
Abstract
Objective:
α-fetoprotein (AFP) expression is activated during the embryonic stage or hepatocellular carcinogenesis, so it is presumed that AFP is a key endogenous molecule to promote cell proliferation or differentiation. We carried out gene screening in an unknown family with hyper-alpha-fetoproteinemia and some sporadic menopausal women, and discussed the relationship between AFP expression and liver cirrhosis.
Methods:
Peripheral blood samples from family members, patients with malignant liver tumors, and normal controls were collected. Full-length sequence of AFP was amplified and directly sequenced, and compared with normal controls. HNF-1α and HNF-1β in plasma levels of family members, patients with liver cancer, newborns, pregnant women, and normal subjects were detected by ELISA, and the relationship between HNF-1 and AFP mutation or high expression was evaluated.
Results:
There was a mutation in AFP promoter region at c.-200 C>T, which was located at the binding site of AFP hepatocyte nuclear factor 1 (HNF-1). AFP was higher than 4000 ng/L in all members carrying the mutation, but liver cancer was excluded in the family with hyper-alpha-fetoprotein. However, cirrhosis occurred in post-menopausal women. The cases reviewed showed that unknown hyper-alpha-fetoprotein was closely related to HNF-1 binding point of AFP in post-menopausal women with cirrhosis (7/11), while the plasma levels of HNF-1α and HNF-1β were not significantly different.
Conclusion:
The mutation of the HNF-1 binding point of AFP may lead to an abnormal high expression of AFP by altering the binding of HNF transcription factors, which is closely related to cirrhosis in menopausal women.
Introduction
For a long time, people only care about the diagnostic value of α-fetoprotein (AFP) , while ignoring its biological effects. There are many patients with high serum AFP for unknown reasons, which brings great confusion to clinicians and patients alike. This unexplained high AFP is internationally named as “high alpha-fetoprotein syndrome.” Currently, high AFP is not considered to be a concurrent phenomenon caused by a certain disease, but is an independent disease.1,2 The high expression of AFP may be related to the structure of the AFP gene and hepatocyte nuclear factor 1 (HNF-1).1-3
Until now, 2,766 types of AFP single nucleotide polymorphisms (SNPs) have been found, most of which are variations of exon or intron regions, while the promoter mutations are rarely reported. AFP can be used as a transport carrier to bind estrogen, fatty acids,heavy metal ions, drugs and some environmental contaminants, etc.3, 4 AFP is activated during embryogenesis, hepatitis, cirrhosis, and hepatocyte carcinogenesis.5-8 Recent studies have shown that liver cirrhosis differs between genders; that the progression of liver fibrosis in pre-menopausal women is slower than in men and post-menopausal women; and that estrogen reduces the risk of liver cancer. 7 Estrogen receptor-α (ERα) and estrogen receptor-β (ERβ) play opposite roles, which together regulate cell proliferation and apoptosis. ERα mediates cell proliferation, while ERβ mediates cell anti-proliferation and pro-apoptosis. The level of estrogen is closely related to disease progression. The levels of estrogen and its receptors in menopausal women vary greatly, while the rate of liver fibrosis in post-menopausal women is higher than that in pre-menopausal women. The research investigates the relationship between unexplained high AFP and liver cirrhosis in post-menopausal women.
Materials and methods
Information on a family with hyper-alpha-fetoprotein
Figure 1 shows unexplained high AFP in a family. There are five members of the family with high AFP, including one male as a proband (III2), four females (I2, II2, II3, and III4); the grandmother of the proband (I2) died of cirrhosis 5 years ago. Pathology and imaging data of the mother of the proband (II2) are shown in Figure 2.

Pedigree of hyperalphafetoproteinemia.
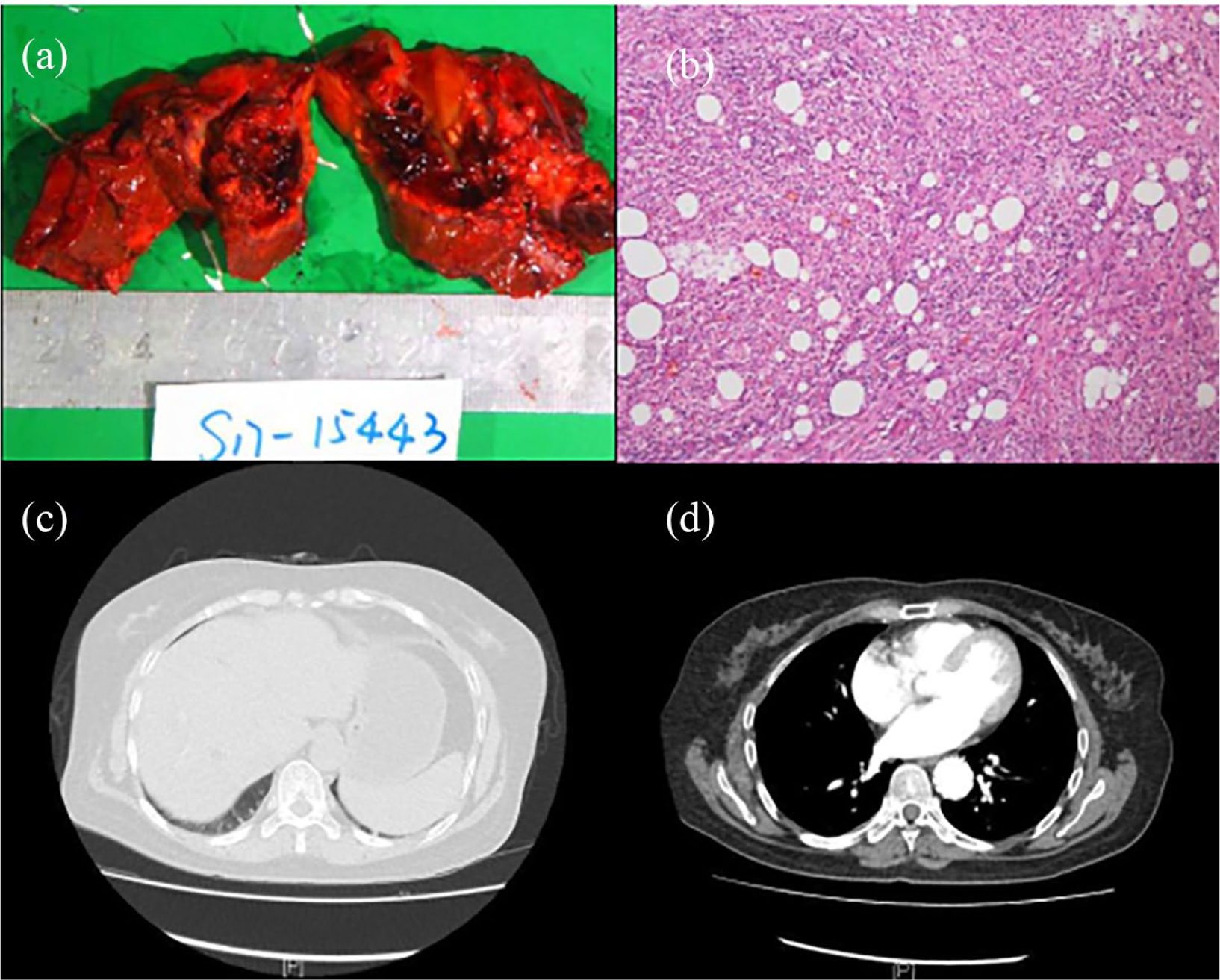
Histopathology and imaging examination of the mother of the proband.
Histopathology showed focal hepatic abscess formation with hemorrhage, necrosis, and organization, cholestasis, focal intrahepatic bile duct dilatation with stones, small bile duct hyperplasia around the portal area, peripheral hepatic parenchymal fibrosis (Ishak score=5 points), cirrhosis with a few nodules, mild edema, and inflammatory cell infiltration. Two peripheral lymph nodes showed reactive hyperplasia. Immunohistochemistry (IHC) showed CD68-PGM1 (+), Heppar1 (peripheral liver, +), PAS (−), SMA (partial, +), Ki67 (+, 10%), and reticular fiber (peripheral liver, +).
The imaging showed an imbalance of the hepatic lobe, caudate lobe enlargement, left hepatic lobe atrophy, a kind of round long T1 and long T2 signal shadow in the lower right lobe of the liver, clear, approximately 2.9cm × 2.8cm, visible mural nodules in the section (see the point-like high-density shadow). The enhanced scanning wall nodules can be seen obviously enhanced; there is flaky transient enhancement around the arterial lesion, thickening and strengthening of the adjacent right peritoneum. The surrounding fat gap is blurred; the lesion is connected with the colonic hepatic curvature; and the local intestinal wall is thickened. In the lumen of the common bile duct, a nodular slightly high-density shadow was seen; the common bile duct was dilated; and the wall was thickened and strengthened. The intrahepatic bile duct was diffused and cast with slightly high density, and the intrahepatic bile duct was enlarged.
Retrospective analysis
In order to systematically understand the frequent occurrence of patients with unexplained high AFP, we retrospectively analyzed a total of 11 menopausal women admitted to our hospital during the past 4 years. There were 55 pregnant women, 22 newborns, and 103 patients with liver cancer; 56 healthy persons were collected as a reference for the study. According to the investigation of the clinical data, the inclusion criteria were:
(a) Exclusion of viral hepatitis (A, B, C, D, and E)
(b) The patients underwent re-examination of AFP within 1 week, and the high expression of AFP was stable.
(c) According to the imaging data of the patients, liver cancer was excluded clinically, among which 7/11 patients had fatty liver, cirrhosis, and other clinical manifestations.
(d) Nearly 33.3% of the patients presented a weak or positive autoantibody.
All family members signed informed consent to extract peripheral blood (II2, II3, III1, III2) and EDTA-2K anticoagulation, and plasma of healthy people and high AFP groups (pregnant women, newborns, liver cancer) were collected. Peripheral blood of family members (II2, II3, III1, III2) and 10 cases of malignant hepatocellular tumors (7 cases of hepatitis B surface antigen positive malignant hepatocellular tumors, 2 cases of hepatitis B surface antigen negative malignant hepatocellular tumors, and 1 case of normal AFP malignant hepatocellular tumors) were collected. Peripheral blood genomic DNA was extracted by using a centrifugal adsorption column DNA extraction kit (Promega-Tiangen, Beijing, China), and the procedure was carried out according to the product specification.
Gene amplification and sequencing
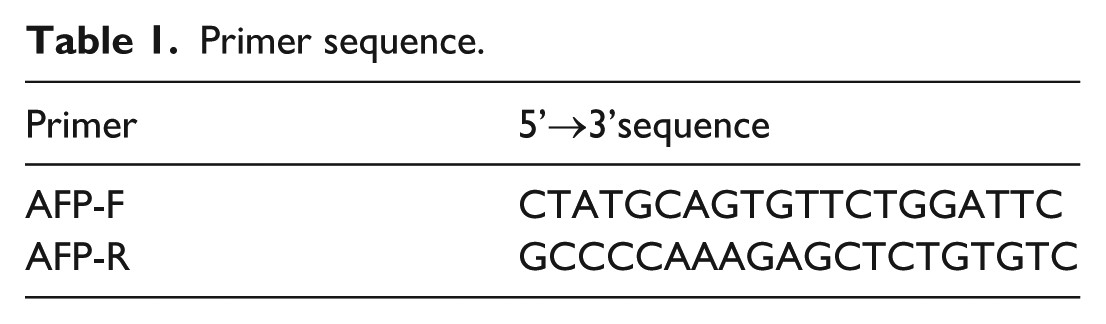
Amplification primers (Table 1) were designed by using PRIMER 6.0 software, and the primers covered the full length of the AFP gene, including the 300 bp flanking sequence upstream of the promoter. Fragment amplification was performed using an ABI 9700 thermal cycler. The PCR product was sent to BioSune Co., Ltd. (Fuzhou, China) for purification and sequencing. The sequencing instrument was ABI 3700.
Primer sequence.
Determination of serum levels of HNF-1α and HNF-1β
Determination of serum (or plasma) levels of HNF-1α and HNF-1β were measured using a specific enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Minneapolis, MN, USA), according to the manufacturer’s protocols.
Statistical analysis
The rank sum test of ELISA results was performed by SPSS18.0 software. Both the “progressive significance” and the “unilateral significance” (precise significance) were greater than 0.05. It was concluded that there was no significant difference.
Results
High AFP pedigree
The related clinical examination results of family members are shown in Table 2. Serum AFP were all above 4000 ng/L in members carrying AFP gene mutations.
General clinical data of members with high AFP level.
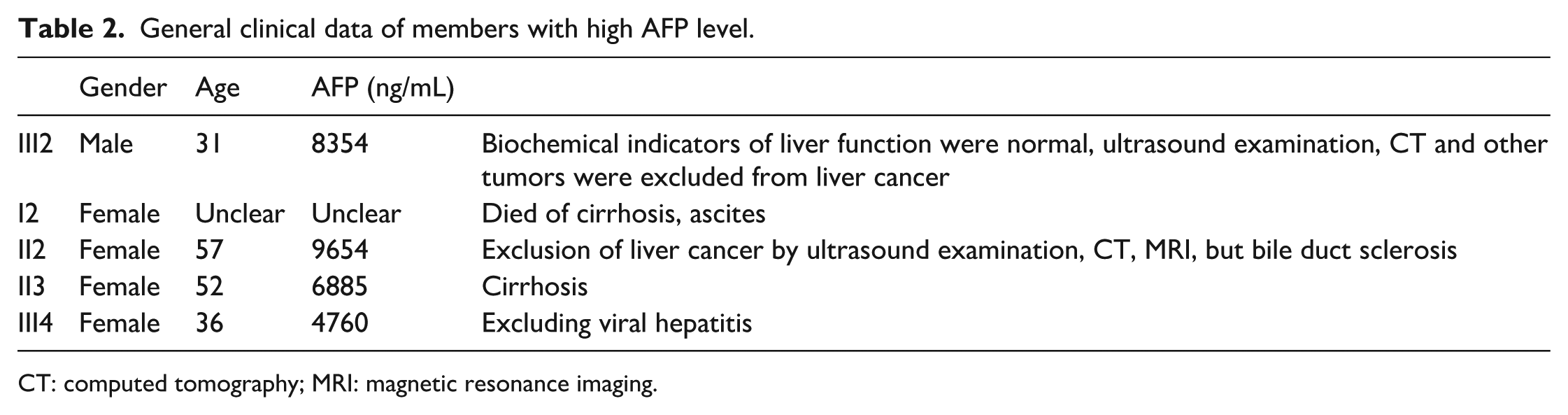
CT: computed tomography; MRI: magnetic resonance imaging.
Full-length sequencing of AFP gene
In the family (II2, III2, III4), c.200 C>T mutation (heterozygous mutations) was found in the AFP promoter region (Figure 3), and the mutation was located at the HNF-1 transcript binding site.
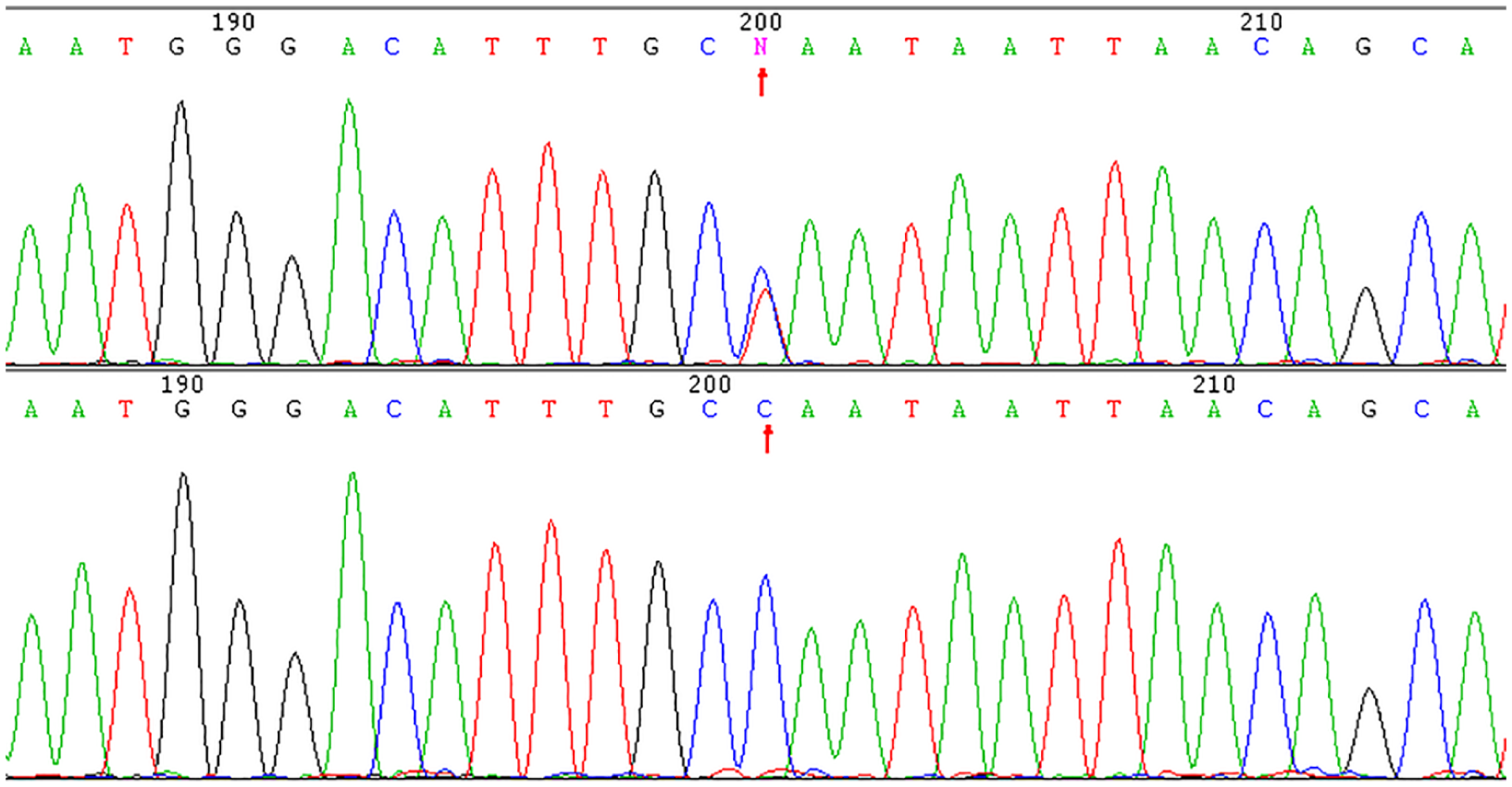
AFP promoter mutation.
Serum HNF-1α and HNF-1β determining
The serum level of HNF-1α in this study was not significantly different from the healthy control group, neonatal group, pregnant group, and suspected hereditary disease group; however, the difference was statistically significant compared with the liver cancer group. There was no significant difference in the serum levels of HNF-1β the healthy control group, the neonatal group, the pregnant group, the suspected genetic disease (SD) group, and the liver cancer group (Table 3).
Statistical analysis of serum HNF-1α levels and HNF-1β levels.

Retrospective analysis
A case review showed that unexplained high AFP is closely related to cirrhosis (8/11), and in most patients with the AFP gene HNF binding point mutation (10/11) (Table 4).
Retrospective analysis of clinical conditions and sequencing results of patients with unexplained hyperalphafetoproteinemia.
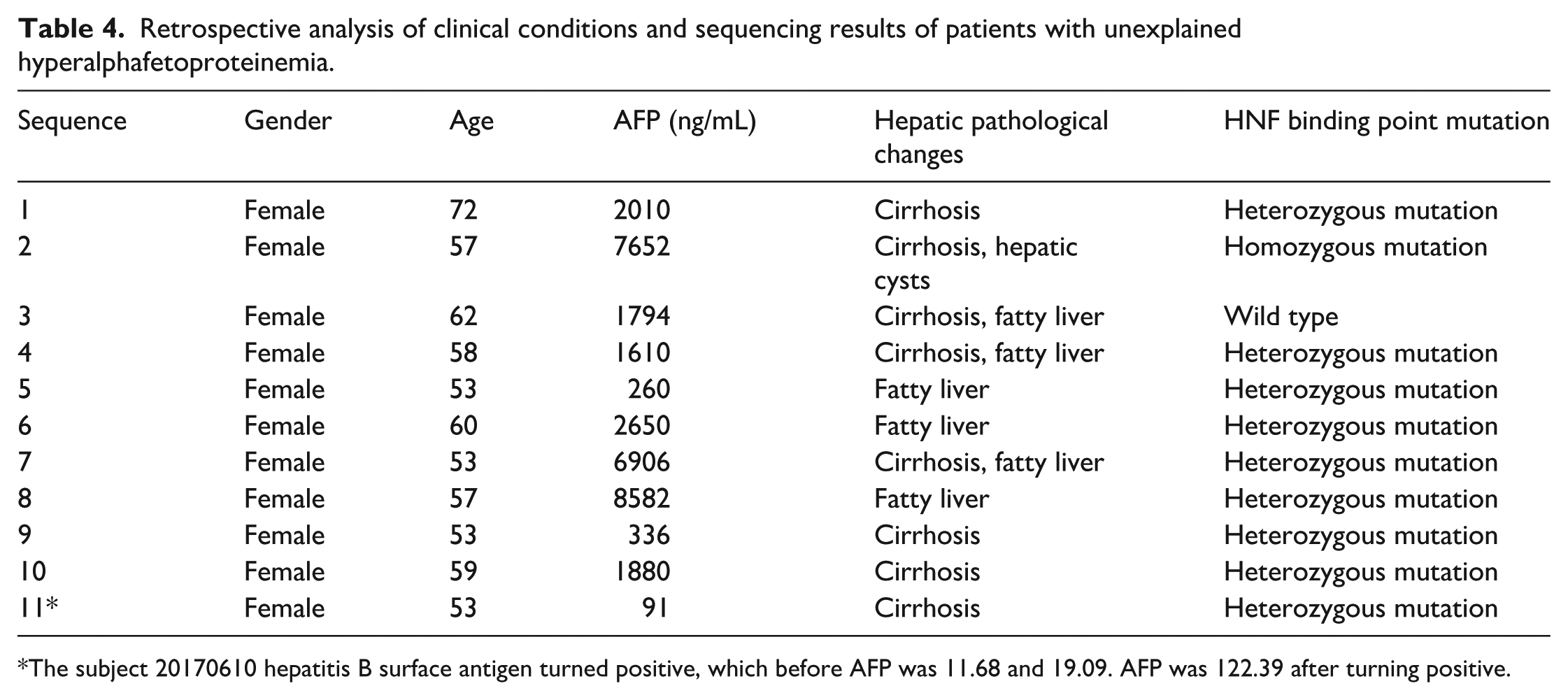
The subject 20170610 hepatitis B surface antigen turned positive, which before AFP was 11.68 and 19.09. AFP was 122.39 after turning positive.
Discussion
The clinical diagnostic value of AFP has been relatively clear, and its relationship with liver cancer and reproductive system tumors is also clear. AFP mutations have also been found in recent years. 9 The gene includes 14 exons and 15 introns, which can express 590 amino acids, and the signal peptide is 19 amino acids at the N-terminus. The gene contains a cap structure, located 44bp upstream of the transcription initiation site, with two AFLU families (moderate repeat sequences unique to primates and one of the most active genetic regions in the genome). At 27 bp upstream of the cap sequence, there is also the classic “TATA” box structure. 10 During the evolution of species, AFP is conservative and its gene structure is very stable. The AFP promoter is located in the 200 bp region upstream of the gene, 11 where there are many binding sites of transcriptional regulatory factors, which are related to the regulation of AFP.12,13 The AFP promoter region has two hepatocyte nuclear factor-1 (HNF-1) binding sites and non-tissue-specific NF-1 binding sites partially overlap with C/EBP and HNF1 binding sites. Low concentration of NF-1 produces a weak activation effect on the AFP promoter, while high concentration inhibits promoter activity. 8 Mutation will enhance the binding of HNF-1 and attenuate the binding of NF-1. 14 In general, the point mutation of the gene will change the binding sequence or structure, and weaken the binding ability. However, the point mutation of the HNF-1 binding site in the AFP promoter region changed the sequence at the promoter. We suspect that this mutation alters the signal that regulates AFP expression, initiates high expression of AFP, enhances HNF-1 binding, and attenuates NF-1 binding.
In this study, the results showed that there was a c.-200 C>T mutation in the HNF binding site in the pedigree, which lead to an increase in the homology of HNF-1α binding to the AFP promoter sequence. This resulted in enhanced transcriptional activity of the AFP gene, which causes a significant increase in the AFP serum level, and the genotype is consistent with the clinical phenotype. All mutation carriers in the family presented with high AFP, while the wild type presented with normal AFP in the serum level. This suggests that HNF binding point c.-200 C>T can affect the binding of HNF-1α, and thus affect the expression of AFP, which may be closely related to the persistent high alpha fetoprotein syndrome in the family. In addition, the c.-200 C>T mutation may also interfere with the activity of HNF-1α, leading to abnormal expression of AFP. It have found that HNF-1α (-119 G>A and -55 C>A) sites were mutated, or rs7310409 polymorphism were independently and significantly correlated with serum level of AFP. 15 Moreover, HNF-1 a rs7310409 polymorphism may play a genetic role in determining the serum level of AFP, but the exact mechanism requires further study.
AFP in neonates and pregnant women is a physiological increase. At this time, AFP is not specifically activated by hepatocyte HNF-1 to initiate AFP transcription, and the yolk sac produces AFP. The AFP of hepatic malignant tumors is a pathological increase. Some studies have shown that there are differences in the expression of HNF-1 between liver tissue and paracancerous tissues of hepatic malignant tumors, as well as differences in low-differentiated and medium-differentiated cancer tissues. HNF-1α and HNF-1β in the serum level in this study were not significantly different in mutant families from healthy controls, neonates, pregnant women, or groups with suspected genetic diseases. When HNF-1 binds to point mutation, HNF-1 binding capacity is enhanced.
There are numerous physiologic and biochemical changes in menopause that can affect the function of the liver and mediate the development of liver disease. Menopause represents a state of increasing estrogen deficiency, and this loss of estrogen in the setting of physiologic aging increases the likelihood of mitochondrial dysfunction, cellular senescence, declining immune responses to injury, and disarray in the balance between antioxidant formation and oxidative stress. The sum effect of these changes can contribute to increased susceptibility to the development of significant liver pathology and hepatocellular carcinoma, as well as accelerating the progression of fibrosis in liver diseases. 16
Conclusion
As a powerful endogenous antioxidant, estrogen and its receptor change significantly during menopause. The relationship between the structure of AFP and estrogen can provide good material and a basis for the regulation mechanism of female endocrine hormones.
Footnotes
Author contributions
Q-CL, FG, and SZ planned the project. Q-CL, J-WW, and FG conceived of and designed the study. G-ZL, and Q-CL performed the sample collection. Y-JG, FG, and CL performed immunohistochemistry. J-WW, Q-CL, and G-ZL, participated in the in vivo procedures. Q-CL, FG, Y-JG, and SZ performed the expression analysis. Q-CL, FG, Y-JG, and SZ analyzed the data and drafted the manuscript. All authors reviewed the manuscript and approved the final version. J-WW, YC, and Q-CL contributed equally to this work.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (no.81871293, no.81572442, and no.81800070), Fujian Natural Science Foundation (No.2018J01848), Medical innovation in Fujian Province (2019-CX-27), and Youth fund of Fujian Provincial Department of Health (2019-1-41 and 2019-1-46). These funding sources played a key supportive role for sample collection, molecular analysis of patient samples, bioinformatics analysis.