
Abstract
Objective:
Tissue inhibitor of metalloproteinases 1 (TIMP-1) and matrix metalloproteinase 7 (MMP-7) were reported to have potent growth promoting activity. Lack of balance between MMPs and TIMPs is an important factor in the development of gastrointestinal malignancies.
Methods:
We collected serum samples from 97 patients with metastatic colorectal cancer and 79 samples from healthy controls. Serum levels of TIMP-1 and MMP-7 were measured immunochemically and compared with standard tumor markers carcinoembryonic antigen and CA19-9.
Results:
Serum levels of TIMP-1 and MMP-7 were significantly higher in patients with colorectal cancer compared to healthy controls (both, P < 0.001). TIMP-1 and MMP-7 correlate with the presence of colon involvement (P = 0.001; P = 0.012) and the presence of liver metastases (P = 0.002; P = 0.037), and negatively correlate with pulmonary metastases (P = 0.014; P = 0.005). MMP-7 had similar sensitivity and the same specificity as carcinoembryonic antigen. TIMP-1 and MMP-7 had better sensitivity than CA19-9. TIMP-1 and MMP-7 level correlate with worse outcome (P = 0.002).
Conclusion:
The results indicate that TIMP-1 and MMP-7 are effective biomarkers in patients with metastatic colorectal cancer with good sensitivity. TIMP-1 and MMP-7 levels strongly correlate with the extent of liver disease and have prognostic value.
Introduction
Colorectal cancer (CRC) is the second leading tumor diagnosis in women and in men in the Czech Republic 1 and is the third most common cancer in men (10.0% of the total) and the second in women (9.2% of the total) worldwide. 2 Early detection of metastatic liver disease is an important indication for liver surgery. Therefore, novel biomarkers for earlier cancer detection and early detection of metastatic disease are strongly needed.
Tissue inhibitors of metalloproteinases (TIMP-1, TIMP-2, TIMP-3, and TIMP-4) are recognized as a family of intrinsic inhibitors of matrix metalloproteinases (MMPs).3–4 Their ability to inhibit MMPs suggests that they play an important role in the regulation of MMP activity, effectively controlling the breakdown of extracellular matrix components involved in various kinds of important biological phenomena and pathological events, such as inflammation and tumor invasion.5–7 In addition, TIMP-1 and TIMP-2 were reported to have potent growth-promoting activity for a wide range of cells, and previously unrecognized cell-growth factors in serum.3,8–9 Lack of balance between MMPs and TIMPs is an important factor in the development of gastrointestinal malignancies. 10 An increased plasma level of TIMP-1 was a significant prognostic factor for the survival of patients with CRC.11–13 Elevated concentrations of this protein were detected in patients with CRC.14–15
MMPs comprise a family of zinc-dependent endopeptidases involved in the tumor invasion of surrounding tissue plus metastatic formation and evasion of the immune system. 16 Their ability to degrade the extracellular matrix components and even non-matrix proteins helps tumor invasion and metastatic spread.17–18 Upregulation of several MMPs including MMP7, MMP10, and MMP12 in cancerous tissue. Their secretion into the blood stream and adverse association with survival has been evaluated in CRC.19–22 MMP-7 has a broad proteolytic activity against a variety of extracellular matrix substrates, including collagens, proteoglycans, elastin, laminin, fibronectin, and casein.22–24 It is produced by malignant tumor cells including prostate, gastric, head and neck, lung, hepatocellular, and colorectal carcinomas.25–28 It is noteworthy that only MMP-7 is produced by CRC cells themselves, whereas the other MMPs are secreted by stromal cells.25, 27
In this study, we investigated the serum levels of TIMP-1 and MMP-7 in patients with metastatic CRC compared to healthy controls. This is the first study with complex information regarding clinico-pathological correlation and survival compared to standard biomarkers used in CRC (carcinoembryonic antigen (CEA) and CA19-9).
Material and methods
Patients and healthy control characteristics
Between November 2011 and May 2013, 97 patients with metastatic CRC at the time of distant metastasis diagnosis or during progression validated by computed tomography (CT), and 79 relatively age- and gender-matched healthy individuals, were included in this study at the Department of Oncology of the First Faculty of Medicine, Charles University and General Teaching Hospital in Prague. All patients had a histologically proven diagnosis of colorectal adenocarcinoma with distant metastases, adequate liver and renal function (transaminases < 2× and creatinine clearance < 1.5× upper normal limit), and signed informed consent. Serum samples from 58 patients were collected 3 months after the first one together with imaging control using response evaluation criteria in solid tumors (RECIST) 1.1 criteria. Healthy individuals signed informed consents, underwent healthy examinations and had negative colonoscopies.
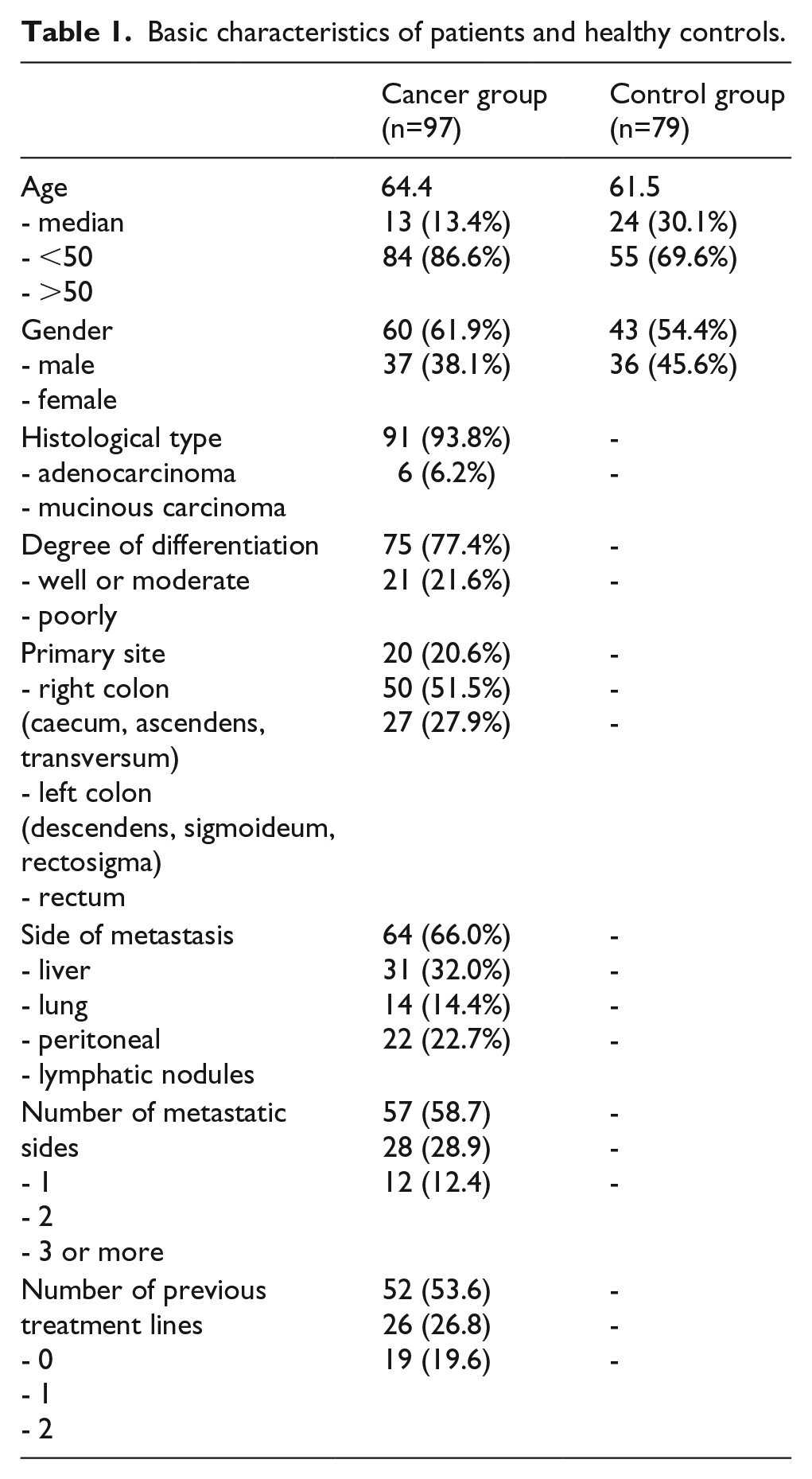
The majority of patients were included after resection of primary tumor (79.4%). Metastases were liver in 64 cases (66.0%), lung (31; 32.0%), peritoneal (14; 14.4%) and lymphatic nodules (22; 22.7%). The patient characteristics are described in Table 1. In the cancer group, the serum level of CEA was 308.3 ± 84.9 ug/L and CA19-9 and was 948.1 ± 307.0 kIU/L. Both markers were significantly elevated compared to the control group (P = 0.001; P = 0.006, respectively). 29
Basic characteristics of patients and healthy controls.
Laboratory methods
Blood for laboratory analyses was collected after overnight fasting via puncture of the cubital vein. Routine biochemical parameters were measured in fresh samples. For special parameters, blood was centrifuged for 10 min at 3000 rpm (rotations per minute) and serum was stored at −80 °C until analysis. Levels of TIMP-1 (Thermo Fisher Scientific, Waltham, MA, USA) and MMP-7 (R&D Systems, Minneapolis, MN, USA) in serum samples were determined by commercially available ELISA (enzyme linked immunoassay) kits according to the manufacturer’s protocols.
Statistical analysis
Statistical analysis was performed using SAS (SAS Institute Inc., Cary, NC, USA). Basic statistics were calculated for parameters measured in the whole group and in different subgroups, such as mean, standard deviation, variance, and median. Non-parametric analysis of variance two-sided Wilcoxon test was used for comparison of the distribution of the individual parameters in the different groups and subgroups. Due to non-Gaussian distribution of variables Spearman’s correlation coefficient was used to determine the dependency of characters. Statistical significance was determined at the border of alpha = 0.05. Receiver operating characteristic (ROC) curves were generated to assess the diagnostic accuracy of each parameter; the sensitivity and specificity of the optimum cutoff point were found. Survival data were graphically processed by Kaplan–Meier curves and these curves were compared by the log-rank test.
Results
Baseline characteristic of patients and controls
In the cancer group, serum samples from 97 patients with generalized CRC were collected (38.1% women; median age 64.4 years), and from 58 patients we obtained the second serum sample 3 months after the first. In the control group, 79 healthy volunteers were included after negative colonoscopy (45.6% women; median age 61.5 years).
Serum levels of TIMP-1 and MMP-7
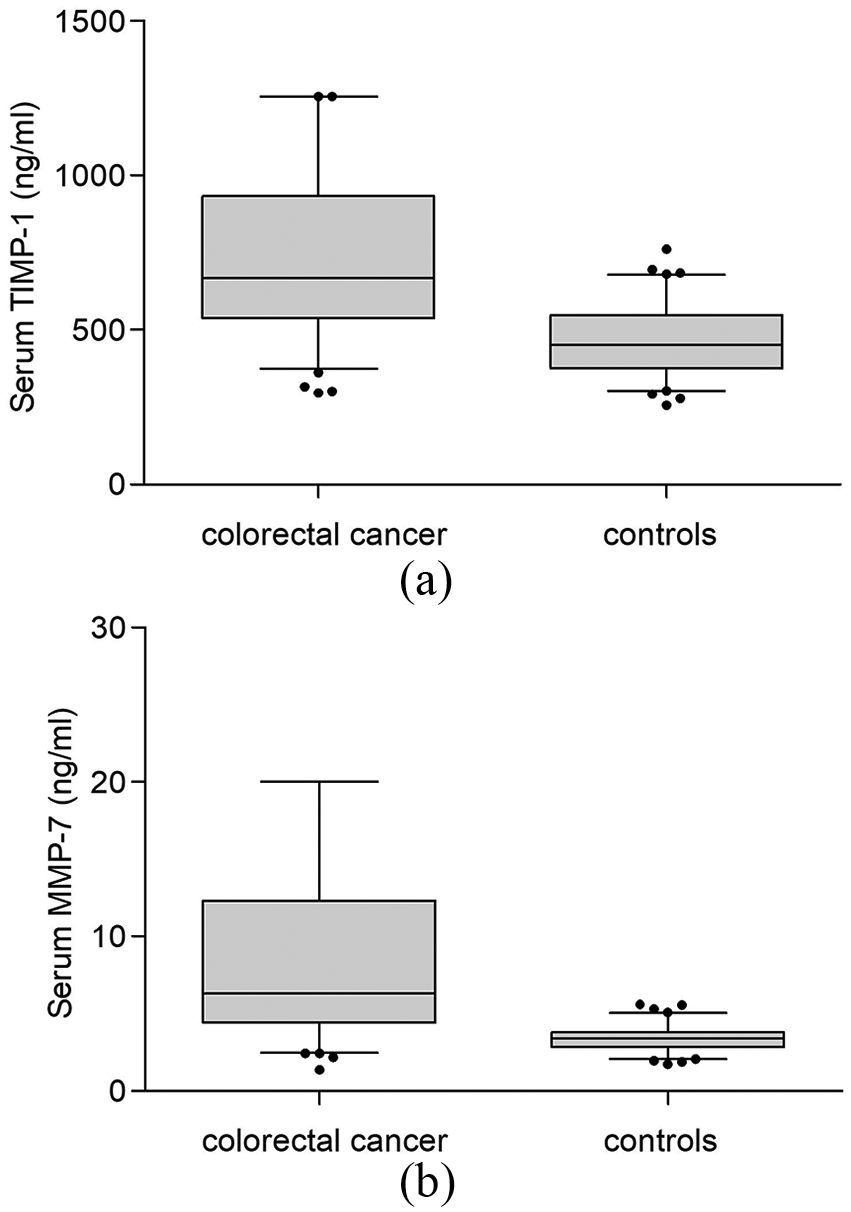
Serum level of TIMP-1 in the cancer group was significantly increased compared to healthy controls (750.4 ± 29.6 ng/mL and 463.9 ± 12.2 ng/mL, respectively, P < 0.001, Figure 1(a)). In the control group there was no significant difference in TIMP-1 level between men and women (P = 0.205), similarly in younger than or equal to 55 years and older than 55 (P = 0.806).
The comparison of TFF, CEA, and CA19-9 levels in patients with colorectal cancer and healthy controls.
There was no significant difference in serum level of TIMP-1 between sex, age, part of colon with primary tumor and tumor grade (Table 2). Patients with non-resected primary tumor (n=20) had statistically significantly higher TIMP-1 levels 957.1 ± 63.8 ng/mL than patients after resection (n=77) with 697.1 ± 30. 8 ng/mL (P = 0.001). Association was recognized between patients with and without liver metastases (817.3 ± 38.4 ng/mL, n=64; 621.4 ± 35.9 ng/mL, n=33; P = 0.002). Negative association was identified between patients with and without pulmonary metastases (649.9 ± 50.0 ng/mL, n=31; 797.6 ± 36.7 ng/mL, n=66; P = 0.014). The group of patients with liver metastases without pulmonary metastases was divided into patients with the sum of the longest dimension of liver metastases smaller than 100 mm (n = 20) and larger than or equal to 100 mm (n = 29). The difference in TIMP-1 levels was statistically significant (P < 0.001), 658.9 ± 50.4 ng/mL and 977.0 ± 51.8 ng/mL, respectively (Figure 2(a)).
Serum TIMP-1 and MMP-7 levels in different subgroups.
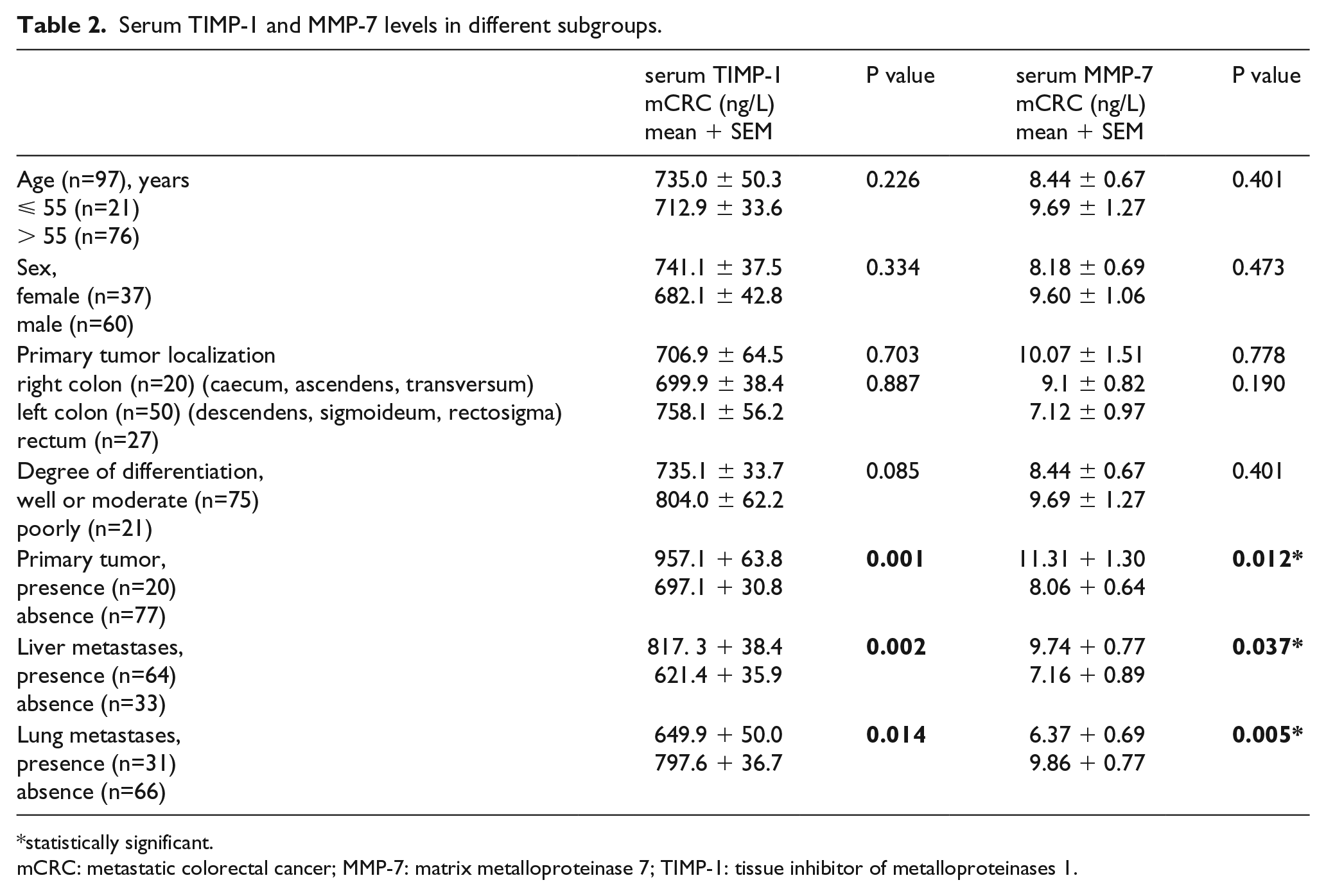
statistically significant.
mCRC: metastatic colorectal cancer; MMP-7: matrix metalloproteinase 7; TIMP-1: tissue inhibitor of metalloproteinases 1.
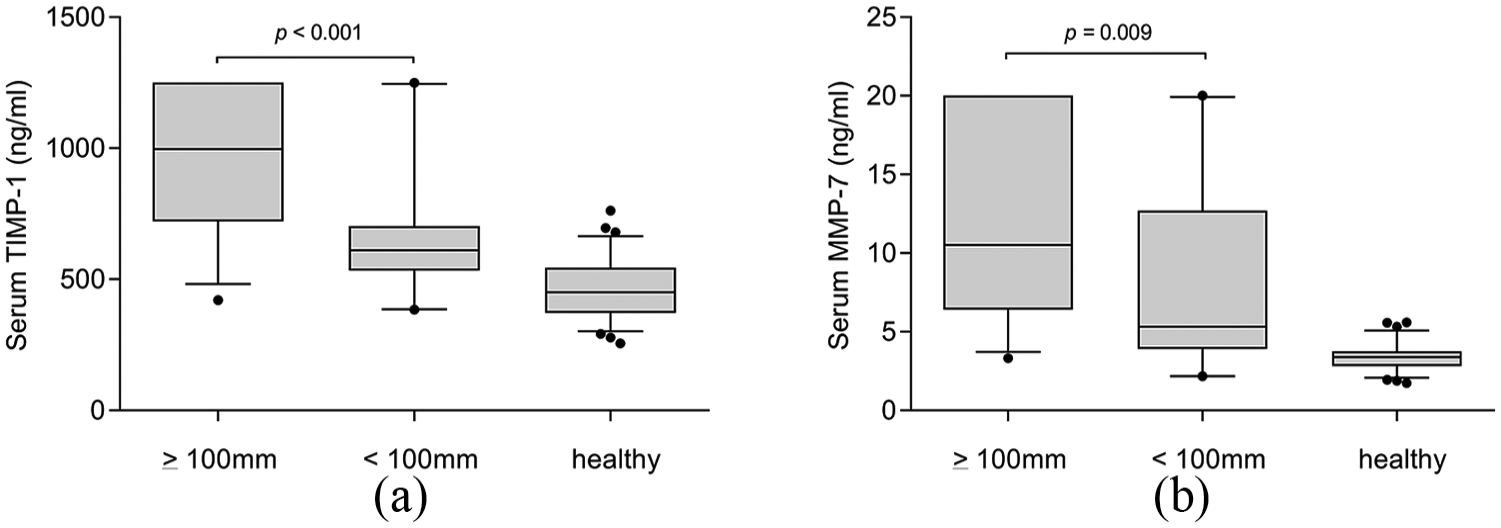
The serum levels of TIMP-1 and MMP-7 in patients without pulmonary metastasis and with the presence of liver metastasis.
Serum level of MMP-7 in the cancer group was 8.72 ± 0.60 ng/mL and was significantly elevated compared to 3.38 ± 0.09 ng/mL in the healthy control group (Figure 1(b), P < 0.0001). In the control group there was no significant difference in MMP-7 level between men and women (P = 0.556) and in younger than or equal to 55 years and older than 55 years (P = 0.741).
In the cancer group there was no significant difference between sex, age, part of colon with primary tumor, and tumor grade (Table 2). There was a significant difference in the presence or absence of the primary tumor, 11.31 ± 1.30 ng/mL (n = 20) and 8.06 ± 0.64 ng/mL (n = 77), respectively (P = 0.012). A statistically significant difference was found between patients with and without liver metastases (9.74 ± 0.77 ng/mL, n=64; 7.16 ± 0.89 ng/mL, n=33; P = 0.037). Negative association was identified between patients with and without pulmonary metastases (6.37 ± 0.69 ng/L, n=31; 9.86 ± 0.77 ng/mL, n=66; P = 0.005). There was an indicated difference in pulmonary negative tumors with the presence (11.69 ± 1.33 ng/mL, n=17) or absence of primary tumor or local relapse (8.73 ± 0.92 ng/ml, n=36; P = 0.036). The group of patients with liver metastases without pulmonary metastases with the sum of the longest dimension of liver metastases smaller than 100 mm (n = 20) compared to larger than or equal 100 mm (n = 29) has a statistically significant difference in MMP-7 levels (8.07 ± 1.33 ng/mL and 11.95 ± 1.12 ng/mL, respectively; P = 0.009; Figure 2(b)).
Sensitivity and specificity of TIMP-1 and MMP-7
ROC curve analysis showed that serum TIMP-1 with an area under the curve (AUC) of 0.820 (Figure 3(a)) and a serum level cutoff of 600.0 ng/mL has the sensitivity and specificity to distinguish CRC from healthy controls are 50.5 % and 93.8%, respectively (P < 0.001). MMP-7 with an AUC of 0.873 (Figure 3(b)) and serum level cutoff values 4.9 ng/mL has the sensitivity and specificity of 69.1% and 93.8%, respectively (P < 0.001).
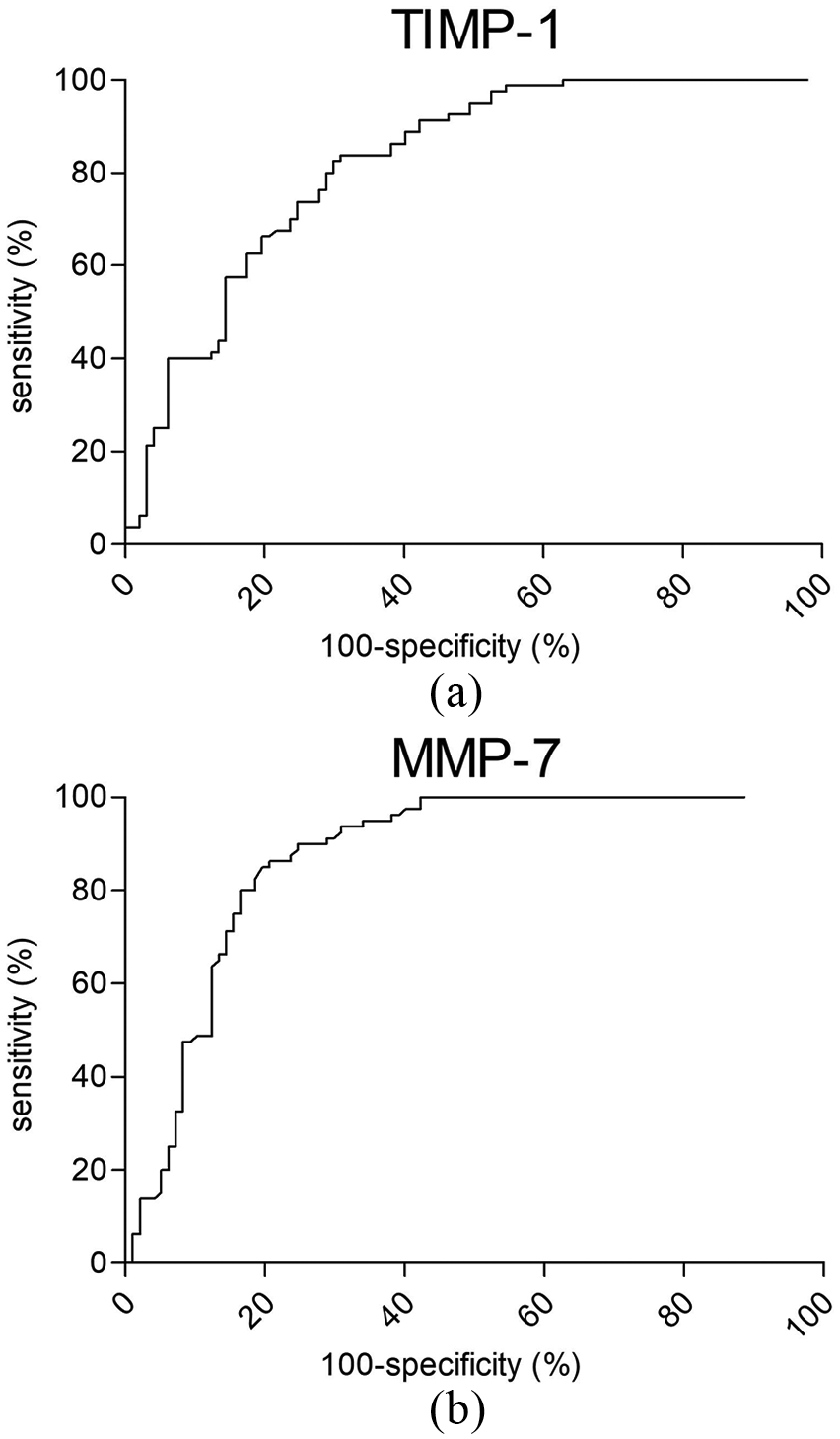
ROC curve analysis of TIMP-1 and MMP-7.
Change in levels of TIMP-1 and MMP-7 during therapy
Serum samples from 58 patients were collected 3 months after first one, together with imaging control using RECIST 1.1 criteria. The samples were divided into three groups according to imaging control (with partial remission, stable disease, and progressing disease). In the group with partial remission on CT scans (n = 15) TIMP-1 levels decreased in nearly all patients (Figure 4(a), mean decrease of level between first and second sample collected 3 months later was 179.0 ng/mL; P = 0.010). In the group of patients with stable disease on CT scans (n = 22) no statistically significant decrease in TIMP-1 levels was observed (Figure 4(b), mean decrease 63.1 ng/mL; P = 0.379). In the last group with progression of disease on CT scans (n = 21) TIMP-1 levels increased, but the difference was not statistically significant (Figure 4(c); mean increase 73.7 ng/mL; P = 0.393).
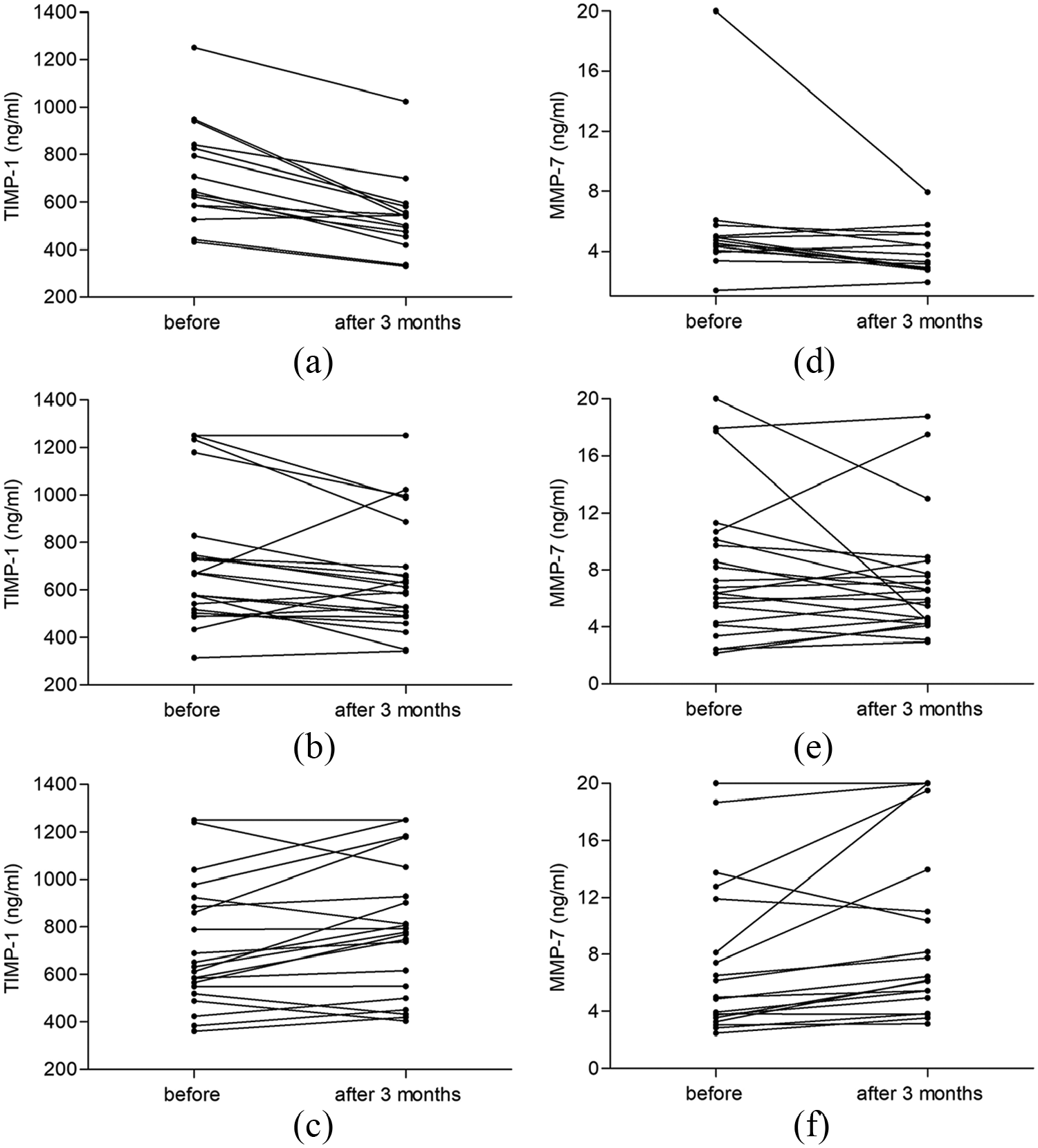
Change of TIMP-1 and MMP-7 levels after 3 months of therapy according to CT scans (RECIST 1.1).
Similarly, in the group of patients with partial remission MMP-7 levels decreased, but not with statistical significance (Figure 4(d), mean decrease 1.4 ng/mL; P = 0.234). No statistically significant change was observed in the group of patients with stable disease (Figure 4(e), mean decrease 0.8 ng/mL; P = 0.551) and in the group with progression of disease (Figure 4(f), mean increase 1.9 ng/mL; P = 0.340).
The level of TIMP-1 and MMP-7 as a prognostic factor
The serum level of TIMP-1 appears to have a prognostic value. The cutoff for serum TIMP-1 level was determined as 600.0 ng/mL. Patients were divided into the group with negative serum levels of TIMP-1 (⩽ 600.0 ng/mL, n=39), slight increase (> 600.0 and ⩽ 1200.0 ng/mL, n=40) and large increase (> 1200.0 ng/mL, n=18). From all 58 patients, overall survival (OS, time from first sample collection to death) was calculated. No significant difference (P = 0.245) between the group with negative TIMP-1 levels (mOS 18.8 months) and the group with slight increase (mOS 12.3 months) was observed. But there was statistically significant difference between these two groups and the group with a large increase in TIMP-1 serum level (mOS 4.4 months; P < 0.001 and P = 0.001, respectively; Figure 5A).
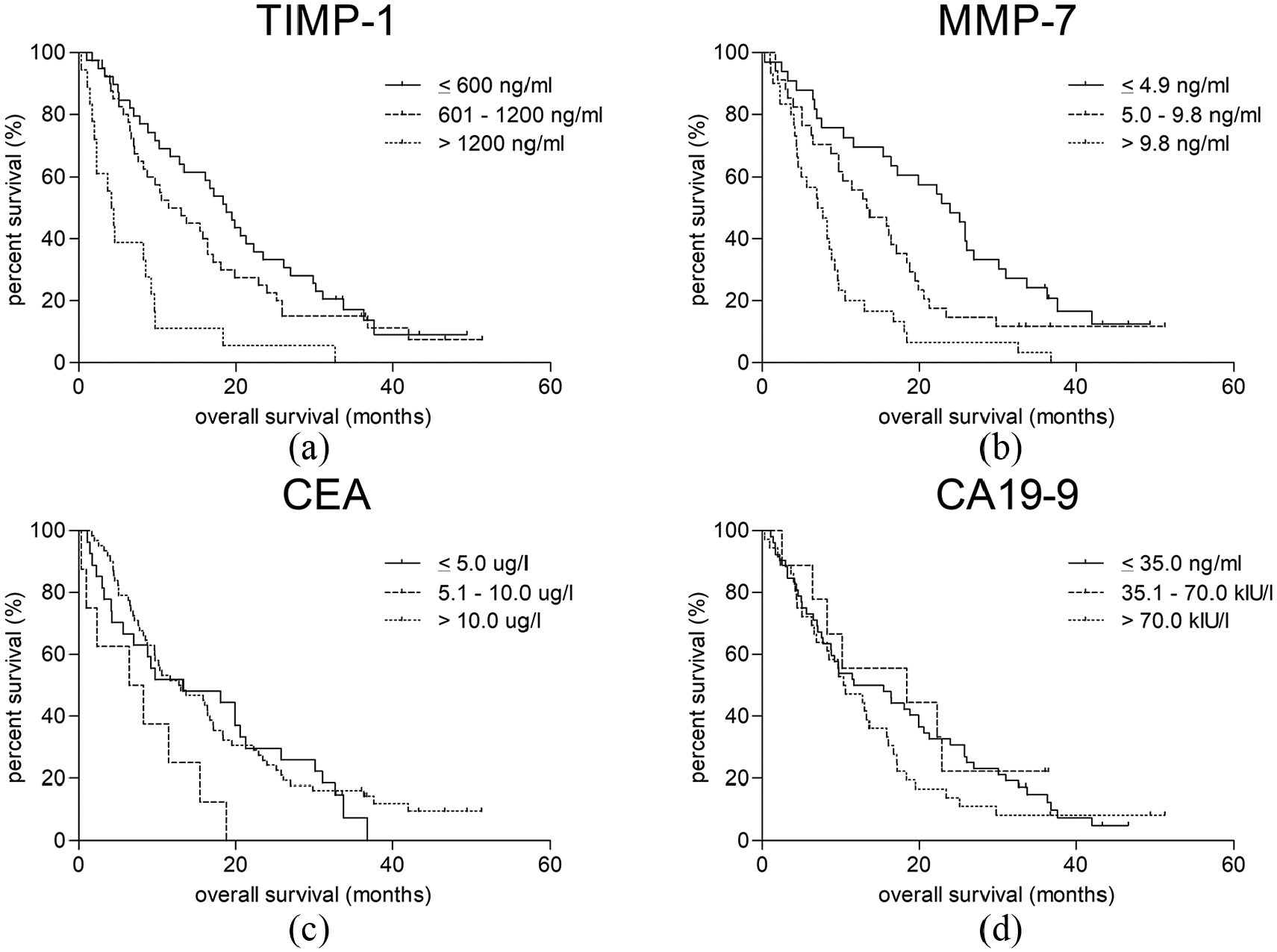
Overall survival according to TIMP-1 and MMP-7 levels.
Similarly, the serum level of MMP-7 appears to have a prognostic value, too. Patients were divided into a group with negative serum levels of MMP-7 (⩽ 4.9 ng/mL, n=33), a slight increase (5.0 and ⩽ 9.8 ng/mL, n=34), and a large increase (> 9.8 ng/mL, n=30). There was a statistically significant difference between the group with negative MMP-7 levels (mOS 24.0 months) and the group with a slight increase (mOS 13.6 months; P = 0.032), and between these two groups and the group with a large increase of MMP-7 serum level (mOS 7.5 months; P < 0.001 and P = 0.006, respectively; Figure 5(b)).
We tried the same with CEA and CA19-9, but there was no significant difference found (Figure 5(c) and (d)). The OS of patients with a negative serum level of CEA (⩽ 5.0 ug/L) did not differ from patients with a slight increase (5.0 and ⩽ 10.0 ug/mL; P = 0.128) and a high increase (> 10.0 ng/mL, P = 0.701). Similar results were found in patients with a negative serum level of CA19-9 (⩽ 35.0 kIU/l). The results did not differ from patients with a slight increase (35.0 and ⩽ 70.0 kIU/l; P = 0.634) and a high increase (> 70.0 kIU/l, P = 0.257).
Further, we used univariate Cox analysis to confirm the effect of entry serum levels of TIMP-1, MMP-7, CEA, and CA19-9 on OS (Table 3). While the entry levels of CEA and CA19-9 did not show any significant correlation with survival, the higher entry serum levels of TIMP-1 and MMP-7 were associated with worsened survival (hazard ratio (HR) 1.65, P = 0.024; and HR 1.94, P = 0.005, respectively).
Univariate Cox analysis of the effect of entry serum levels of TIMP-1, MMP-7, CEA, and CA19-9 on overall survival.
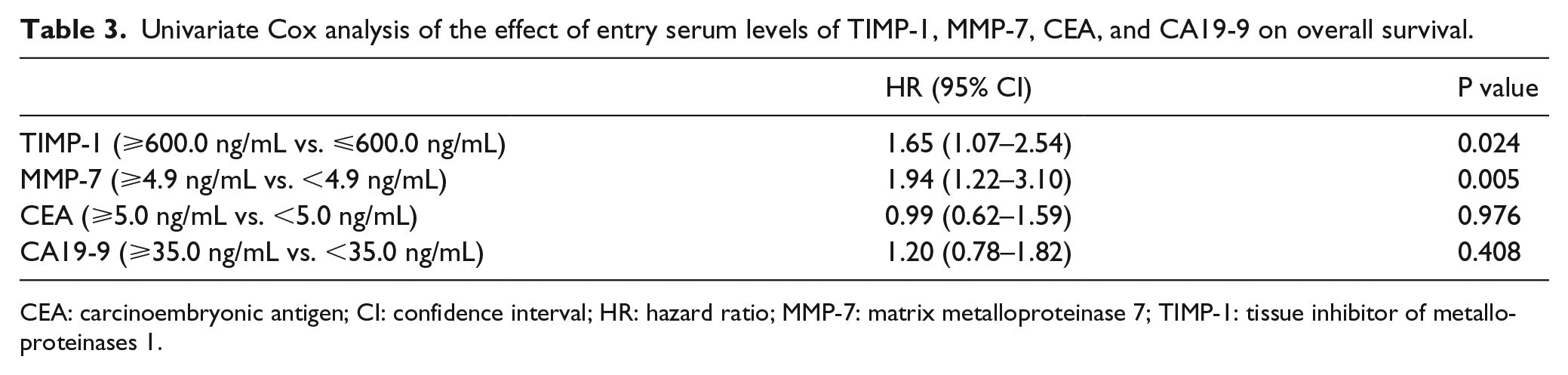
CEA: carcinoembryonic antigen; CI: confidence interval; HR: hazard ratio; MMP-7: matrix metalloproteinase 7; TIMP-1: tissue inhibitor of metalloproteinases 1.
Based on these observations, we compared the survival of patients with negative levels of TIMP-1 (< 600.0 ng/mL) and MMP-7 (< 4.9 ng/mL; n=17) with patients whose entry serum levels of TIMP-1 and MMP-7 was high (> 1200.0 ng/mL, > 9.8 ng/mL, respectively; n=15). The OS difference was statistically significant (26.1 vs. 4.6 months; HR = 0.25, 95% CI 0.11, 0.59; P = 0.002).
Discussion
Early diagnosis is crucial for the successful treatment of CRC. In the patients with metachronous distant metastases previously treated for local disease, early diagnosis is important for possible radical resection. In clinical practice new biological markers for early detection of CRC are urgently needed.
TIMP-1, an intrinsic inhibitor of matrix metalloproteinases, was reported to have potent growth-promoting activity for a wide range of cells. Higher serum or plasma levels were described in patients with localized CRC by Nielsen et al. 30 and their impact on survival of patients. Birgisson et al. 31 reported the impact of entry level of TIMP-1 on prognosis (HR 1.8; 95% CI 1.3, 2.4) and no association of CEA levels with prognosis. Holten-Andersen et al. 32 showed a correlation of pre- and postoperative plasma levels of TIMP-1 with poor prognosis in patients with resectable CRC. In contrast, Ishida et al. 15 reported no correlation of TIMP-1 level and prognosis. Frederiksen et al. 33 and Sørensen et al. 34 published worse prognosis with a higher plasma level of TIMP-1 at the beginning of treatment in patients with metastatic CRC (HR 1.80, P = 0.008; and HR 3.80, P < 0.001, respectively).
MMP-7 is produced by CRC cells themselves. 25 In a meta-analysis published by Sun and colleagues, 35 higher expression of MMP-7 in tumor tissue was connected with the poor prognosis of these patients. Klupp et al. 22 and Maurel et al. 36 published difference between serum levels in patients with localized and metastatic CRC. Three other studies describe only prognostic value of serum MMP-7 levels (two in localized CRC before surgery and one in metastatic CRC).37–39 Studies presenting serum levels of TIMP-1 and MMP-7 in stage IV patients were published without sufficient information about level difference between metastatic side, extent of metastatic side involvement, and direct comparison to CEA and CA19-9.
The TIMP-1 and MMP-7 levels were significantly higher in patients compared to controls. Serum levels of both markers correlated with colon or rectum involvement (non-resected primary tumor or local recurrence) with liver involvement, and negatively with pulmonary involvement. In addition, TIMP-1 and MMP-7 correlated with the extent of liver involvement in cases without pulmonary metastases. This finding is very interesting because these patients could be candidates for a radical resection of liver metastases, the only modality than can completely cure them.
The MMP-7 has slightly lower sensitivity (sensitivity and specificity of 69.1% and 93.8%, respectively) than CEA (72.16% and 97.47%, respectively, as in our previous study). 29 TIMP-1 level correlate with tumor response controlled by CT scans (RECIST 1.1). These results suggested that serum TIMP-1 may be a useful potential marker of response to chemotherapy.
The entry level of TIMP-1 appears to be a prognostic factor that strongly correlates with OS. This can be partially explained by a strong correlation of TIMP-1 level with liver involvement in patients without pulmonary metastases. The patients with a sum of liver metastases larger than 100 mm had significantly higher levels of TIMP-1 and their liver reserve was smaller. Another partial explanation could be that patients with a non-resected primary tumor, who have higher levels of TIMP-1, were not operated on because of their worse performance status. This may be the reason for a worse outcome of the treatment. Similar results have been reported before, but were not so complex.38,39
In the univariate Cox analysis, the higher serum levels of MMP-7 were associated with poor prognosis of patients (HR 1.948; 95% CI 1.22, 3.10; P=0.005). Our data are similar to that previously reported by Maurel et al. 36 MMP-7 (as a continuous variable) was associated with decreased survival (HR 1.016, 95% CI 1.002, 1.031). The same results were published by Garcia-Albeniz et al. 39 in metastatic CRC patients. They found a correlation between the level of MMP-7 and survival (HR 1.03, P=0.029).
We tried to find similar correlation of CEA or CA19-9 serum level and patient survival, but no significant difference was observed. Further investigation and data are needed to clarify these results.
In summary, our data indicated that serum TIMP-1 together with MMP-7 can be used as effective tumor markers for the detection of metastatic CRC. Our data have shown that decreased serum TIMP-1 levels significantly correlate with response to chemotherapy in the group of patients with partial regression, and are not significantly correlated with the group with disease progression. TIMP-1 and MMP-7 correlate with the extent of liver involvement in patients, and the entry levels of them appear to be a prognostic factor that correlates with OS.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by research projects Progres Q28/LF1, BBMRI-CZ II LM2015089 and MH CZ DRO VFN 64165.