or functional regulators in human cancers.9–11 However, only a few miRNAs had been identified as potential prognostic markers or therapeutic targets in GBC.12–14 The full molecular blueprint of miRNAs expression and their clinical implication in GBC is largely unknown.
MicroRNA-125b (miR-125b) has been found to be dysregualted in cancer patients’ plasma or carcinoma tissues, and may be used as a biomarker to predict cancer chemoresistance in breast cancer, and patients’ prognosis in non-small-cell lung cancer.15,16 In a recent microarray study, it was demonstrated that miR-125b was downregulated in tumorous tissues of patients with GBC. 13 However, the exact expression profile, functional mechanisms or clinical relevance of miR-125b in GBC, has not been elucidated.
In this study, we used quantitative measurement of quantitative real-time polymerase chain reaction (qRT-PCR) to definitively examine the endogenous expression of miR-125b in GBC cell lines, as well as clinical samples of GBC tumors. In 79 patients diagnosed with GBC and underwent cholecystectomy, their clinicopathological variances and overall survival (OS) were followed up and statically analyzed based on their tumorous miR-125b expression. In addition, in GBC cell lines, TYGBK-8 and G-415 cells, we ectopically upregulated miR-125b to examine the possible tumor suppressing role of miR-125b in regulating GBC proliferation and migration in vitro.
Patients, materials, and methods
Ethic statement
Ethic approvals for conducting all experiments in our study were approved by the Clinical Study and Ethic Committee at Second Military Medical University in Shanghai, China. All participating patients signed consent forms. All protocols were performed in accordance with the Declaration of Helsinki, local and national regulations on good clinical practice.
Patients and clinical samples
Paired GBC samples and adjacent non-carcinoma gallbladder epithelial samples were obtained from 79 patients who received cholecystectomy at Second Military Medical University in Shanghai, China, between June 2005 and September 2010. GBC tumors were sectioned and examined by independent histologists. Their classification of tumor, lymph node, metastasis (TNM) stages was then determined in accordance to the International Union Against Cancer and the American Joint Committee on Cancer. 17 Immediately after surgery, clinical samples were snap-frozen in liquid nitrogen and stored at −70°C to be further used for RNA extraction.
Cell lines
In our study, a normal gallbladder epithelial cell line, N-GB, was generated at the East Hepatobiliary Hospital, Second Military Medical University, according to the method described previously. 18 GBC cell lines, TYGBK-1, TYGBK-8, OCUG-1, and NOZ were purchased from National Institutes of Biomedical Innovation, Health and Nutrition (NIBIOHN) JCRB Cell Bank (Japan). Other GBC cell lines, G-415, TGBC1TKB, TGBC2TKB, TGBC14TKB, and TGBC24TKB, were purchased from RIKEN Cell Engineering Division-Cell Bank (Japan). All GBC cell lines were maintained in phenol red–free Dulbecco’s modified Eagle’s medium (DMEM; Thermo Fisher Scientific, USA), supplemented with F12 medium (DMEM; Thermo Fisher Scientific, USA), 10% fetal calf serum (FCS; Thermo Fisher Scientific, USA), penicillin (100 U/mL), and streptomycin (100 µg/mL; Thermo Fisher Scientific, USA) in a tissue culture chamber with 5% circulating CO2 at 37°C.
RNA isolation and qRT-PCR
Total RNA was isolated from GBC cell lines or clinical samples using a mirVana miRNA Isolation kit (Thermo Fisher Scientific, USA) according to the manufacturer’s instructions. For each sample, 0.5-µg RNA was reversely transcribed into complementary DNA (cDNA) using an iScript Reverse Transcription SuperMix kit (Thermo Fisher Scientific, USA) according to the manufacturer’s instructions. qRT-PCR to detect hsa-miR-125b was then performed using an miRNA TaqMan assay (Thermo Fisher Scientific, USA) on an ABI Prism 7000 sequence detection system (Thermo Fisher Scientific, USA) according to the manufacturer’s instructions. Nucleolus RNA sno135 was used as a loading control. For each sample, relative miR-125b expression was characterized using 2−ΔΔCt methods, and normalized to the miR-125b expression in control cell lines or non-carcinoma gallbladder epithelial tissues. Mean data were averaged from biological triplicates.
Upregulation of MiR-125b in GBC
Human miR-125b mimics oligonucleotides (miR-125b-mimic) and control non-specific miRNA mimics oligonucleotides (C-miR) were purchased from RiboBio (Guangzhou, China). GBC cell lines, TYGBK-8 and G-415 cells, were transfected with C-miR or miR-125b-mimic with Oligofectamine 2000 (Thermo Fisher Scientific, USA) for 48 h. Forty-eight hours after transfection, endogenous miR-125b expression was examined by qRT-PCR to confirm the upregulation efficiency.
Proliferation assay
Proliferation of GBC cell lines, TYGBK-8 and G-415 cells, was characterized using a CellTiter-96 AQueous One Solution Cell Proliferation Assay (MTS assay; Promega, USA) according to the manufacturer’s instructions. Briefly, miRNA-transfected TYGBK-8 and G-415 cells were suspended and re-plated in 96-well plates at a density of 5000 cells per well. On days 1, 2, 3, 4, and 5, 20-µL MTS medium was mixed into culture well for 30 min. Optical densities (ODs) at 570 nm, representing proliferation rates of GBC cells, were then measured by a Synergy-2 multimode microplate reader (BioTek, USA) according to the manufacturer’s instructions.
Migration assay
Migration of GBC cells was characterized using a transwell assay. MiRNA-transfected TYGBK-8 and G-415 cells were treated with mitomycin (20 µg/mL; Thermo Fisher Scientific, USA) for 20 min to stop proliferation. They were then suspended and re-plated in the Matrigel-coated upper chambers of transwell inserts (Corning, USA) in 12-well plates. The upper chambers were filled with culture medium but without FCS. The lower chambers were filled with normal culture medium (with 10% FCS). Twenty-four hours later, upper chambers were removed. The lower chambers were fixed, immunostained with crystal violet, and imaged using an Olympus inverted microscope (IX71; Olympus, Japan). The number of migrated TYGBK-8 or G-415 cells were tallied for each chamber, and normalized to the cell number in control chambers.
Statistical analysis
In our work, statistical analysis was performed using version 11.0 SPSS software (SPSS, USA). Student’s t-test was used for comparison of miR-125b gene expression, in vitro GBC proliferation and migration. Chi-square test was used to assess correlation of miR-125b with patients’ clinicopathological variances. The Kaplan–Meier method with log-rank test was used to assess patients’ OS. Cox proportional hazard models with 95% confidence intervals (CIs), including both univariate and multivariate analyses, were used to assess correlation of patient’s clinicopathological variances with OS. Differences were considered to be statistically significant if p < 0.05.
Results
MiR-125b is downregulated in both GBC tumors and cell lines
In a previous microarray study, it was suggested that miR-125b was downregulated in GBC tumors. 13 In our work, we used qRT-PCR to definitively examine the expression pattern of miR-125b in GBC. From 79 patients with GBC, miR-125b expression was compared between GBC tumors and non-carcinoma gallbladder epithelial tissues. It showed that miR-125b was significantly downregulated in GBC tumors than in normal gallbladder tissue samples (Figure 1(a), *p = 0.005). We then compare miR-125b expression between GBC cell lines, including TYGBK-1, TYGBK-8, OCUG-1, NOZ, G-415, TGBC1TKB, TGBC2TKB, TGBC14TKB, TGBC24TKB, and a normal gallbladder epithelial cell line, N-GB. It showed that miR-125b was significantly downregulated in all examined GBC cell lines than in N-GB cells (Figure 1(b), *p < 0.05).
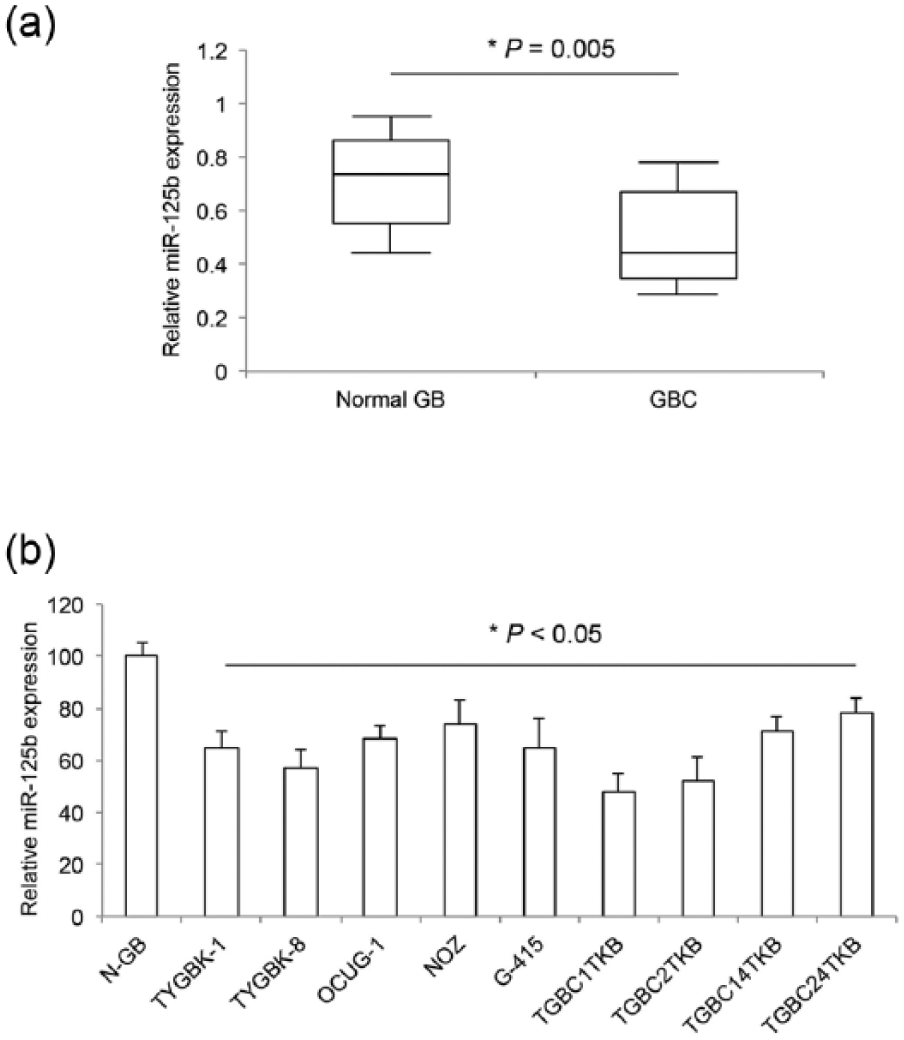
Expression of miR-125b in clinical GBC samples and GBC cell lines. (a) Paired GBC tumors (GBC) and their adjacent non-carcinoma normal gallbladder epithelial tissues (Normal GB) were extracted from 79 patients. Quantitative real-time polymerase chain reaction (qRT-PCR) was used to compare endogenous miR-125b expression between Normal GB tissues and GBC tissues (*p = 0.005). (b) qRT-PCR was also used to compare endogenous miR-125b expression between a normal gallbladder epithelial cell line, N-GB cells, and GBC cell lines, TYGBK-1, TYGBK-8, OCUG-1, NOZ, G-415, TGBC1TKB, TGBC2TKB, TGBC14TKB, and TGBC24TKB (*p < 0.05).
MiR-125b is associated with clinicopathological variances of patients with GBC
GBC patients were divided into two groups according to the median miR-125b expression in their tumors. One group had 41 patients, whose tumorous miR-125b expressions were lower than the median value. The other group had 38 patients, whose tumorous miR-125b expressions were higher than the median value. The correlation of patients’ miR-125b expressions with their clinicopathological variances was then statistically analyzed (Table 1). We found that, some of the clinicopathological variances, including patients’ sex, age, tumor size, and GBC pathology, were similar between patients with low miR-125b expressions and patients with high miR-125b expressions. On the other hand, several clinicopathological variances, including patients’ TNM stage, tumor differentiation status, lymph metastasis, and invasion status, were significantly different between patients with low miR-125b expressions and patients with high miR-125b expressions (Table 1, *p < 0.05).
Correlation of miR-125b and clinicopathological variances of patients with GBC.
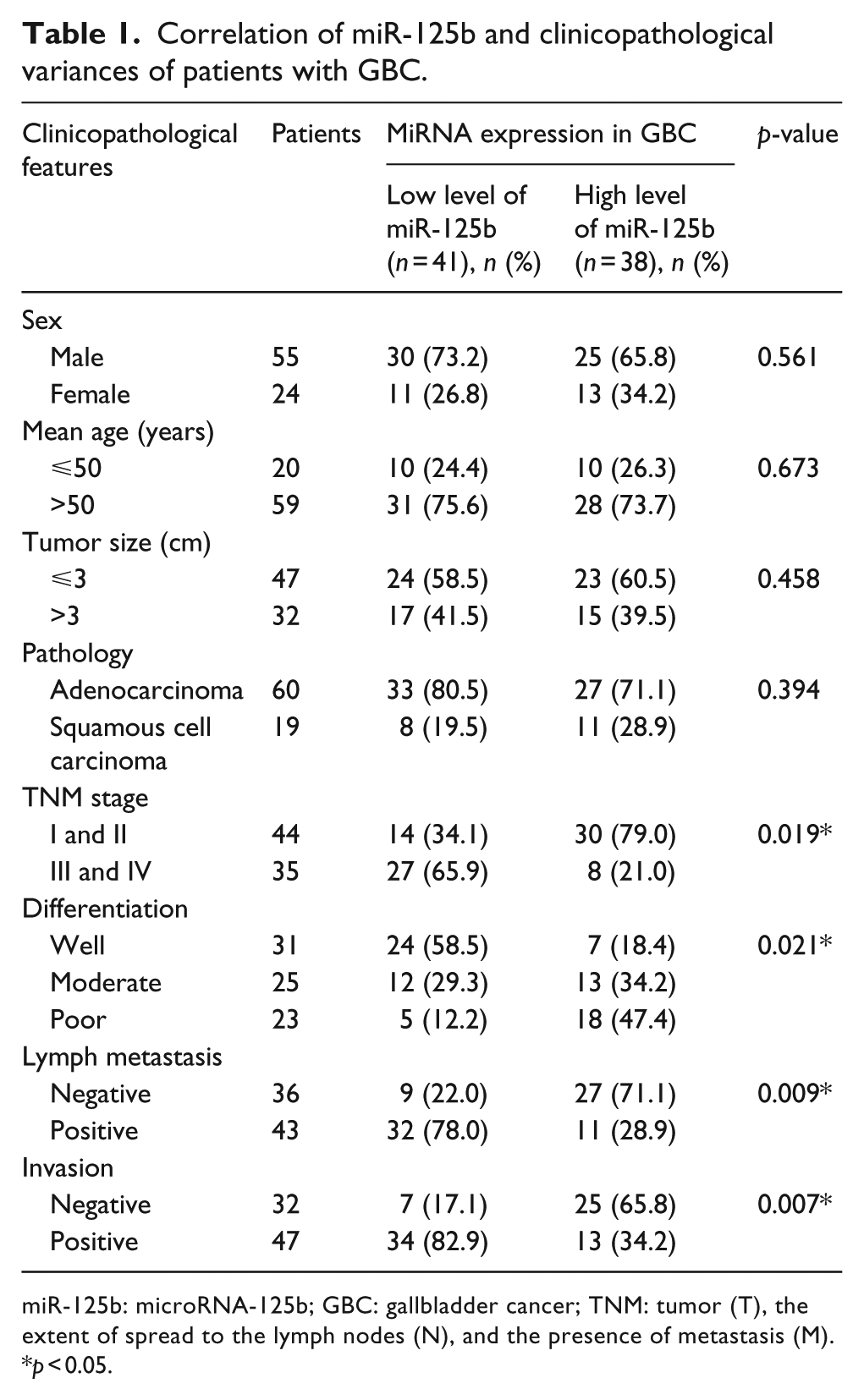
miR-125b: microRNA-125b; GBC: gallbladder cancer; TNM: tumor (T), the extent of spread to the lymph nodes (N), and the presence of metastasis (M).
p < 0.05.
MiR-125b downregulation is associated with poor prognosis of patients with GBC
After cholecystectomy, patients were followed up to 60 months. Their OSs were estimated using the Kaplan–Meier method, and compared between patients with low miR-125b expressions and patients with high miR-125b expressions using the log-rank test. It showed that patients with low miR-125b expressions had much worse survival rates than patients with high miR-125b expressions (Figure 2, p = 0.007, log-rank test).

GBC patients’ overall survivals according to miR-125b expression. GBC patients’ overall survivals (OS) were censored by Kaplan–Meier model, for patients with low miR-125b expressions and for patients with high miR-125b expressions (p = 0.007, log-rank test).
We then used Cox regression model to examine the correlation of patients’ OS with their clinicopathological variances (Table 2). Univariate analysis showed that patients’ TNM stage (p = 0.021, hazard ratio = 1.543, 95% CI = 1.121–1.743), differentiation status (p = 0.018, hazard ratio = 1.194, 95% CI = 0.902–1.382), lymph metastasis (p = 0.009, hazard ratio = 2.977, 95% CI = 1.893–4.731), invasion (p = 0.020, hazard ratio = 1.764, 95% CI = 1.346–2.086), and miR-125b expression in GBC tumors (p = 0.003, hazard ratio = 4.882, 95% CI = 3.875–6.381) were significantly correlated with OSs among patients with GBC. Furthermore, multivariate analysis demonstrated that patients’ TNM stage (p = 0.034, hazard ratio = 1.319, 95% CI = 1.021–1.508), lymph metastasis (p = 0.018, hazard ratio = 1.865, 95% CI = 1.387–2.275), and miR-125b expression in GBC tumors (p = 0.009, hazard ratio = 2.789, 95% CI = 1.458–4.782) were independent prognostic factors for GBC patients’ OS.
Correlation of OS and clinicopathological variances of patients with GBC.

OS: overall survival; GBC: gallbladder cancer; TNM: tumor (T), the extent of spread to the lymph nodes (N), and the presence of metastasis (M); CI: confidence interval; miR-125b: microRNA-125b.
p < 0.05.
MiR-125b upregulation suppressed GBC proliferation and migration
In order to elucidate the functional mechanism of miR-125b in GBC development, we transfected GBC cell lines, TYGBK-8 and G-415 cells, with human miR-125b mimics (miR-125b-mimics) to upregulate endogenous miR-125b. GBC cells were also transfected with a non-specific miRNA mimics (C-miR) as a parallel control. Forty-eight hours after transfection, qRT-PCR confirmed that miR-125b was significantly upregulated in TYGBK-8 and G-415 cells (Figure 3(a), *p < 0.05). Transfected TYGBK-8 and G-415 cells were then suspended from dishes and re-plated in 96-well plates. GBC proliferation was then assessed by a proliferation assay. It showed that, in both TYGBK-8 and G-415 cells, miR-125b upregulation significantly suppressed GBC proliferation rates 3 to 5 days after the onset of assay (Figure 3(b), *p < 0.05).

MiR-125b upregulation inhibited in vitro GBC proliferation. (a) TYGBK-8 and G-415 cells were transfected with C-miR or miR-125b-mimic with Oligofectamine 2000 for 48 h. qRT-PCR was then used to assess endogenous miR-125b expression in transfected GBC cells (*p < 0.05). (b) Transfected TYGBK-8 and G-415 cells were examined by a proliferation assay for 5 days (*p < 0.05).
Transfected TYGBK-8 and G-415 cells were also assessed through a migration assay. It showed that significantly less GBC cells migrated into lower chambers if cells were transfected with miR-125b, rather than transfected with C-miR (Figure 4(a) and (b), left). After counting the cell numbers in lower chambers, it clearly demonstrated that miR-125b upregulation significantly suppressed migration in TYGBK-8 and G-415 cells by approximately 40% (Figure 4(a) and (b), right, *p < 0.05).

MiR-125b upregulation inhibited in vitro GBC migration. (a) TYGBK-8 cells and (b) G-415 cells transfected with C-miR or miR-125b-mimic were examined by a transwell migration assay. Twenty-four hours later, representative images were shown for cells migrated into lower chambers (left). Relative migration was compared between cells transfected with C-miR and cells transfected with miR-125b-mimic (right, *p < 0.05).
Discussion
In a recent study, Letelier and colleagues 13 conducted a microarray assay on 21 clinical GBC tissues and found that a total of 481 miRNAs were expressed in GBC carcinomas. They also found that 36 miRNAs were consistently downregulated in GBC carcinomas than in normal gallbladder epithelial tissues, including miR-125b. 13 However, at that time, qRT-PCR was not performed to verify the downregulation of miR-125b in GBC carcinoma. 13 Thus, in this study, we followed up on that study by conducting thorough qRT-PCR to examine miR-125b expression not only in clinical GBC carcinomas with larger sample size (79 pairs of samples vs 21 samples in previous study 13 ) but also in in vitro GBC cell lines. And the results of our qRT-PCR analysis demonstrated that miR-125b was indeed downregulated in both GBC carcinomas and GBC cell lines, not only confirming the finding of previous study 13 but also in line with other studies showing miR-125b was downregulated in carcinomas of breast cancer, ovarian cancer, thyroid cancer, and hepatocellular cancer.19–22
Previous studies had demonstrated that circulating miR-125b might be used as diagnostic biomarkers for patients with breast cancer and non-small-cell lung cancer.15,16 However, until now, no study has shown whether or not miR-125b could also have a similar role in GBC diagnosis. Therefore, the puzzle is resolved in our study, as we elucidated the clinical relevance of miR-125b in GBC. Our data showed that low miR-125b expression in GBC tumors was statistically correlated with patients’ advanced TNM stages, advanced tumor differentiation status, positive lymph metastasis, and positive tumor invasion. Moreover, we followed up on patients’ OS rates between those with high miR-125b expression and those with low miR-125b expression. Analysis of the log-rank test then revealed that low miR-125b expression was also statistically correlated with poor survival. Most importantly, using the multivariate Cox regression model, we discovered that low expression of miR-125b in GBC was an independent prognostic marker to predict the OS of GBC patients.
Also in this study, we took one step further to investigate the possible cancer-regulating role of miR-125b in GBC. After transfecting TYGBK-8 and G-415 cells with miR-125b mimics, we demonstrated that in vitro GBC proliferation and migration were dramatically suppressed by miR-125b upregulation. These results are in line with similar inhibitory effect of miR-125b on cancer development in breast cancer,19,23 suggesting that miR-125b is predominantly a tumor suppressor in both GBC and breast cancer. Interestingly, studies also demonstrated that miR-125b could act as an oncogene by promoting carcinoma proliferation and migration in prostate cancer and endometrial cancer.24,25 Therefore, it is critical for future investigators to unravel the intricate signaling pathways associated with miR-125b to further understand its regulatory functions in GBC.
In conclusion, we discovered a novel diagnostic biomarker, as well as a functional tumor suppressor of miR-125b in GBC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.