
Abstract
Despite initial responsiveness, acquired resistance to both bevacizumab and chemotherapy in metastatic colorectal cancer is universal. We have recently published that in vitro, chronically oxaliplatin resistance upregulates soluble vascular endothelial growth factor receptor 1, downregulates vascular endothelial growth factor, and also promotes c-MET, b-catenin/transcription factor 4, and AKT activation. We tested whether variation in three serum biomarkers such as the natural c-MET ligand (hepatocyte growth factor), soluble vascular endothelial growth factor receptor 1, and vascular endothelial growth factor-A was associated with efficacy in metastatic colorectal cancer patients treated in the prospective BECOX study. Serum levels of vascular endothelial growth factor-A165, soluble vascular endothelial growth factor receptor 1, and hepatocyte growth factor were assessed by enzyme-linked immunosorbent assay method basally and every 3 cycles (at the time of computed tomography evaluation) in a preplanned translational study in the first-line BECOX trial in metastatic colorectal cancer patients treated with CAPOX plus bevacizumab. Response was evaluated by routine contrast-enhanced computed tomography by RECIST 1.1 by investigator assessment and by three blinded independent radiologists. Ratios between soluble vascular endothelial growth factor receptor 1/vascular endothelial growth factor-A and hepatocyte growth factor/vascular endothelial growth factor-A were established and variations through time were related to RECIST 1.1 by investigator assessment and independent radiologist. The BECOX trial included 68 patients, and 27 patients were analyzed in the translational trial. A total of 80 RECIST 1.1 evaluations were done by investigator assessment and 56 by independent radiologist. We found that a 3.22-fold increase in soluble vascular endothelial growth factor receptor 1/vascular endothelial growth factor-A by investigator assessment and a 3.06-fold increase in soluble vascular endothelial growth factor receptor 1/vascular endothelial growth factor-A by independent radiologist from previous determination were associated with responses compared with 1.38-fold increase by investigator assessment and 1.59 by independent radiologist in non-responders (p = 0.0009 and p = 0.03, respectively). Responders had a 3.36-fold increase in hepatocyte growth factor/vascular endothelial growth factor-A from previous determination by investigator assessment and 3.66-fold increase in hepatocyte growth factor/vascular endothelial growth factor-A by independent radiologist compared with 1.43-fold increase by investigator assessment and 1.53 by independent radiologist for non-responders (p = 0.002 and 0.003, respectively). In conclusion, a decrease in vascular endothelial growth factor-A and an increase in soluble vascular endothelial growth factor receptor 1 during chemotherapy and bevacizumab exposure can contribute to both chemotherapy (due to c-MET/b-catenin activation) and bevacizumab (due to low vascular endothelial growth factor requirements) resistance. Because hepatocyte growth factor levels decrease also during acquired resistance, alternative strategies to hepatocyte growth factor–ligand inhibition should be investigated.
Keywords
Introduction
Colorectal carcinoma (CRC) is the third most common cancer worldwide and the second leading cause of cancer-related deaths. Use of anti-angiogenic treatments in conjunction with chemotherapy has become an accepted standard of care for metastatic colorectal cancer (mCRC). Despite of this, the median progression-free survival (PFS) is only between 9 and 10 months and acquired resistance to both anti–vascular endothelial growth factor (VEGF) therapy (bevacizumab) and chemotherapy is almost universal.1,2
Angiogenesis, defined as the formation of new blood vessels from a preexisting vasculature, is essential for tumor growth and the spread of metastases. The VEGF pathway is a key network of proteins that regulate angiogenesis. VEGF is a family of five structurally related proteins comprising VEGF-A, VEGF-B, VEGF-C, VEGF-D, and placental growth factor (PlGF). VEGF-A is the most important pro-angiogenic factor in tumorigenesis. Circulating VEGF-A functions primarily through two tyrosine kinase receptors, VEGFR1 (or Fms-like tyrosine kinase 1 (FLT1)) and VEGFR2 (or kinase insert domain receptor (KDR)), and neuropilin-1 serves as an important coreceptor. VEGF-A has become a particularly important target in anti-tumor drug development, and many anti-angiogenic drugs target VEGF-A, for example, bevacizumab (monoclonal antibody anti-VEGF-A).3,4
Currently, there are no predictive markers for bevacizumab efficacy. VEGF, interleukin-8, basic fibroblast growth factor (bFGF), PlGF, hepatocyte growth factor (HGF), stromal derived factor-1 (SDF-1), thrombospondin-1 (TSI-1), and soluble vascular endothelial growth factor receptor 2 (sVEGFR2) between others have been proposed as potential markers for bevacizumab resistance, but none of these are used in clinical practice.5,6 Thus, the identification of predictive biomarkers to monitor bevacizumab efficacy still represents a big challenge.
MET is a receptor tyrosine kinase activated by its natural ligand HGF. MET is essential for proliferation, migration, and tissue regeneration and has been associated to VEGF resistance. 7 However, mutations 8 or amplification 9 of MET is very rare (<1%) in untreated mCRC. Therefore, alternative mechanisms of MET activation would probably be important for intrinsic (primary) and secondary (acquired) VEGF resistance in mCRC. Moreover, the increment of HGF induced by cancer-associated fibroblast has been associated pre-clinically to anti-EGFR resistance in colorectal cancer cell lines through MET activation.10,11 We have recently published another mechanism that in chronically oxaliplatin-resistant cells upregulate the soluble vascular endothelial growth factor receptor 1 (sVEGFR1) and downregulate VEGF, inducing MET, AKT, and β-catenin/transcription factor 4 (TCF-4) activation and promoting VEGF independence. 12
Based on our pre-clinical findings, we tested whether variation in three serum biomarkers, VEGF, sVEGFR1, and the HGF, were associated with chemotherapy and bevacizumab efficacy in the phase II study (BECOX trial, NCT01067053). The BECOX trial was designed to investigate the efficacy and safety of a bevacizumab plus XELOX regimen as a first-line treatment in elderly population diagnosed of mCRC. 13
Materials and methods
Study population
This was a prospective analysis in the phase II clinical trial performed in elderly patients with mCRC in Spain, the BECOX trial. The main inclusion criteria were previously published. 13 Briefly, they were the following: elderly patients (≥70 years old), performance status of 0 or 1, histologically confirmed diagnosis of mCRC not suitable for resection, measurable disease according to RECIST version 1.1, not prior systemic therapy for metastatic disease, and prior adjuvant chemotherapy ended >12 months before starting the study. Exclusion criteria included brain metastases, clinically significant cardiac disease, clinical use of full-dose anticoagulants, and major surgical procedures within 28 days before study entry. The study was performed in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki and was approved by local ethics committees. Study population was invited to participate in the preplanned translational study. All patients who agreed to participate in the translational study provided an additional written informed consent. All patients enrolled in the trial received CAPOX–bevacizumab (capecitabine 1000 or 750 mg/m2/12 h for days 1–14, oxaliplatin 130 mg/m2/day for day 1, bevacizumab 7.5 mg/m2/day for day 1) every 3 weeks for 6 cycles. After 6 cycles, oxaliplatin was discontinued and patients continued to receive bevacizumab and capecitabine until progression or study discontinuation.
Assessments
Tumor response was assessed using RECIST version 1.1 at baseline and after the administration of 3 and 6 cycles in the initial treatment phase and every 3 cycles thereafter in the continuation phase. Assessment of overall tumor burden was performed using imaging of thorax and abdomen with computed tomography (CT), resulting in documentation of target and non-target lesions. All patients were invited to participate in the radiologic sub-study, in which response was evaluated using RECIST 1.1 by investigator assessment (IA) and by three blinded independent radiologists (IRs).
Blood samples collection
Venous blood samples were collected before treatment and every 3 cycles at the time of radiologic assessment. Blood samples were centrifuged, and serum was divided in equal aliquots, frozen, and stored at −80°C until assayed. VEGF-A165, sVEGFR1, and HGF serum levels were measured by means of the enzyme-linked immunosorbent assay (ELISA) Quantikine Kit. The optical density was determined using a microplate reader set to 450 nm, with a wavelength correction set to 540 nm.
Statistical analysis
The primary objective of this analysis was to correlate serum biomarkers with response to treatment (comparing responders to non-responders). Ratios between sVEGFR1/VEGF-A and HGF/VEGF-A were established and variations through time in every radiologic evaluation were related by RECIST 1.1. Therefore, every radiologic assessment in every patient was evaluated as one case (responder or non-responder) and correlated with the plasma biomarker ratio changes. Responders were defined as population achieving partial or complete response at any time. Non-responders were defined as population not achieving response at any time (stable disease or progressive disease). Analyses were performed on the intention to treat (ITT) population, which consisted of all patients who received at least one dose of study medication. Survival analyses were performed using Kaplan–Meier method, which provided medians and 95% confidence intervals (CIs).
Results
Between November 2009 and March 2012, 68 patients were enrolled into the BECOX trial at 15 centers in Spain. In all, 57 patients signed the informed consent of the translational study; 30 patients were excluded: 21 patients were excluded because only the basal blood sample or not correlated samples were collected and 9 patients were excluded because their blood samples were not sent to the reference center (Hospital Clinic of Barcelona). Therefore, only 27 patients (39%) from eight centers were evaluable for the translational study (see Figure 1). Baseline characteristics of patients in the translational study did not differ from the 41 patients not evaluated in the BECOX trial (see Table 1). A total of 121 serum determinations were done in 27 patients, with a median of 4 samples for patient (from 2 to 11). Radiologic assessments were done by RECIST version 1.1 by the investigators (IA; n = 80) and by central radiological reviewers (IR; n = 56).

Flowchart of patient study selection.
Patients’ characteristics between patients analyzed and not analyzed in the translational trial.

LDH: lactate dehydrogenase; ULN: upper limit of normal.
The number of administered cycles was also significantly greater in the translational study (median of 13 cycles (3–45)) than in the BECOX trial (median of 6 cycles (1–25); p = 0.004). Overall response rate (ORR) was significantly better in the translational study (66.7%) than in the BECOX population (31%; p = 0.01). Median time to progression (mTTP) and median overall survival (mOS) were non-significantly better in the translational than in patients not included in the translational BECOX trial. Data are summarized in Table 2.
Differences between treatment compliance and efficacy outcomes between patients analyzed and not analyzed in the translational trial.
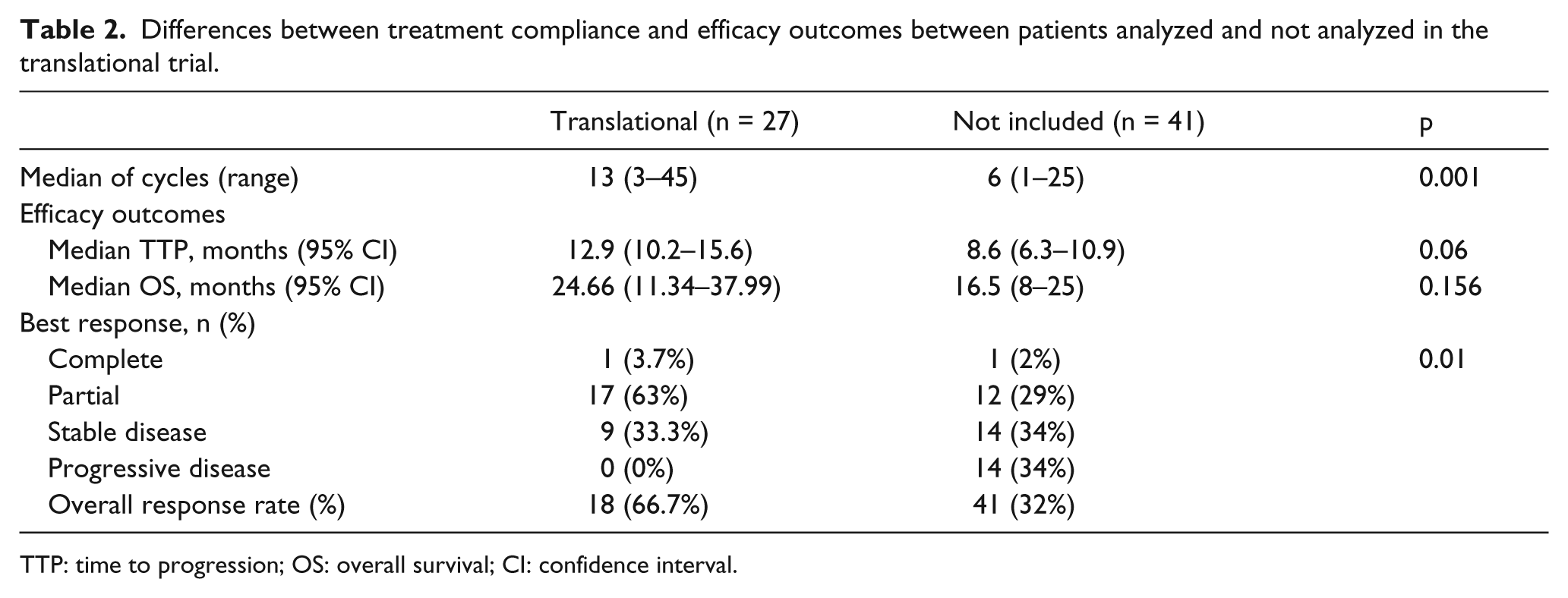
TTP: time to progression; OS: overall survival; CI: confidence interval.
Median basal levels of VEGF-A165, sVEGFR1, and HGF were 664 pg/mL (36–1450), 195 pg/mL (115–837), and 2157 pg/mL (815–4336), respectively. VEGF-A165, sVEGFR1, and HGF basal levels did not correlate with efficacy outcomes. As described previously, VEGF-A levels decrease after treatment with bevacizumab independent of response. HGF serum levels initially increase in responders and decrease in non-responders, but during treatment serum HGF levels also decrease progressively in responders initially (see Figure 2).

Averaged evolution of VEGF-A, sVEGFR1, ratio sVEGFR1/VEGF-A, HGF, and ratio HGF/VEGF-A. Averaged evolution of VEGF, sVEGFR1, and HGF having achieved a Partial response (labeled blue) at any time during follow-up.
We found that responders had a 3.22-fold (by IA) and a 3.06-fold (by IR) increase in the ratio of sVEGFR1/VEGF-A from previous determination compared with a 1.38-fold (IA) and a 1.59-fold (IR) increase in non-responders (p = 0.0009 and 0.03, respectively). Moreover, responders had a 3.36-fold (IA) and a 3.66-fold (IR) increase in the ratio of HGF/VEGF-A compared with a 1.43-fold (IA) and 1.53-fold (IR) increase for non-responders (p = 0.002 and 0.003, respectively; see Table 3 and Figure 3).
Fold change in sVEGFR1/VEGF and HGF/VEGF ratios from previous cycle by type of response achieved.

IA: investigator assessment; IR: independent radiologist; VEGF: vascular endothelial growth factor; sVEGFR1: soluble VEGF receptor 1; HGF: hepatocyte growth factor.

Fold change in sVEGFR1/VEGF and HGF/VEGF ratios from previous cycle by type of response achieved (cycle 0: non-responders; cycle 1: responders).
Discussion
Our main finding is that the decrease in VEGF-A and an increase in sVEGFR1 during chemotherapy and bevacizumab exposure can contribute to both chemotherapy (due to MET/b-catenin activation) and bevacizumab (due to low VEGF requirements) resistance. In our study, we have confirmed clinically our previous pre-clinical observation 12 that a significant increase in the ratio of sVEGFR1/VEGF-A can predict response to bevacizumab–chemotherapy combination. This is the first work that analyzes changes in the ratios of serum biomarkers in a dynamic manner and the correlation with radiologic assessments. Because HGF levels decrease also during intrinsic and acquired resistance, alternative strategies to overcome MET/B-catenin activation should be implemented.
Previously, we have described that chemoresistant CRC cells in vitro upregulate sVEGFR1 and phosphorylate MET. 12 Because MET can be activated also in mCRC patients with low sVEGFR/VEGF-A and not only through HGF, our study suggests that in selected refractory mCRC patients (those with low sVEGFR1/VEGF-A ratio), monoclonal antibodies against MET such as onartuzumab 14 would be probably less effective than MET tyrosine kinase inhibitors (TKIs) such as cabozantinib. 15
We are aware of the limitations of our study. First, only one-third of patients in the BECOX trial were analyzed in the translational study. Second, patients included in the translational study constitute a biased selection population with better treatment response because none of the patients with progressive disease participated in the translational study. Finally, we cannot distinguish chemotherapy effects from anti-VEGF effects because all patients are treated with chemotherapy and bevacizumab. Strengths of our study are the intrinsic prospective nature and the novel dynamic analyses, not previously described, that confirms our pre-clinical findings.
In conclusion, our translational study reflects that the serum dynamic biomarker would allow to switch in selected bevacizumab-refractory mCRC patients to other therapies such as MET TKIs. This strategy deserves merits in a prospective biomarker-selected mCRC bevacizumab-refractory patients in a phase II study.
Conclusion
In summary, a decrease in VEGF-A and an increase in sVEGFR1 during chemotherapy and bevacizumab exposure can contribute to both chemotherapy (due to c-MET/b-catenin activation) and bevacizumab (due to low VEGF requirements) resistance. Because HGF levels decrease also during acquired resistance, alternative strategies to HGF-ligand inhibition should be investigated.
Footnotes
Acknowledgements
This study was presented in part in the European Cancer Congress, 2015, Vienna and in the ASCO Annual Meeting, 2015, Chicago. The authors thank Dr Cristobal Mezquita, Departament de Ciències Fisiològiques de la Facultat de Medicina, Universitat de Barcelona.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “beca SEOM a Jóvenes Investigadores 2009” and by the Emili Letang fellowship to Estela Pineda.