
Abstract
OBJECTIVE:
This study was designed to evaluate the relation between GPx2 (glutathione peroxidase 2) expressions and clinicopathological features as well as prognosis of patients with nasopharyngeal carcinoma (NPC).
METHODS:
A total of 89 cases of NPC were investigated to examine the immunohistochemical expression of GPx2. Fourteen pairs of NPC and the control samples were analyzed respectively by qRT-PCR and Western blot. The correlations of GPx2 expressions with the clinicopathologic features and the prognosis of NPC patients were also analyzed.
RESULTS:
The expression of GPx2 in NPC tissues was elevated immunohistochemically when compared with normal nasopharyngeal tissues (
CONCLUSIONS:
GPx2 may play an important role in the development of nasopharyngeal carcinoma. Furthermore, GPx2 may serve as a prognostic biomarker for NPC patient.
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant neoplasm arising from the nasopharynx epithelium. It has obvious geographic and racial distribution. It is mainly reported in southern China, Southeast Asia, North and East Africa, the Middle East and Alaska [1, 2]. In southern China, the incidence rate is approximately 25–50 per 100,000 people, which is 100-fold higher than the western world [3, 4]. The development of NPC is related to both genetic and environmental factors. It has been confirmed that Epstein Barr Virus (EBV) infection is a risk factor for NPC as well as genetically controlled biological progresses such as oxidative stress [5, 6].
Oxidative stress is defined as the imbalance of free radicals, reactive oxygen species (ROS) and their elimination by protective mechanisms, such as antioxidants. It has been confirmed that cancer initiation and progression were linked to oxidative stress by increasing DNA mutations or inducing DNA damage, genome instability and cell proliferation [7]. As one member of antioxidants, glutathione peroxidase (GPX) can react with H
In this study, we detected the expressions of GPx2 both in NPC tissues and the normal nasopharyngeal tissues. Also, we analyzed the associations between expressions of GPx2 and clinicopathologic features, as well as metastasis of NPC.
Association of GPx2 expression and clinicopathologic features of 89 NPC patients
Association of GPx2 expression and clinicopathologic features of 89 NPC patients
Patients and materials
A total of 119 archived paraffin-embedded tissues were used for immunohistochemical analysis, including 89 NPC patients and 30 control cases. The case with chronic nasopharyngeal inflammation was defined as normal control. All tissues were obtained from the Pathology Department, the First Affiliated Hospital of Chongqing Medical University. The samples were collected by biopsy before any treatment was performed. Tumor and clinical stages were defined according to the criteria of the 2002 TNM Classification [18]. After confirmed as NPC, the patients received radiotherapy with or without chemotherapy from March 2006 to March 2013. The last follow-up of all patients ended at October 2013. Clinical features of patients and characteristics of tumor were shown in Table 1. For qRT-PCR and Western blot analysis, fourteen paired fresh specimens were collected randomly, frozen in liquid nitrogen immediately following biopsy and then maintained at
Immunohistochemistry
Results of GPx2 expression determined by immunohistochemistry
Results of GPx2 expression determined by immunohistochemistry
Before immunohistochemistry analysis, HE staining was performed to identify the NPC cancer cells. Immunohistochemistry analysis was performed by 2-step plus Poly-HRP anti-mouse/rabbit IgG detection system (Zhongshan Golden Bridge Bio-technology, Beijing, China). The slides were incubated successively with GPx2 antibody (dilution 1:30, sc-54604, Santa Cruz Biotechnology, CA, USA) for overnight. Sections were evaluated by two pathologists blindly. The following scoring system based on the percentage of positive cells and intensity was used to evaluate the GPx2 expressing. The percentage was scored as 0 (0–9% cells stained), 1 (10%–25%), 2 (26%–50%), 3 (51%–75%), and 4 (76%–100%). The intensity scored as follows: 0
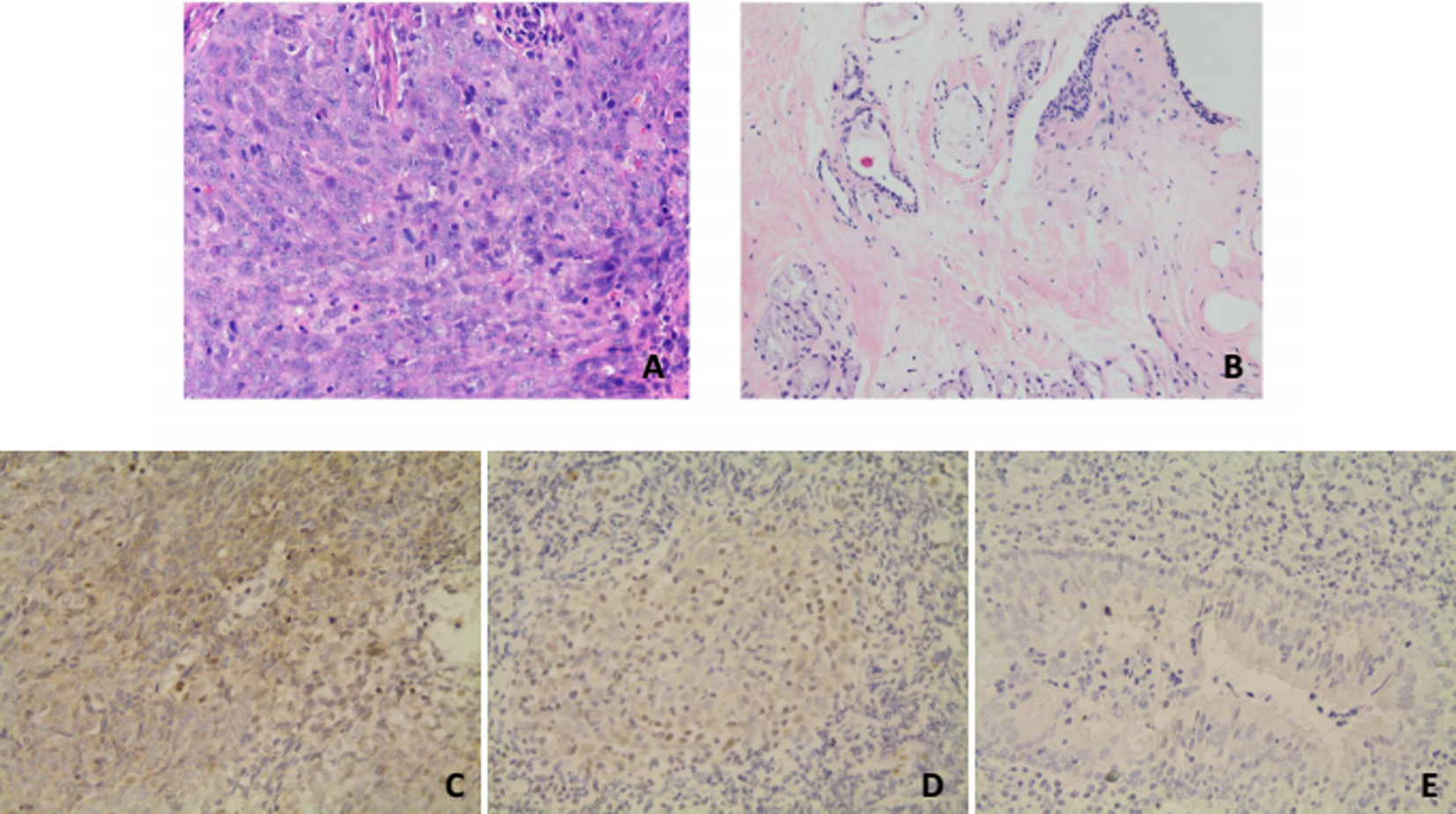
HE staining for NPC tissues (A) and normal nasopharyngeal tissues (B). Representative immunohistochemistry for NPC (high expression (C); light expression (D)) and normal nasopharyngeal tissues (E).
Total proteins from 7 pairs of fresh nasopharyngeal carcinoma and inflammation tissues were extracted using RIPA buffer (Beyotime Institute of Biotechnology, Nantong, China). The concentrations of protein were detected by BCA Protein Assay Kit (Beyotime Institute of Biotechnology, Nantong, China). The 15% sodium dodecyl sulfate polyacrylamide gel electrophoresis was used to separate protein samples. Then proteins on the gel were transferred to PVDF membranes. Membranes were incubated with GPx2 antibody (dilution 1:500, sc-54604, Santa Cruz Biotechnology, CA, USA).
QRT-PCR was performed by One-Step SYBR PrimeScript RT-PCR Kit II (Takara Biotechnology, Dalian, China) following the supplied protocol. Total RNA from 7 pairs of specimens was extracted by Trizol (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s instructions. Total RNA was then reverse transcribed into cDNA. GAPDH was used as the internal standard in qRT-PCR system. Then GPx2 and GADPH expressions were analyzed in a LightCycler 480 qRT-PCR system (Bio-RAD CFX96, Hercules, CA, USA) with SYBR Premix Ex Taq (Takara Biotechnology). The PCR primers for GPx2 were: 5
Statistic analysis
All statistical analyses were performed by SPASS 21.0 statistics. Data shown as
Results of logistic regression exploring the effects of covariates on clinical stage
Results of logistic regression exploring the effects of covariates on clinical stage
Prognosic factors for metastasis of 89 patients with NPC by Cox regression analysis
Expression of GPx2 in nasopharyngeal carcinoma as determined by immunohistochemistry
Totally 89 nasopharyngeal carcinoma patients and 30 nasopharyngeal inflammation tissues were analyzed. Results were shown in Table 2. Representative examples of staining are shown in Fig. 1, indicating that nasopharyngeal carcinoma samples have strong cytoplast GPx2. Among 89 cases of nasopharyngeal carcinoma, 53 cases had strong staining and 36 cases had light staining. While in 30 control cases, 28 cases had light staining and 2 cases had strong staining, which demonstrated that GPx2 was over expressed in nasopharyngeal carcinoma (
GPx2 mRNA expression in NPC patients and the controls (*
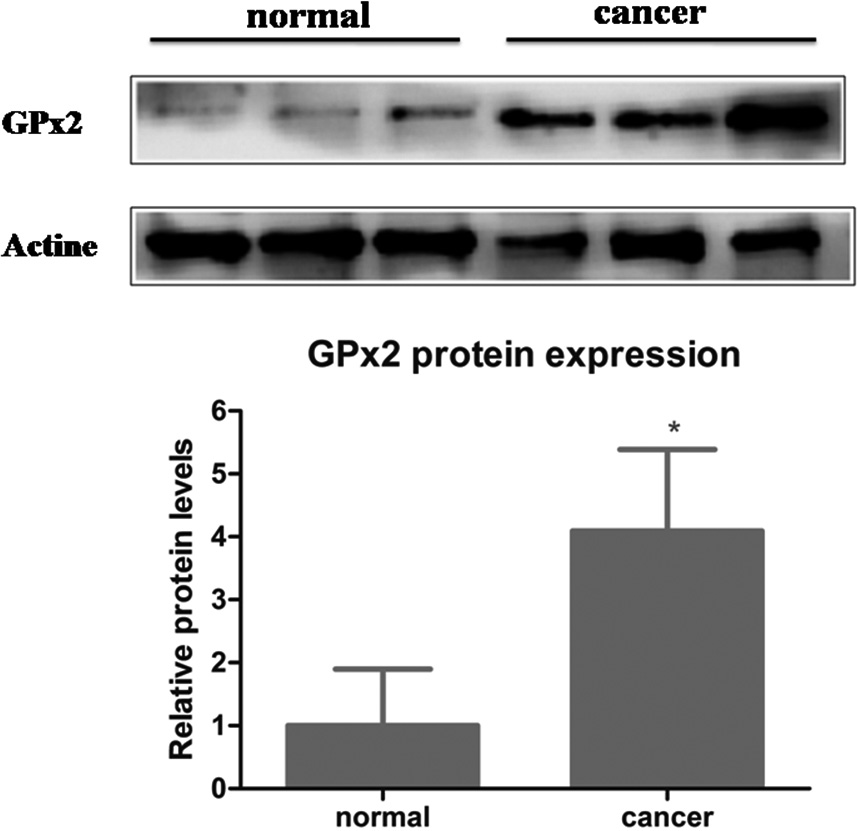
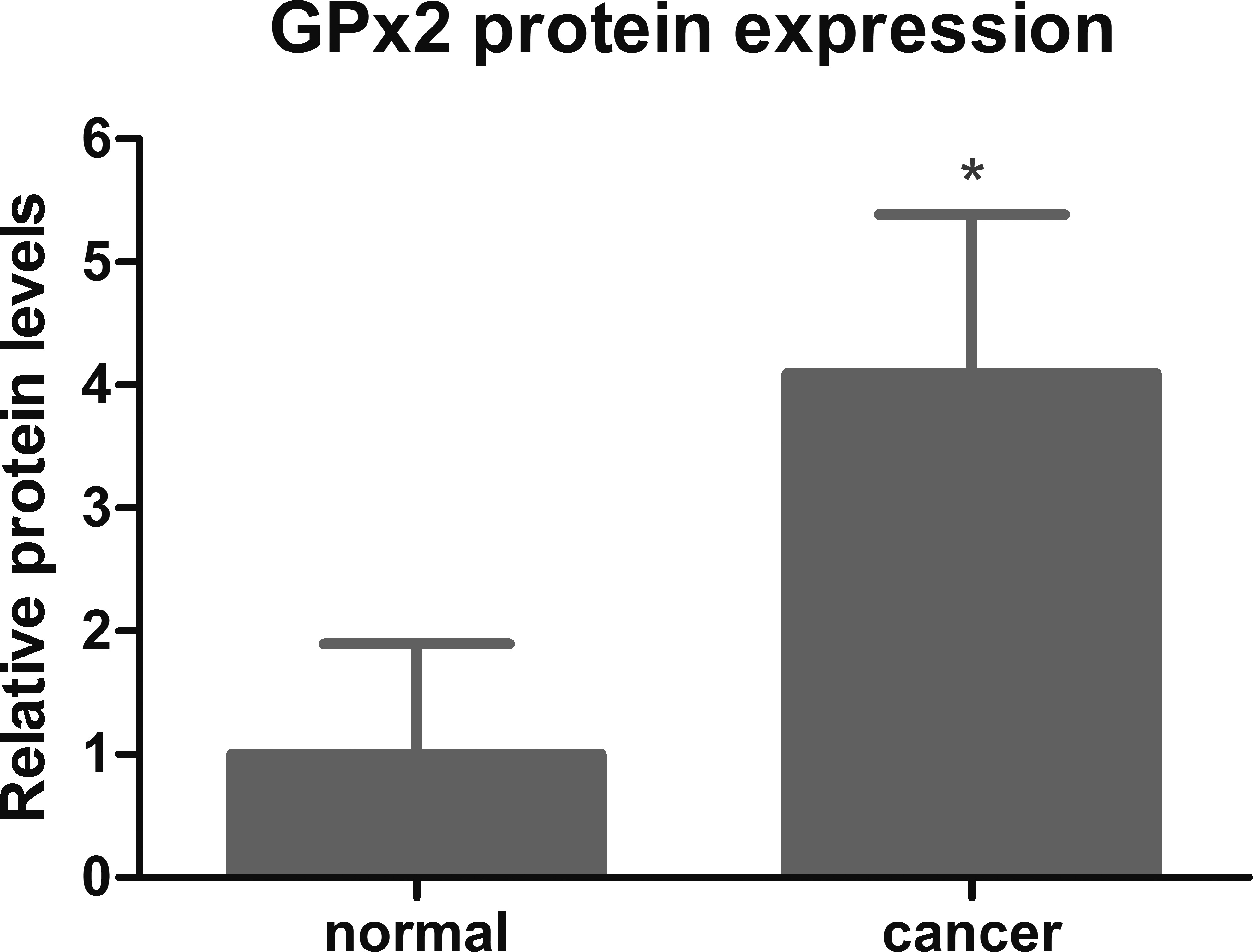
GPx2 protein expression in NPC patients and the controls (*
Seven pairs of nasopharyngeal carcinoma and the control samples were analyzed respectively. Mean age of patients for qRT-PCR analysis was (42.9
Relation between GPx2 expression and clinicopathologic features
Table 1 shows the association between GPx2 expression and the clinicalpathologic features of nasopharyngeal carcinoma patients. Statistical analysis showed GPx2 expression was significantly higher in the late clinical stage (
Logistic regression analysis showed that GPx2 expression was the only statistically significant predictor for clinical stage (Table 3).
To investigate whether GPx2 expression was associated with metastasis, Cox regression analysis was performed. Both univariate analysis and multivariate analysis revealed that there was no significant relation between GPx2 expression and the metastasis (Table 4).
Discussion
The present study showed that GPx2 was clearly detected in the cytoplasm of cancer cells of NPC tissues immunohistochemically. Also,
The shift in the balance between ROS and biological antioxidative response plays a vital role in tumor progression. ROS such as superoxide anion (O
GPx2 can act as the prevention of metastasis in tumor. It was reported that GPx2 knockdown cells had a higher capability to migrate and invade than the GPx2-expressing controls [34]. Interestingly, the GPx2 promoter is activated by
In conclusion, our data demonstrated that GPx2 was elevated in NPC and may play an important role in the development of NPC through the regulation of ROS. Furthermore, higher GPx2 expression was associated with late stage of tumor, indicating that GPx2 may serve as a prognostic biomarker for NPC patient.