
Abstract
Background
Hepatocellular carcinoma (HCC) is the most common primary liver neoplasia. Vascular endothelial factor receptor 2 (VEGFR-2) plays an important role in angiogenesis and it has been associated with poor survival in certain other tumor types. Although a recent study also suggested an association between VEGFR-2 expression and HCC, the relationship between VEGFR-2 amplification and HCC is still obscure.
Aim
To evaluate prognostic role of vascular endothelial growth factor receptor 2 (VEGFR-2) amplification in relation to serum alpha-fetoprotein (AFP) levels and tumor clinicopathological parameters among liver-transplanted patients with HCC.
Study design
Cohort study
Methods
A total of 54 formalin-fixed paraffin-embedded and frozen HCC samples from patients who underwent liver transplantation between 2009 and 2015 were analyzed. VEGFR-2 amplification was determined via fluorescence in situ hybridization (FISH) method in tissue samples obtained during liver transplantation and analyzed with respect to serum AFP levels, tumor clinicopathological parameters, and oncological outcomes including recurrence free survival (RFS) and overall survival (OS).
Results
Amplified VEGFR-2 gene was prominent in 27 (50.0%) patients, while AFP levels were ≥100 ng/mL in 14 (25.9%) patients. Presence of amplified VEGFR-2 gene was associated with significantly shorter RFS time (mean 72.8 vs 101.3 months for positive and negative patients respectively, P = .015), whereas had no significant impact on OS time (median 79.2 vs 93.1 months, respectively, P = .206). Presence versus absence of amplified VEGFR-2 gene was associated with significantly higher levels of AFP (mean±SD 266.6±405.8 vs 40.6±94.6 ng/mL, P = .016) and higher recurrence rate (81.8 vs 18.2%, P = .018), and significantly predicted the AFP levels ≥100 ng/ml (OR, 10.2, 95%CI 1.8-56.9, P = .008). Lymphatic invasion and vascular invasion emerged as independent predictors of poor OS (HR, 12.4 [95% CI, 2.7-57.3], P = .01) and RFS (HR, 8.3 [95% CI, 2.3-29.8], P = .01).
Conclusion
In conclusion, our findings revealed the presence of amplified VEGFR-2 gene and its association with serum AFP elevation for the first time in HCC. VEGFR-2 amplification was associated with significantly shorter RFS and it emerged as a significant predictor of elevated AFP. Accordingly, our findings seem to indicate the role of AFP elevation in VEGFR-2-mediated tumorigenesis as well as the likelihood of amplified VEGFR-2 gene and high AFP levels to determine the risk status and efficacy of VEGFR-2-inhibitors in HCC liver transplanted patients.
Keywords
Introduction
Liver cancer ranks the sixth in incidence and the fourth in mortality among all cancers globally. 1 Hepatocellular carcinoma (HCC) comprises the majority of primary liver cancers, as associated with risk factors including hepatitis B virus and hepatitis C virus infection and cirrhosis of any etiology. 2
Current treatment options in HCC include hepatic resection, transplantation, ablation, and trans-arterial chemoembolization as well as tyrosine-kinase inhibitors (TKIs) such as sorafenib, lenvatinib, and regorafenib, which are mainly used for the advanced disease.3-9 In early-stage HCC, liver transplantation is the best treatment modality associated with the highest likelihood of cure, also offering a potential treatment for the underlying cirrhosis. 10
Vascular endothelial growth factor (VEGF) harbors 3 tyrosine kinase receptors, namely the VEGF receptor 1, VEGF receptor 2 (VEGFR-2), and VEGF receptor 3. VEGFR-2 is a major regulator of angiogenesis and is encoded by the KDR gene (located at 4q12) in HCC.11-13 The blockage of VEGFR-2 is considered a promising strategy to inhibit tumor-induced angiogenesis to provide cancer patients maximal survival benefit.14, 15 HCC lesions are characterized by arterial hyper-vascularity, in which angiogenesis plays an important role. 16 Knockdown of VEGFR-A 165 expression inhibits the proliferation, migration, survival, and adhesion ability of HCC cell culture. 17 SHARP study was the first study to show the potential role of VEGFR inhibition, albeit with limited survival benefit, in HCC treatment. 8
However, given the discouraging results obtained in preclinical studies with VEGFR inhibitor treatments indicating a limited survival benefit with rapid revascularization and more invasive and metastatic behavior of cancers after the initial suppression of tumor vasculature and tumor growth,18-20 the need for further investigation of the mechanisms involved in VEGF-mediated regulation of tumor angiogenesis and to develop novel strategies to enhance efficacy of VEGFR inhibitors with MET inhibitor has been emphasized. 17
Indeed, the high expression of VEGFR-2 by HCC tumor cells was reported via real-time polymerase chain reaction, western blotting and immunohistochemistry and shown to be associated with poor prognosis.21, 22 However, despite the likelihood of gene overexpression and gene amplification to have differential prognostic roles, no genomic study to date have provided data on VEGFR-2 amplification as well as its prognostic value in liver-transplanted HCC patients. 23 Only one immunochemical study in transplanted patients indicated a high expression of VEGFR-2 in cirrhotic liver tissue but not in the tumor tissue. 22
In addition, while a link between VEGFR overexpression and increased concentrations of alpha-fetoprotein (AFP) has previously been described, the relationship between VEGFR-2 amplification and AFP is unclear.21, 24 This seems notable given that a high-level gene amplification of a TKI receptor gene such as VEGFR-2 has been considered likely to serve as a biomarker for TKI inhibitor therapy. 25
This study was therefore designed to evaluate VEGFR-2 gene amplification in HCC tumor samples obtained during liver transplantation, using the gold standard FISH method, and to evaluate the potential prognostic role of amplified VEGFR-2 gene in relation to serum AFP levels, tumor clinicopathological parameters, and oncological outcome.
Materials and Methods
Tissue Samples
A total of 54 formalin-fixed paraffin-embedded and frozen HCC samples from patients who underwent hepatic transplantation between 2009 and 2015 were obtained from Pathology Department. Mixed tumors with coexisting intrahepatic cholangiocarcinoma were excluded.
The study was conducted in accordance with the ethical principles stated in the “Declaration of Helsinki.”
Assessments
Data on patient demographics (age, gender), primary etiology, tumor clinicopathological parameters (tumor stage, tumor grade, tumor diameter, microvascular invasion, lymphatic invasion, vascular invasion, portal vein invasion, hepatic vein invasion, bile duct invasion and positive surgical margin) and serum level of AFP (ng/mL) as well as follow-up data on recurrence-free survival (RFS) and overall survival (OS) were retrieved from the hospital records. All tumors were classified according to the WHO classification system. VEGFR-2 amplification in tumor samples was analyzed using FISH technique.
FISH Technique
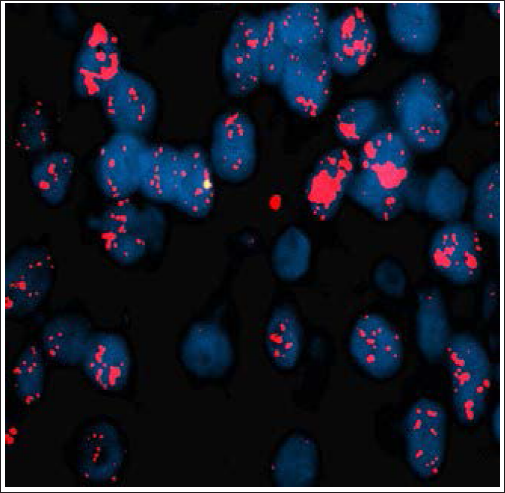
VEGFR-2 FISH analyses were performed, respectively, using the Abnova VEGFR-2 4q12/CEN 4p13 Texas Red/FITC Amplification dual color FISH probes (Abnova Jhongli, Taiwan). Gene amplification was identified with FISH technique on 3 µm-thick tissue sections with a Dako Histology FISH Accessory kit following the manufacturer’s instructions. FISH slides were read using an epifluorescence microscope (Zeiss, Oberkochen, Germany) at ×1000 magnification (Zeiss) with DAPI, SpectrumGreen, SpectrumRed, and double SpectrumGreen plus SpectrumRed filters (Abbott Molecular). The microscope was connected to a charge-coupled device camera and software (In Situ Imaging System version 5.3; MetaSystems Hard & Software, Altlußheim, Germany) for analyzing fluorescent signals. The amplification criteria for each probe was set to >15% of tumor nuclei with > 2.5 amplification signal per tumor nuclei within 100 tumor nuclei. Figure 1 illustrates an example of VEGFR-2 FISH positivity.
An Example of FISH Positivity for Amplified VEGFR-2 Gene.
Statistical Analysis
Statistical analysis was made using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY). Categorical variables were compared using Pearson’s Chi-square test or Fisher’s exact test. Continuous variables were compared using Mann-Whitney U or Student’s t-test for independent samples, depending on the normality of the data. Multivariate analysis (stepwise logistic regression) was used for determination of risk factors predicting high AFP levels. Recurrence-free survival was defined as the time elapsed between the date of hepatic transplantation and death from any cause or recurrence. OS analysis was based on the time elapsed between the date of hepatic transplantation and death from any cause and patients without event at the last follow up were censored. Survival rates were estimated using Kaplan-Meier analysis and inter-group comparisons were performed using the log-rank test. Multivariate analysis of potential factors for RFS and OS was performed via Cox proportional hazard model. Data were expressed as mean±standard deviation (SD), minimum-maximum, and percent (%), and 95% confidence interval (CI) where appropriate. P < .05 was considered statistically significant.
Results
Patient Demographics and Tumor Clinicopathological Characteristics
Mean±SD patient age was 56.6±8.2 years and males (92.6%) composed the majority of study population. In terms of the etiology of liver disease, 33 patients had hepatitis B (61.1%), 10 patients had hepatitis C (18.5%), 1 patient had nonalcoholic steatohepatitis (1.9%), and 10 patients had cryptogenic cirrhosis (18.5%). T 1-3 stage tumors were evident in 79.6% of patients along with microvascular invasion (48.1%), portal vein invasion (34.6%), and hepatic vein invasion (39.2%) in at least one-third of the study population (Table 1).
Patient Demographics and Tumor Clinicopathological Characteristics.
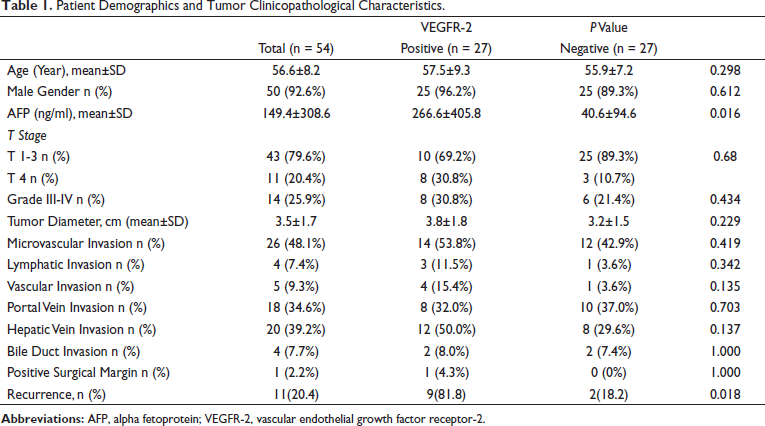
Amplified VEGFR-2 gene was evident in 27(50.0%) patients. Patient demographics as well as all clinicopathological parameters, except for serum AFP levels and recurrence rates, were similar between positive and negative groups for VEGFR-2 amplification. Presence of amplified VEGFR-2 gene was associated with significantly higher levels of AFP (mean±SD 266.6±405.8 vs 40.6±94.6 ng/mL, P = .016) and higher recurrence rate (81.8 vs 18.2%, P = .018) (Table 1). AFP levels were ≥100 ng/mL in 14(25.9%) patients and ≥400 ng/mL in 7(13.0%) patients.
Correlates of Higher AFP Levels
Lymphatic invasion (21.4 vs 2.5%, P = .049), vascular invasion (28.6 vs 2.5%, P = .013), presence of amplified VEGFR-2 gene (85.7 vs 35.0%, P = .001), and recurrence (63.6 vs 36.4%, P = .004) were significantly more common among patients with high (
Correlates of higher AFP levels
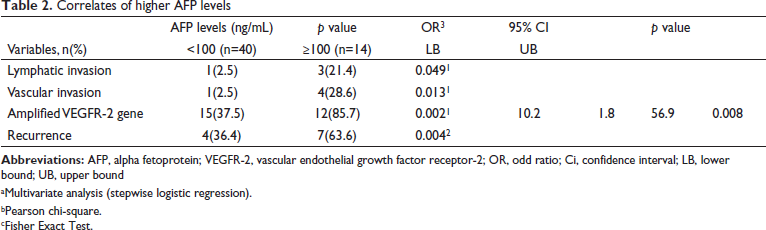
aMultivariate analysis (stepwise logistic regression).
bPearson chi-square.
cFisher Exact Test.
Presence of amplified VEGFR-2 gene was also significantly more common in the AFP≥400 group vs AFP<400 ng/mL group (85.7 vs 44.7%, P = .045).
RFS Time and OS Time According to Demographic and Clinicopathological Characteristics
During the median 68.5 months of the follow-up period (range, 3-78 months), 17 (31.5 %) patients died and 37 (68.5 %) were still alive and 5-year OS rate was 82% (median 89.8 months, range, 79.7 to 97.9 months).
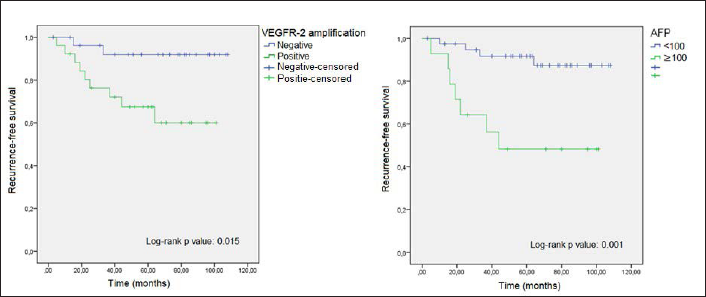
Presence of amplified VEGFR-2 gene was associated with significantly shorter RFS time (mean (95% CI) 72.8 (58.0-87.7) versus 101.3 (92.3-110.2) for positive and negative patients, respectively, P = .015), whereas it had no significant impact on OS time (median [95% CI] 76.8 [65.5-88.1] vs 91.2 [79.3-103.1] for positive and negative patients, respectively, P = .065) (Table 3, Figures 2 and 3).
Survival Outcome According to Demographic and Clinicopathological Characteristics.
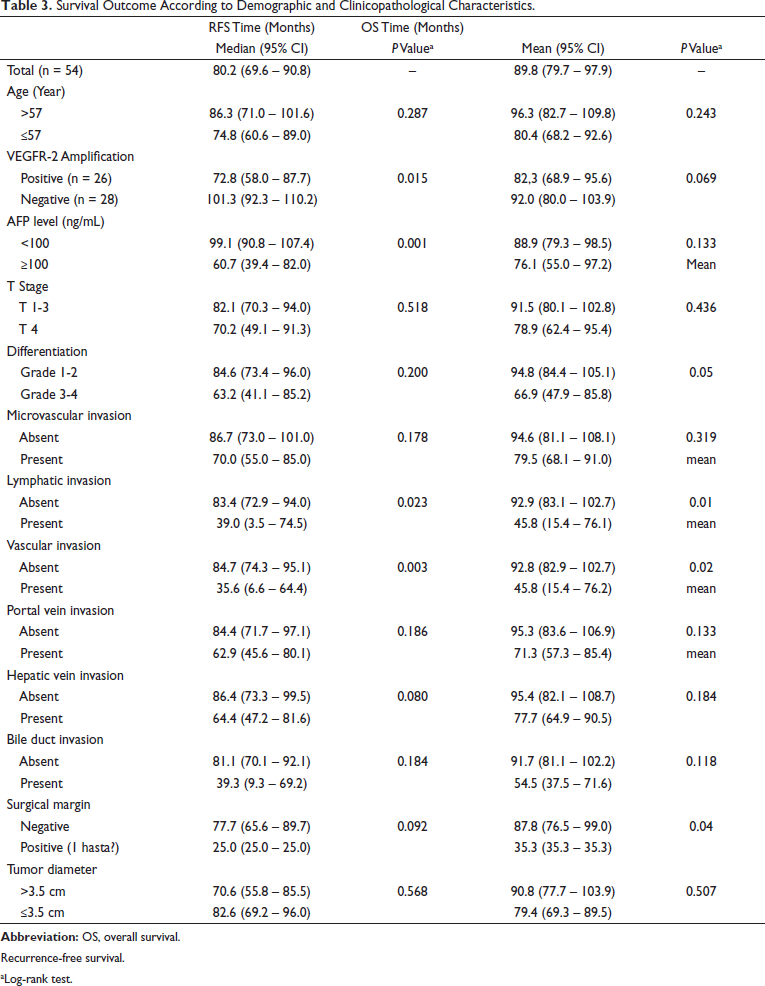
Recurrence-free survival.
aLog-rank test.
Kaplan-Meier Curves for Recurrence-Free Survival According VEGFR-2 Amplification and AFP Levels.
Kaplan-Meier Curves for Overall Survival According VEGFR-2 Amplification and AFP Levels.
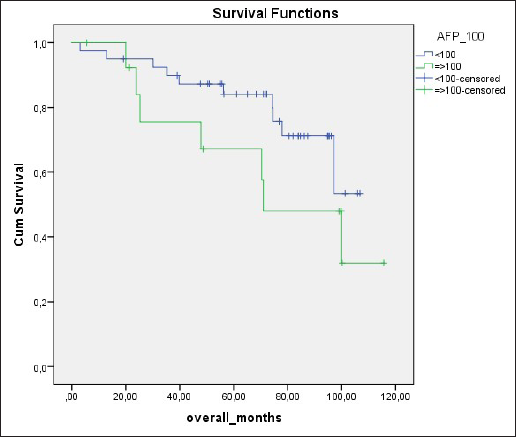
AFP levels of ≥100 ng/mL as compared to lower AFP levels were associated with significantly shorter mean RFS time (60.7 (39.4 – 82.0) vs. 99.1 (90.8 – 107.4), p=0.001) and a nonsignificant tendency for shorter median OS time (72.0 [53.8-90.2] vs 93.6 [83.9-103.3], P = .061) (Table 3, Figures 2 and 3).
Amongst the tumor clinicopathological parameters studied, the presence of lymphatic invasion (46.5 vs 92.3 months, P = .005 and 39.0 vs 83.4 months, P = .023, respectively) and vascular invasion (46.5 vs 92.2 months, P = .008 and 35.6 vs 84.7 months, P = .003, respectively) were the only parameters associated both with significantly shorter median OS time and median RFS time (Table 3).
Cox-regression analysis identified lymphatic invasion (HR, 12.4, 95% CI, 2.7-57.3, P = .01) and vascular invasion (HR, 8.3, 95% CI, 2.3-29.8, P = .01) as the only independent significant determinants of poor OS and poor RFS, respectively.
Discussion
Our findings revealed the presence of amplified VEGFR-2 in at least half of HCCs. Presence of amplified VEGFR2, while had no significant impact on OS, significantly predicted higher AFP levels and was associated with significantly higher recurrence rate and a shorter RFS. This seems notable given that higher AFP levels were associated with a non-significant tendency for shorter OS and significantly shorter RFS, and with more common presence of 2 tumor pathology parameters (lymphatic invasion and vascular invasion) that significantly predict OS and RFS, respectively.
High baseline AFP plasma levels (>200 ng/mL) were reported to have a negative impact on OS in HCC patients, 26 while the association of elevated AFP concentrations with poor prognosis in HCC patients has also been stated in the EASL guidelines. 27
The current study investigated the relationship VEGFR-2 amplification and AFP for the first time in HCC and identified that VEGFR-2 amplification was a significant independent predictor of AFP levels of ≥100 ng/mL. Presence of amplified VEGFR-2 gene and AFP levels≥100 ng/mL were both associated with higher rate of recurrence. Given the association of high AFP levels also with poor prognostic characteristics such as tumor invasiveness and poor survival in the current study, our findings seems to emphasize the potential role of VEGFRf-2 inhibition in improving prognosis among HCC patients via decreasing the expression of AFP.
Notably, data from REACH trial in HCC patients regarding the use of ramucirumab, an anti-VEGFR-2 monoclonal antibody that specifically binds to VEGFR-2, revealed no significant survival benefit in the overall study population, whereas further subgroup analysis (REACH-2 trial) indicated the efficacy of the treatment in terms of improved OS and progression free survival (PFS) in a subgroup of patients with AFP ≥400 ng/mL, resulting in approval of the drug as second-line agent for advanced HCC (after sorafenib) in patients with AFP ≥400 ng/mL.28-30 In this regard, our findings seem to provide additional data that would contribute to a better understanding of the mechanism underlying ramucirumab efficacy.
Our findings indicate significantly higher levels of AFP secretion by tumors with vs without amplified VEGFR-2 gene (median 266.6 vs 40.6 ng/mL), and thus indicate high AFP levels as potential predictive factor of efficacy of VEGFR-2 inhibitors in HCC patients. Likewise, a consistent correlation of an early decrease of > 20% in AFP levels following sorafenib with objective response and better outcome (both OS and PFS) has been reported in several studies conducted with advanced HCC patients.31-34 Moreover, VEGF-A gene amplification with FISH was reported to be 11% and associated with response to sorafenib in a mouse model study, and authors considered the VEGF-A amplification as a potential biomarker of response to VEGF-A-blocking drugs in HCC. 35
To the best of our knowledge, this is the first study to show an association between elevated AFP and VEGFR-2 amplification in HCC, indicating genetic information involving the VEGFR-2 signal pathway in HCC and highlighting VEGFR-2 amplification among the factors that increase AFP in this signal pathway. In this regard, FISH seems to be an appropriate method to examine VEGF and VEGFR signal pathways for guidance on pretreatment identification of responsiveness to therapy. Notably, although the soluble VEGF-A inhibitor antibody bevacizumab with atezolizumab was for the first time associated with a survival difference versus sorafenib, the gene amplification of VEGF-A in HCC was shown to be 11%.35, 36
Although no survival impact of amplified VEGFR-2 in HCC was noted in the current study, it should be noted that AFP levels were ≥400 ng/mL only in 7(13.0%) patients in our study population. Hence, given the suggested role of AFP levels ≥400 ng/mL in prediction of higher treatment efficacy with VEGFR-2 inhibitors, there is a need for larger scale studies in subpopulations of HCC patients with AFP levels of ≥400 ng/mL.
VEGFR-2 is a conserved marker for hepatic progenitors and a functional receptor instructing early liver development. 37 After the first description of VEGFR-2 amplification in glioblastoma multiforme in 2005, 38 the association of FISH positivity for VEGFR-2 amplification with poor oncological outcome has been reported in several other cancer types including non-small lung cancer, 39 triple-negative breast cancer, 40 childhood brain tumors. 41 In the study of glioblastoma multiforme, if tumors have more than 7 copy numbers per one centromere, these were defined as high-level amplification and if copies were 3 to 7, these were considered as low-level amplification. 38 Johansson and et al, defined amplification as the ratio between gene copies and centromere probe >2 in >10% of cancer cells. 40 Blom and et al defined amplification when 6 or more signals per nuclei were present in at least 20% of tumor cells. 41 In our study, >2.5 signal per nuclei in >15% of tumor nuclei within 100 tumor cells was considered as amplification. Nonetheless, several studies reported no association between VEGFR-2 amplification positivity and VEGFR-2 protein expression detected by immunohistochemistry.25, 40, 41
In patients with HCC, VEGFR-2 overexpression has been related to progressive pathological features (ie large tumor diameter, poor differentiation, elevated AFP, and multi-focal disease) and poor prognosis. 21 In the current study, amongst the clinicopathological characteristics studied, only serum ALP levels differed with respect to presence of VEGFR-2 overamplification, while tumor invasion and VEGFR-2 amplification were more likely in case of high AFP levels and VEGFR-2 overamplification emerged as an independent predictor for elevated AFP.
An EpCAM positivity rate of 2% in HCC and normal liver cells suggests that HCC may not be of epithelial origin and may therefore be a chemo-resistant tumor for the epithelial tumor chemotherapies. In our study, half of the tumors were VEGFR-2 amplification positive. Previous embryological studies suggesting a mesodermal origin for VEGFR-2 may partially account for the clinical behavior of HCC including chemo-resistance.42, 43 If this assumption proves valid, this would probably change the current paradigm of HCC treatment.
Certain limitations to this study should be considered. First, potential lack of generalizability seems to be the most important limitation due to small sample size. Second, in accordance with the candidacy criteria for liver transplantation that considers AFP level >1000 ng/as an exclusion criterion for liver transplantation, 27 the number of patients with an AFP ≥ 400 ng/ml in our study population comprising liver-transplanted patients was too small to conduct a subgroup analysis.
In conclusion, our findings revealed the presence of amplified VEGFR-2 gene and its association with serum AFP elevation for the first time in HCC. VEGFR-2 amplification was directly associated with RFS and it also emerged as a significant predictor of elevated AFP. Accordingly, our findings seems to indicate the role of AFP elevation in VEGFR-2-mediated tumorigenesis as well as the likelihood of amplified VEGFR-2 gene and high AFP levels to determine the efficacy of VEGFR-2-inhibitors in HCC patients. Further investigation of clinicopathological characteristics and oncological outcomes related to amplified VEGFR-2 gene in a larger subpopulation of HCC patients with higher AFP levels as well as the examination of other VEGF and VEGFR signal pathways using the FISH methodology may contribute to the development of the most effective combination in HCC patients.
Footnotes
Author Contributions
Conceptualization, SS; data curation, SS, UIK, MD, GBD, MA, MB, and EQ; methodology, SS, UIK, MD; writing—original draft, SS; writing—review and editing, SS, UIK, MD, GBD, MA, MB, and EQ.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the ethical principles stated in the “Declaration of Helsinki” and approved by the Human Research Ethics Committee of Demiroglu Bilim University (No: 2016-59).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was funded by Turkish Society of Medical Oncology (P-TTOD-2018-35).