
Abstract
BACKGROUND:
GDF-15 is a protein belonging to the transforming growth factor beta superfamily that has a role in regulating inflammatory and apoptotic pathways. High level GDF-15 in tumor tissues and plasma correlate with an increased risk of recurrence and reduced overall survival.
OBJECTIVE:
The aim of this study was to screen GDF-15 capacity to detecting metastatic CRC and compare it with standard tumor markers CEA and CA19-9.
METHODS:
We collected serum samples from 97 patients with metastatic colorectal cancer and 79 samples from healthy controls. Serum levels of GDF-15, CEA and CA19-9 were measured by immunochemically. A Kaplan-Meier curve was applied for analysis of survival rates, and a log-rank was used for univariate analysis.
RESULTS:
Serum levels of GDF-15 were significantly higher in patients with colorectal cancer compared to healthy controls (
CONCLUSIONS:
Our results show GDF-15 as an effective biomarker in patients with metastatic colorectal cancer with the same sensitivity as CEA. In addition, GDF-15 levels strongly correlate with extension of liver involvement in contrast with CEA.
Introduction
Colorectal cancer is the third most common cancer in men (746,000 cases, 10.0% of the total) and the second in women (614,000 cases, 9.2% of the total) worldwide [1]. Patient outcome strongly depends on the stage of tumor at the time of diagnosis and in metastatic disease the prognosis depends on localization and extent of distant metastases [2]. Early detection and diagnosis still present the best chance for successful treatments and improved outcomes. Early detection of metastatic liver disease is important for indication of liver surgery. Therefore, novel biomarkers for earlier cancer detection and early detection of metastatic disease are strongly needed.
GDF-15 also known as non-steroidal anti-inflamm-atory drugs (NSAIDs) activated gene (NAG-1), growth differentiation factor 15 (GDF-15), prostate differentiation factor (PDF), or placental bone morphogenetic protein (PLAB), is a protein belonging to the transforming growth factor beta superfamily that has a role in regulating inflammatory and apoptotic pathways in injured tissues and during disease processes [3]. GDF-15 mRNA is most abundant in the liver, with lower levels seen in some other tissues [4]. GDF-15 over expression is associated with different cancers, including gastric, pancreatic, prostate, colorectal cancer, breast and melanoma [5, 6, 7, 8, 9, 10, 11, 12]. Moreover, GDF-15 is also overexpressed in adenomatous colonic polyps [12].
Many studies have revealed the important role of GDF-15 in CRC. It has been observed that GDF-15 expression levels are markedly enhanced in malignant tissues, established cancer cells and plasma during the transition of numerous localized cancers to invasive and metastatic disease stages as compared with non-malignant tissues, normal cells, and basal GDF-15 concentration in serum [5, 7, 9, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22]. GDF-15 deregulation is involved in the progression of colon cancer, and research showed that the GDF-15 levels in serum gradually increase in the process of conversion from adenomatous polyps to colorectal carcinoma. There is a significant positive relationship between serum GDF-15 levels, clinical stage, presence of metastasis and progression of CRC [20].
Meta-analysis published by Li et al. [23] summarizes the diagnostic and prognostic performance of serum GDF-15. From all studies only 8 were included in the meta-analyses. They summarized that serum GDF-15 levels in CRC patients were higher than those in healthy controls (SMD
In our study, we investigated the serum levels of GDF-15 in the patients with metastatic colorectal cancer compared to the healthy controls. This study compares the levels of GDF-15 to standard biomarkers used in monitoring of colorectal cancer (CEA and CA19-9) and that studies correlation of tumor characteristics and treatment outcomes to the serum levels of GDF-15.
Materials and methods:
Patients and healthy control characteristics
Between November 2011 and May 2013, 97 patients with metastatic CRC and 79 healthy individuals were included in this study. The serum samples from patients were collected before beginning treatment for mCRC (
All patients had adequate liver and renal function (transaminases
Laboratory analyses
Blood for laboratory analyses was collected after overnight fasting via puncture of the cubital vein, simultaneously with blood collection for routine examinations. Routine biochemical parameters were measured in fresh samples. For special parameters, blood was standardly centrifuged for 10 min at 3000 rpm (rotations per minute) and serum was stored at
Statistical analysis
Statistical analysis was performed using SAS (SAS Institute Inc., Cary, NC, USA). Basic statistics were calculated for parameters measured in the whole group and in different groups and subgroups, such as mean, standard deviation, variance, median, interquartile range, minimum, maximum. Selected statistical data were also graphically processed, Box & Whisker plot diagrams. Non-parametric analysis of variance two-sided Wilcoxon test was used for comparison of the distribution of the individual parameters in the different groups and subgroups. Due to non-Gaussian distribution of variables Spearman’s correlation coefficient was used to determine the dependency of characters. Statistical significance was determined at the border of alpha
Results
Baseline characteristic of patients and controls
In the cancer group serum 97 patients with generalized colorectal cancer were included (38.1% women and median of age was 64 years). In a majority of patients (
In the cancer group serum level of CEA was 308.3
Serum levels of GDF-15
Serum level of GDF-15 in the cancer group was 7.58
GDF-15 levels in patients with colorectal cancer and healthy controls (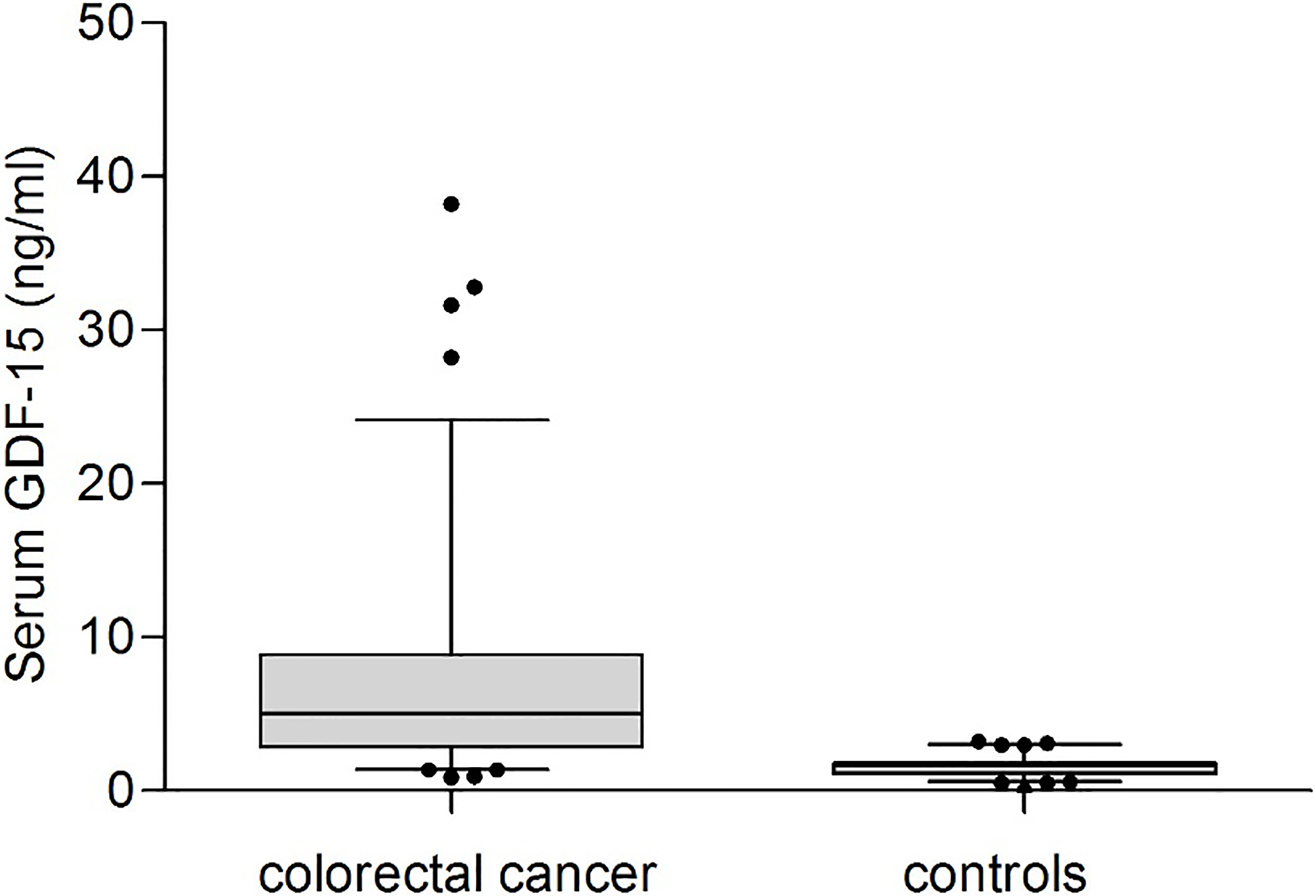
In the cancer group, there was no significant difference between sex, age, part of colon with primary tumor and tumor grade (Table 1). There was indicated difference in presence or absence of the primary tumor (
Serum GDF-15/MIC-1 levels in different groups
The group of patients with liver metastases only was divided into patients with the sum of the longest dimension of liver metastases smaller than 100 millimeters (
The serum levels of GDF-15 in patients without pulmonary and with liver metastasis. Sum of liver metastases larger than or equal to 100 mm, smaller than 100 mm and healthy controls.
ROC curves analysis showed that serum GDF-15 with an AUC of 0.921 (Fig. 3A) and serum level cut-off 3.5 ng/ml has the sensitivity and specificity to distinguish colorectal cancer from healthy controls are 65.98% and 97.47%, respectively (
ROC curve analysis of GDF-15. GDF-15 (AUC 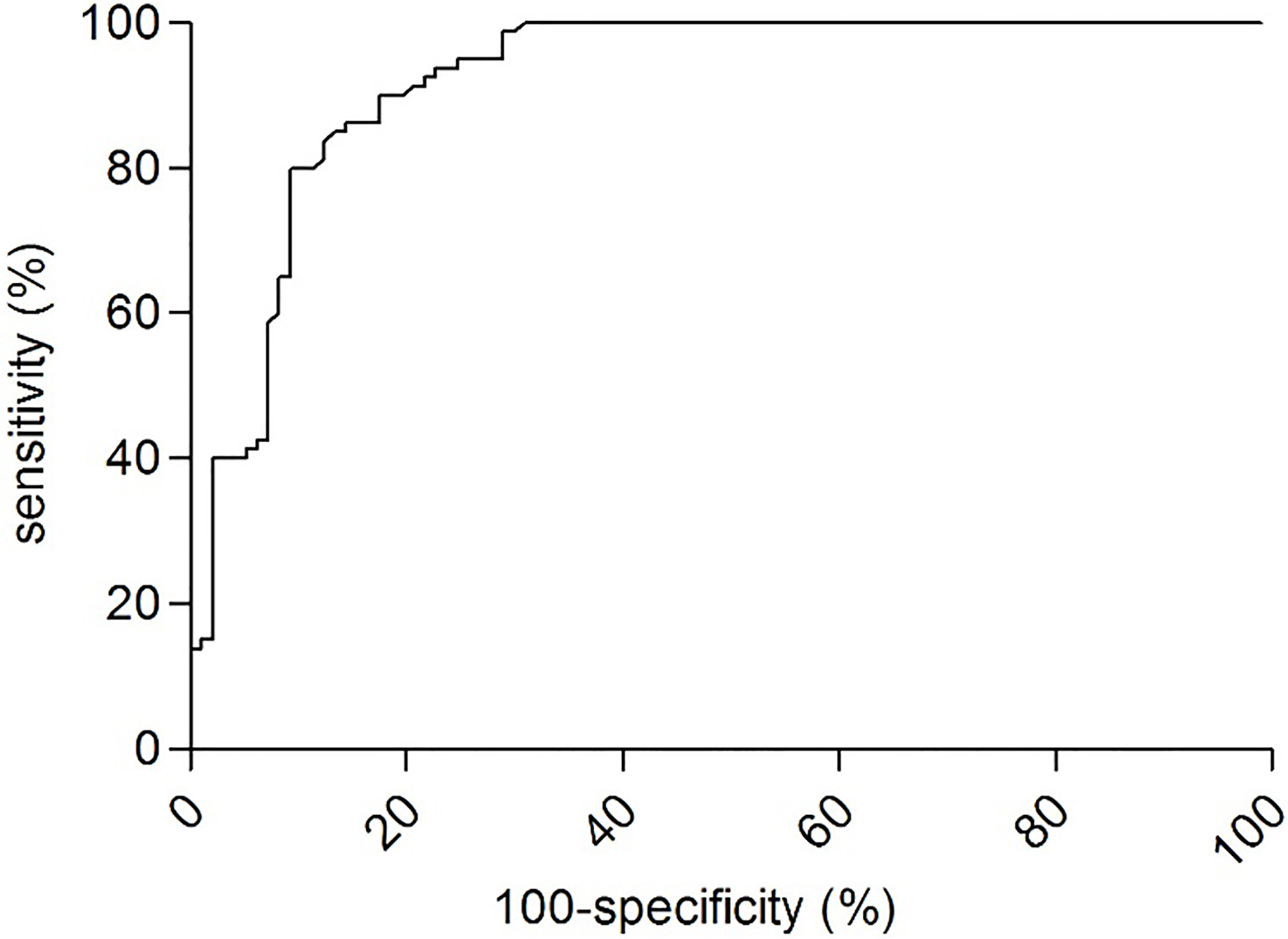
The serum level of GDF-15 appears to have a prognostic value. The cut-off for serum GDF-15 level was determined as 3.5 ng/ml. Patients were divided into the group with negative serum levels of GDF-15 (
Overall survival according to GDF-15 levels. Kaplan-Meier curves of patients with GDF-15 level 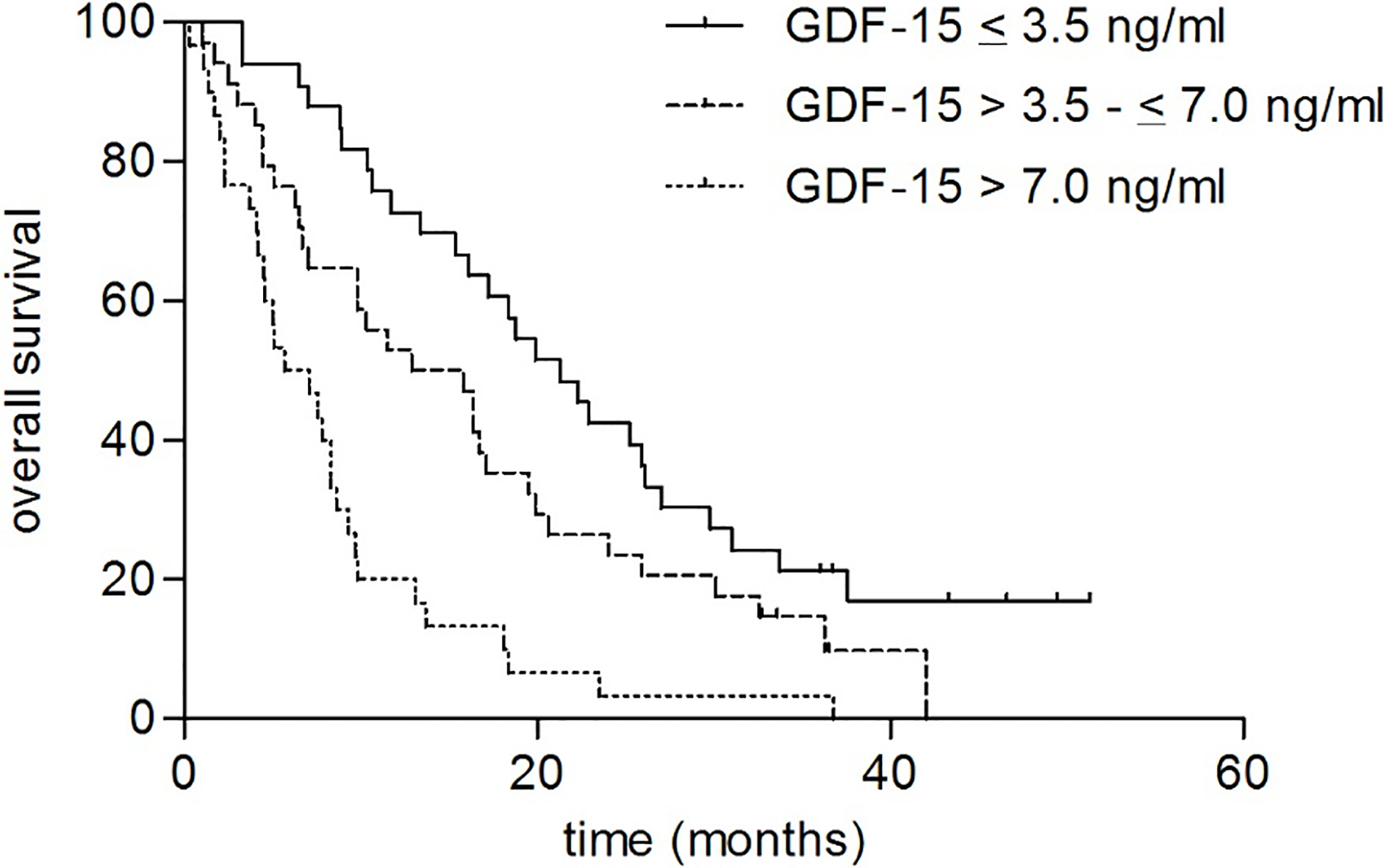
Early diagnosis is crucial for successful treatment even in metastatic colorectal cancer with liver involvement. Therefore, new biological markers for early detection (more sensitive and specific than CEA and CA19-9) and predictors of prognosis for colorectal cancer are urgently needed in clinical practice.
Many studies have evaluated the application of GDF-15 in the diagnosis and prognosis of CRC; however, there are some inconsistent results which have been reported. GDF-15 expression level is usually low in resting cells but may be substantially increased following response to diverse cellular stress signals, such as hypoxia, inflammation, light exposure, acute tissue injury and during cancer progression [25, 26, 27].
The meta-analysis published by Li et al. [23] shown results of GDF-15 that achieved a sensitivity of 58.9%, specificity of 92.08% and AUC of 0.816 (similar results as in our analysis), indicating that GDF-15 has a good diagnostic performance for CRC. Moreover, they suggested that GDF-15 expression level could be a prognostic biomarker in CRC patients. Compared with patients with low GDF-15 expression level, patients with an increased level of GDF-15 had a 2.09-fold higher risk of death. These results suggested that GDF-15 could serve as a diagnostic and prognostic biomarker in CRC [23].
Earlier studies identified serum GDF-15 as a new marker for colon cancer, but they are comparing only CRC vs controls without information about stage [28], only few blood samples were available [19, 20, 23] or only limited number of patients in stage IV were examined or assess stage III and IV as one group [28]. Direct comparison with data from other studies is very difficult due to small number of mCRC patients in earlier studies and only limited information about results of this patients separately. Wallin et al. [20] published levels of GDF-15 in mCRC patients (146.5 pg/ml), but only in 8 cases and it was measured in plasma. All studies with patients in stage IV do not present any data about side of distant metastasis and none compare GDF-15 with standard tumor markers (CEA and CA19-9) was not investigated.
We found that serum GDF-15 levels were significantly higher in patients compared to controls and it correlate with the extent of colon or rectum involvement (non-resected primary tumor or local recurrence), also with the extent of liver involvement only. This finding is promising because these patients could be candidates for a radical resection of liver metastases, the only modality than can complete cure them.
The GDF-15 has the same sensitivity and specificity as CEA. These results suggested that serum GDF-15 could be a useful biomarker. The entry level of GDF-15 appears to be a prognostic factor which strongly correlates with overall survival. This can be partially explained by correlation of GDF-15 serum levels with liver involvement (especially in patient without pulmonary metastases). The patients with sum of liver metastases larger than 100 mm had significantly higher levels of GDF-15 and their liver reserve is smaller. Another partial explanation could be, that patients with non-resected primary tumor, who have higher levels of GDF-15, were not operated because of their worse performance status and that may be the reason for a worse outcome of the treatment. Further investigation and data are needed to clarify these results.
Conclusions
Our data indicated that serum GDF-15 can serve as an effective serum tumor marker for the detection of distant metastasis with the same sensitivity as CEA and better sensitivity than CA19-9. Our data have shown that GDF-15 strongly correlates with extension of liver involvement in patients without pulmonary metastases, who are the candidates for a curative liver resection. The entry level of GDF-15 appears to be prognostic factor that correlates with overall survival.
Footnotes
Acknowledgments
The study was supported by research projects TIP ČR FR-TI3/666, Progres Q25/LF1 and MH CZ DRO VFN 64165. The authors are thankful to nurses from the Clinical Departments and to laboratory staff for technical assistance.