
Abstract
PURPOSE:
The glucose-regulated protein 78 (GRP78), also referred to as immunoglobulin heavy chain binding protein (BiP) (BiP/GRP78), is a major molecular chaperone in the endoplasmic reticulum (ER) and is extensively expressed in human neoplasms. Although the enhanced expression of BiP/GRP78 has been described to be associated with poor prognosis in gastric cancer (GC), details regarding its prognostic significance remain unclear. The aim of this study was to elucidate the prognostic role of BiP/GRP78 in patients with GC.
METHODS:
Study subjects included 328 patients who underwent surgical resection. Tumor specimens of primary tumors underwent immunohistochemical staining for BiP/GRP78.
RESULTS:
BiP/GRP78 was highly expressed in 57% (188/328) of patients. High expression of BiP/GRP78 was significantly associated with older age, male, disease staging, T factor, lymph node metastases, differentiation, lymphatic permeation, and vascular invasion. According to univariate analysis, age, disease staging, T factor, N factor, lymphatic permeation, vascular invasion, and BiP/GRP78 expression were significant prognostic factors for OS. In particular, high BiP/GRP78 expression was proven to be a significant predictor of prognosis in patients with older age, female sex, early disease stage, T1-2 factor, well or moderately differentiated tumors, and negative vascular invasion.
CONCLUSION:
BiP/GRP78 is significantly associated with tumor aggressiveness and progression. The increased expression of BiP/GRP78 was identified as an independent factor for predicting poor OS in patients with early stage of disease, especially T1-2 factor.
Introduction
Gastric Cancer (GC) is a common neoplasm ranking as one of the most common causes of cancer-related death worldwide, especially in East Asian countries such as China, South Korea, and Japan [1]. The pathogenesis of this cancer is poorly understood despite many studies conducted to investigate the tumor development and carcinogenesis of GC. In clinical practice, gastrectomy with regional lymphadenectomy has been widely used as a standard treatment for patients with stage I to III GC; however, about 20 to 30% of patients develop distant or local recurrence and die regardless of appropriate treatment. Generally, disease stage has been thought to be the most important predictor of prognosis following curative surgery or systemic therapy in patients with GC. No molecular biomarker has been established as a useful measurement to correlate with the therapeutic efficacy and outcome after treatment in patients with GC. Future research is needed to contribute to the development of a new molecular targets and the discovery of novel mechanisms related to the pathogenesis and tumorigenesis of GC.
The glucose-regulated protein 78 (GRP78), also referred to as immunoglobulin heavy chain binding protein (BiP) (BiP/GRP78), is a 78 kDa protein and a major molecular chaperone in the endoplasmic reticulum (ER) [2, 3]. BiP/GRP78 is involved in the folding and assembly of newly synthesized proteins in the ER and enhanced resistance to ER-stress-induced apoptosis [2, 3]. This biomarker is known to be extensively expressed in many cancer cell lines and human neoplasms, and correlates with malignant characteristics, metastasis, tumor progression, and resistance to chemotherapy [3, 4]. Several researchers have discussed the clinical and pathological features related to survival, tumor aggressiveness, and response to chemotherapy in various human neoplasms such as lung cancer, breast cancer, hepatocellular carcinoma, prostate cancer, and GC [3, 5, 6, 7, 8, 9, 10, 11, 12]. Recently, Zheng et al. reported that the upregulated expression of BiP/GRP78 was closely associated with tumor growth, invasion, and metastasis in GC and had a significant relationship with poor prognosis and aggressive behavior in this cancer type [13]. In their study, the expression level of BiP/GRP78 was significantly higher in GC lesions than in non-neoplastic lesions. Yang et al. have reported that the increased expression of BiP/GRP78 promotes GC cell proliferation and is associated with shorter survival [14]. Both studies suggest that elevated BiP/GRP78 expression is indicative of poor outcome in patients with GC [13, 14]. However, detailed features regarding the prognostic significance of BiP/GRP78 expression have not been elucidated. In the present study, we performed clinicopathological analysis to evaluate the prognostic significance of BiP/GRP78 expression in patients with GC who underwent surgical resection.
Materials and methods
Patients
A total of 328 consecutive patients who underwent surgery for GC at our institution between January 2000 and December 2009 were selected for inclusion in the current study. We obtained all clinicopathological data such as age, sex, histology, lymphatic permeation, vascular invasion, lymph node metastasis, and disease staging from the database. This study was approved by the institutional review board of Gunma University Hospital (ethical committee for clinical studies – Gunma University Faculty of Medicine).
The age of the patients ranged from 28 to 88 years, and the median age was 68 years. None of the patients had received neoadjuvant chemotherapy. All surgical specimens were reviewed and classified according to the World Health Organization classification by an experienced pathologist who was unaware of clinical or imaging findings. Pathological tumor-node-metastasis stages were established using the International System for Staging adopted by the American Joint Committee on Cancer and the Union Internationale Contre le Cancer. Histologically, all patients had histology of adenocarcinoma (AC), and 181, 65, 63, and 18 of all patients had stage I, II, III, and IV tumors, respectively. The day of surgery was considered the starting day for measuring postoperative survival. The follow-up duration ranged from 50 to 5430 days (median, 2055 days). The author’s approach to the evaluation and resection of these tumors has been previously described [15].
Immunohistochemical staining as representative imaging: Immunohistostaining of BiP/GRP78 showed the immunohistostaining pattern of cytoplasm or membrane [scoring of 4 (A), scoring of 3 (B) and scoring of 2 (C)]. Figure 1D revealed a negative staining of BiP/GRP78 expression (scoring of 1).
BiP/GRP78 was detected using a rabbit monoclonal antibody (Cell Signaling Technology, Danvers, MA, USA, 1:100 dilution). The detailed protocol for immunostaining has been published elsewhere [16]. Immunohistochemical staining was performed on paraffin sections using a polymer peroxidase method (Histofine Simple Stain MAX PO (MULTI) kit; Nichirei Corporation, Tokyo, Japan). Briefly, deparaffinized, rehydrated sections were treated with 0.3% hydrogen peroxidase in methanol for 30 min to block endogenous peroxidase activity. To expose antigens, sections were autoclaved in 10 mmol/L sodium citrate buffer (pH 6.0) for 5 min, and cooled for 30 min. After rinsing in phosphate-buffered saline (PBS), sections were incubated with anti-BiP/GRP78 antibody (1:100) overnight. Subsequently, the sections were incubated with the Histofine Simple Stain MAX PO (MULTI) kit (Nichirei Corporation). The peroxidase reaction was performed using 0.02% 3,3-diaminobenzidine tetrahydrochloride and 0.01% hydrogen peroxidase in 0.05 M tris-HCl buffer, pH 7.6. The expression of BiP/GRP78 was considered positive only if distinct cytoplasmic and plasma membrane staining was present. Negative control tissue sections were prepared by omitting the primary antibody. BiP/GRP78 expression scores were assessed by the extent of staining as follows: 1,
Patient’s demographics according to BiP/GRP78 expression
Patient’s demographics according to BiP/GRP78 expression
Percentage of BiP/GRP78 expression according to scoring of 1 to 5: The percentages with BiP/GRP78 scoring of 1, 2, 3, 4 and 5 were recognized in 18% (58/328), 25% (83/328), 27% (88/328), 22% (74/328) and 8% (26/328), respectively. 
P-values of
Results
Expression of BiP/GRP78 by immunohistochemical staining
Immunohistochemical staining was performed on the 328 primary GC tumors. Figure 1 shows representative images of BiP/GRP78 protein expression. The immunohistochemical staining of BiP/GRP78 expression was recognized in the cancer cells of tumor specimens, and localization of staining to the cytoplasm and membrane was identified. The percentages of samples with BiP/GRP78 expression scoring of 1, 2, 3, 4 and 5 were 18% (58/328), 25% (83/328), 27% (88/328), 22% (74/328), and 8% (26/328), respectively. BiP/GRP78 was highly expressed in 57% (188/328) of all patient tumor samples, and the percentages with BiP/GRP78 scoring of 1, 2, 3, 4 and 5 were recognized in 18% (58/328), 25% (83/328), 27% (88/328), 22% (74/328) and 8% (26/328), respectively (Fig. 2).
Table 1 exhibits patient characteristics according to the expression status of BiP/GRP78. High expression of BiP/GRP78 was significantly associated with age, sex, disease staging, T factor, lymph node metastases, differentiation, lymphatic permeation, and vascular invasion.
Univariate and multivariate survival analysis in all patients
Univariate and multivariate survival analysis in all patients
Survival analysis of BiP/GRP78 according to different variables
The 5-year OS and PFS rates for all patients with GC were 75% and 74%, respectively. Out of 328 patients, 101 died after the initial surgical treatment. According to univariate analysis, age, disease staging, T factor, N factor, lymphatic permeation, vascular invasion, and BiP/GRP78 expression were significant prognostic factors for OS. By multivariate analysis, age, disease staging, and lymphatic permeation were confirmed as independent markers for predicting poor prognosis in patients with GC (Table 2). Figure 3 shows Kaplan-Meier survival curves according to the expression status of BiP/GRP78.
Kaplan-Meier survival curve of overall survival (OS) and progression-free survival (PFS) according to the expression of BiP/GRP78: A statistically significant difference in OS and PFS was recognized between patients with high and low BIP/GRP78 expression [OS, 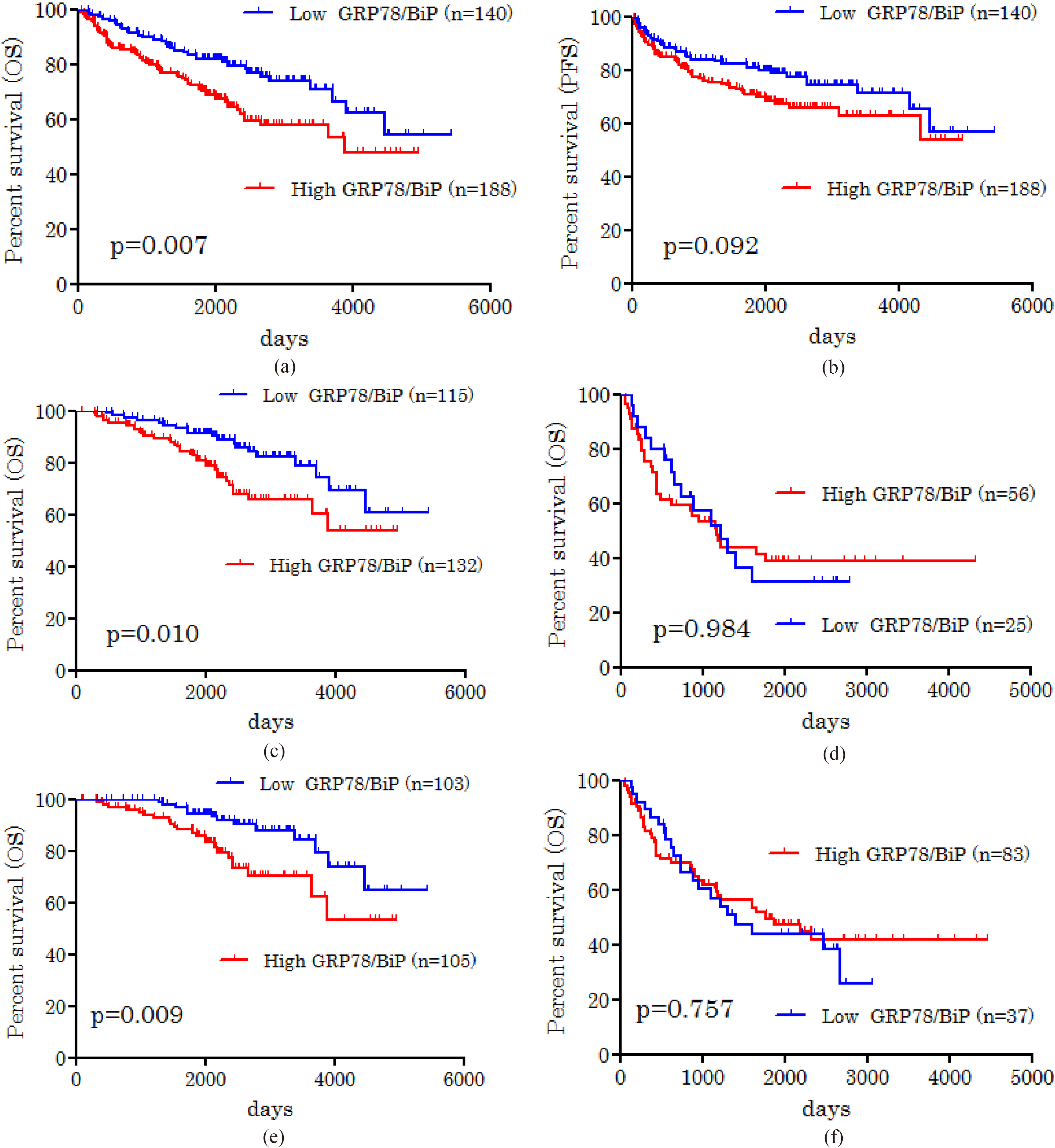
Next, we analyzed the prognostic significance of BiP/GRP78 expression according to different markers (Table 3). Increased expression of BiP/GRP78 was significantly associated with poor OS in patients with older age, female sex, early disease stage, T1-2 factor, well or moderately differentiated tumors, and negative vascular invasion, but not significantly associated with PFS according to any variables. We performed multivariate analysis of BiP/GRP78 expression in the group limited to the abovementioned 8 variables. Based on this analysis, elevated BiP/GRP78 expression was confirmed as an independent prognostic factor related to poor OS in the group of patients with GC with T1-2 factor (Table 4).
Univariate and multivariate survival analysis in all patients with T1 or 2
The present study was a clinicopathological analysis performed to evaluate the prognostic significance of BiP/GRP78 expression in patients with GC who underwent surgical resection as an initial treatment. We found that BiP/GRP78 was highly expressed in 57% of all patients and that high expression of BiP/GRP78 was significantly related to age, sex, disease staging, lymph node metastases, lymphatic permeation, vascular invasion, and shorter survival. Our results suggest that BiP/GRP78 plays a crucial role in the tumor progression and invasiveness of GC, correlating with worse survival. In particular, BiP/GRP78 expression was proven to be a significant predictor of prognosis in patients with older age, female sex, early disease stage, T1-2 factor, well or moderately differentiated tumors, and negative vascular invasion. The present study identified the increased expression of BiP/GRP78 as an independent factor for predicting poor OS in patients with T1-2 factor. It remains unclear why the expression level of BiP/GRP78 is important in the prediction of negative outcomes for patients with early-stage disease.
The current study focused on the prognostic role of BiP/GRP78 expression in patients with GC, and the prognostic features of BiP/GRP78 were elucidated in our analysis. In a previous study, BiP/GRP78 was detected in 64.7% of GC specimens (315/487), and was significantly linked to tumor size, lymphatic and vascular invasion, lymph node metastasis, and disease staging, but not with age or sex. Univariate analysis using the Kaplan-Meier method indicated that the survival rates of patients with GC with weak, moderate, or strong BiP/GRP78 expression were significantly lower than those in patients without BiP/GRP78 expression. BiP/GRP78 expression was not clearly identified as an independent prognostic factor for cumulative OS by multivariate analysis [13]. Another study reported that 163 (68.8%) of 237 patients with GC who underwent surgery exhibited BiP/GRP78-positive staining [14]. In this study, the increased BiP/GRP78 expression was reported to be closely associated with poor differentiation, advanced disease stage, infiltrative depth, and lymph node metastasis. Survival analysis was performed in comparison to 160 GC patients who received adjuvant chemotherapy, and high expression of BiP/GRP78 was associated with a significantly increased risk of recurrence. On multivariate analysis, BiP/GRP78 expression was confirmed as an independent factor associated with an increased likelihood of recurrence. The relationship between BiP/GRP78 expression and risk of recurrence was not significant in patients who were treated with adjuvant taxane-containing (paclitaxel or docetaxel) chemotherapy, but it was statistically significant in patients who did not receive taxane-containing chemotherapy. Moreover, in the group of patients with increased BiP/GRP78 expression, those receiving adjuvant taxane-containing chemotherapy experienced a significantly longer time to recurrence than those not receiving this therapy. The results of this study suggest that patients with BiP/GRP78 expression who were treated with adjuvant taxane-containing chemotherapy exhibited a lower risk of recurrence than those who did not undergo this adjuvant regimen [14]. The authors speculated that taxanes diminish the effect of BiP/GRP78 on the chemotherapy resistance mechanism; thus, a taxane-based regimen may be a good choice in patients with GC. Previous experimental studies had disclosed that therapeutics containing taxanes block ER prolongation and movement by inhibiting polymerization of new microtubules; therefore, taxane-containing chemotherapy could alter or disturb the function of BiP/GRP78, such as by preventing the translation or breakdown of misfolded proteins [17, 18]. In the present study, we confirmed that elevated BiP/GRP78 expression was closely linked to factors reflecting tumor aggressiveness and progression, such as advanced stage, lymph node metastasis, lymphatic and vascular invasion, and shorter survival, consistent with the results of previous studies. Although our evaluation and antibody use for BiP/GRP78 detection were markedly different from the methods of these previous studies, more than half of patients with GC revealed positive BiP/GRP78 staining in any of the studies. Interestingly, the presence of BiP/GRP78 expression was found to be important as a significant prognostic indicator for patients with early stage of disease or non-poorly differentiated tumors. In patients with T1 or 2 factor, in particular, BiP/GRP78 expression was identified as an independent prognostic factor linked to poor OS after surgery, regardless of adjuvant chemotherapy. Considering the results of these studies, including our investigation, taxane-based regimens as adjuvant chemotherapy may be useful to prolong OS in patients with GC with BiP/GRP78 expression and relatively early-stage disease who undergo surgery. Nowadays, taxane-based regimens are not administered as standard adjuvant chemotherapy; thus, BiP/GRP78 inhibitors have potential as a promising target in adjuvant treatment for such patients with GC. Further investigation is warranted to confirm the possibility of BiP/GRP78 inhibitors in the treatment of patients with GC.
As a clinical problem, there is controversy regarding the prognostic significance of BiP/GRP78 expression according to various types of cancer. Increased expression of BiP/GRP78 in patients with prostate cancer, renal cell carcinoma, neuroblastoma, GC, and hepatocellular carcinoma significantly correlated with poorer prognosis than its decreased expression, whereas, increased expression of BiP/GRP78 was associated with worse outcomes than its increased expression in patients with lung cancer and esophageal cancer [3, 5, 6, 7, 8, 9, 10, 11, 12]. In cases of head and neck cancers, one study reported that increased BiP/GRP78 expression was closely linked to advanced disease stage, metastases, and high-grade malignancy and was identified as a prognostic predictor of poor OS [5]. However, another study documented the following: (1) decreased BiP/GRP78 expression significantly correlated with advanced disease stage and lymph node metastasis, (2) strong BiP/GRP78 staining was observed in patients with early stage disease, and (3) patients with advanced disease stage showed weak BiP/GRP78 staining, suggesting that low-grade malignant cells are formed under ER stress conditions but high-grade malignant cells could overcome ER stress-induced apoptosis [7]. Although the sample sizes of these studies are limited for elucidation of the prognostic role of BiP/GRP78 and this may bias their results, it appears to be difficult to conclude how the expression level of BiP/GRP78 differs according to cancer types, disease staging, and the other factors.
In experimental studies, it has been shown that knockdown of BiP/GRP78 expression disturbed GC cell invasion, growth, and metastasis [10]. Fu et al. have shown that Akt phosphorylation, known as the major antiapoptotic and pro-proliferative signaling, is inhibited by the knockdown of BiP/GRP78, suggesting that the silencing of BiP/GRP78 expression is linked to the loss of PTEN tumor suppression and oncogenic Akt activation [19]. Moreover, it has been reported that BiP/GRP78-targeting peptides linked to specific agents induce cancer cell death and suppress tumor growth without affecting normal tissue [20, 21]. These studies support the hypothesis that the inhibition of BiP/GRP78 alternation could be a promising target in the treatment of several cancers. The induction of BiP/GRP78 activity is also shown to have potential as a novel target to combat drug resistant cells in lung cancer, bladder cancer, and breast cancer [3, 4, 10, 12]. Further research is needed to plan studies to explore the possibility of a targeted therapy of the BiP/GRP78 compound.
There are several limitations to the present study. One limitation is that this study did not include any patients with early stage disease who were candidates for endoscopic treatment or patients with advanced stage disease, such as inoperable cases, and thus the results of our study may not reflect the whole spectrum of characteristics of patients with GC. The tumor tissues obtained from endoscopic biopsy are sometimes inadequate for immunohistochemical staining. However, the role of BiP/GRP78 expression should be elucidated in patients with inoperable GC, and further study is needed to investigate the clinicopathological significance of BiP/GRP78 expression in patients with early- or advanced-stage disease or candidates for endoscopic diagnosis. Another limitation is that the antibody against BiP/GRP78 used in our study was different from that used in previous studies. We assessed the quality of BiP/GRP78 detection among several antibodies, and we believe that the antibody that we used against BiP/GRP78 in the present study is appropriate for examining the expression status of BiP/GRP78. Further research is warranted to investigate the prognostic role of BiP/GRP78 expression in patients with GC with utilization of the same antibody and immunohistochemical technique. Finally, it remains clear whether the risk factors such as Helicobacter pylori status, smoking, obesity, consumption of very hot food, skipping breakfast and alcoholism could affect the expression of BiP/GRP78. Because of our retrospective study including some limited data, we have no enough data about BiP/GRP78 expression and these risk factors. Moreover, little is known about the expression of BiP/GRP78 in familial GC or environmental GC. Further investigation is needed to evaluate the relationship between GRP78/BiP expression and several risk factors.
In conclusion, BiP/GRP78 is highly expressed in patients with GC and is significantly linked to tumor aggressiveness and progression. Increased expression of BiP/GRP78 was identified as an independent factor for predicting poor OS in patients with early-stage disease, especially T1-2 factor. The present study suggests that the inhibition of BiP/GRP78 could be a promising target for adjuvant chemotherapy in patients with GC who undergo surgical resection.
Conflict of interest
We (all authors) have no financial or personal relationships with other people or organizations that could inappropriately influence our work.
Footnotes
Acknowledgments
We appreciate Ms. Yuka Matsui for her technical assistance of manuscript submission. We also deeply appreciate Prof. Masahiko Nishiyama of Department of Molecular Pharmacology and Oncology, Gunma University Graduate School of Medicine, for the critical review of this manuscript.