
Abstract
Background:
Over the past 5 years, many studies have reported the prognostic value of hypoxia-inducible factor-1 alpha (HIF-1α) in nasopharyngeal carcinoma. However, the results have not reached a consensus until now. Therefore, we performed this meta-analysis to investigate the influence of HIF-1α expression on the prognosis and clinical characteristics in nasopharyngeal carcinoma.
Methods:
We searched PubMed, the Cochrane Library, Embase (via Ovid interface), Web of Science, and China National Knowledge Infrastructure electronic databases from their establishment to 6 December 2017. We calculated the hazard ratio (HR) and the odds ratio (OR) to assess the prognostic and clinicopathological values of HIF-1α, respectively. Q test and I2 statistic were applied to evaluate heterogeneity. We also conducted publication bias and sensitivity analyses.
Results:
A total of 18 studies with 1476 patients were included in our meta-analysis. We found HIF-1α expression was associated with poor overall survival (HR=1.77; 95% confidence interval (CI) 1.35, 2.32; P<0.001), poor progression-free survival (HR=1.72; 95% CI 1.22, 2.44; P=0.002), a higher rate of lymph node metastasis (OR=3.81; 95% CI 2.60, 5.58, P<0.001), and more advanced tumor stage (OR=2.98; 95% CI 1.79, 4.97; P<0.001).
Conclusions:
Our study demonstrated that HIF-1α could be an appropriate prognostic biomarker for nasopharyngeal carcinoma patients.
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor originating from the nasopharynx epithelium. According to the World Health Organization pathological classification, 1 NPC includes three subtypes; namely keratinizing squamous cell carcinoma, non-keratinizing carcinoma (differentiated and undifferentiated), and basaloid-squamous carcinoma. Among them, non-keratinizing carcinoma is the most common subtype. Regional prevalence is the most distinct characteristic of NPC. The incidence rate of NPC in South China and Southeast Asia is at least twice as high than that in every other area. 2 More than 60% of new cases are diagnosed in China. 3 Currently, the standard treatment for NPC is radiotherapy with or without chemotherapy. 4 Despite developments in treatment, survival of advanced NPC is still poor because of locoregional failure, recurrence, and distant metastasis,5-7 while satisfying prognostic indicators are still unavailable. Although some prognostic markers, including plasma Epstein–Barr virus (EBV) DNA, 8 tumor, node, metastasis (TNM) stage, 9 C-reactive protein, 10 and lactate dehydrogenase, 11 are reported to be related to the prognosis of NPC, they fail to be accurate enough for evaluating the survival outcomes. The value of plasma EBV DNA is limited by a substantial false positive rate and a lack of a universal cut-off value,8,12,13 and the TNM stage is unable to reflect biological heterogeneity. 14 Patients at the same stage have shown various survival outcomes. Inter-laboratory variability and low specificity have limited the application of C-reactive protein and lactate dehydrogenase in clinical practice.15,16 Therefore, a specific and effective prognostic biomarker is expected by clinicians to optimize a treatment strategy for NPC patients.
An important transcriptional factor subunit hypoxia-inducible factor-1 alpha (HIF-1α) has been found to be associated with cellular response to the hypoxia microenvironment, which usually presents in solid tumors. 17 Under a hypoxia condition, HIF-1α activates a series of genes involved in the regulation of malignant biological behaviors. It has been reported that expression of HIF-1α promotes tumor cell proliferation, invasion, migration, and resistance to radiotherapy.18,19 Numerous studies have confirmed that HIF-1α expression is related to poor survival in various cancers, such as esophageal carcinoma, 20 oral squamous cell carcinoma, 21 and lung cancer. 22
However, the prognostic value of HIF-1α expression in NPC has not been clearly elucidated until now. Therefore, this study conducted a meta-analysis to investigate the prognostic and clinicopathological value of HIF-1α expression in patients with NPC.
Materials and methods
Search strategy
A comprehensive literature search was conducted in PubMed, the Cochrane Library, Embase (via Ovid interface), Web of Science, and China National Knowledge Infrastructure (CNKI). The final search was conducted on 6 December 2017. The search syntax was ((“HIF-1” [All Fields] OR “hypoxia-inducible factor-1” [All Fields]) AND (“nasopharyngeal carcinoma” [All Fields] or “nasopharyngeal cancer” [All Fields] or “NPC” [All Fields])). There was no restriction to language in our search. The reference lists of relevant articles were manually searched for potential eligible studies.
Inclusion and exclusion criteria
Studies were considered eligible if they met the following inclusion criteria: (a) NPC patients were confirmed by histopathological diagnosis and had no other malignances; (b) the results were focused on the relationship between HIF-1α expression and survival outcomes or clinical characteristics of NPC patients; (c) available information was provided to estimate hazard ratio (HR) and odds ratio (OR) with 95% confidence intervals (CIs) for prognosis or clinical characteristics. Studies were excluded if: (a) they were reviews, letters, case reports, comments and conference abstracts; (b) they were duplicate publications; (c) they were non-human studies; (d) the HRs or ORs with their 95% CIs were not reported or could not be computed. When studies with overlapping patients were identified, we only included the study with the most patients. Two investigators (WX and LL) evaluated the identified studies independently. Any disagreement was discussed to reach a consensus.
Data extraction and quality assessment
Data were extracted by two investigators (WX and HH) independently. The following required information was drawn from each included study: first author, publication year, country of patients, number of patients, follow-up time, information of clinical characteristics (gender, age, lymph node metastasis, distant metastasis, recurrence, stage), study design, HR, and 95% CI for survival, Kaplan–Meier curves for survival, definition of HIF-1α expression, and positive rate of HIF-1α. The Newcastle–Ottawa Scale (NOS) was applied to assess each included study’s quality. Studies with 6 points or more on NOS were deemed as high-quality studies.
Statistics analysis
To evaluate the prognostic significance of HIF-1α expression, HRs with 95% CIs were used to calculate the pooled HR. If the HRs and 95% CIs were not directly extracted, we calculated them from Kaplan–Meier curves or correlative outcome data. A heterogeneity test was conducted using the Q test and I2 statistic. When P>0.1 and I2<50%, which suggested no significant heterogeneity, the fixed-effects model would be used to calculate the estimate. Otherwise, the random-effects model would be used. To assess the heterogeneity sources, the subgroup analyses would be conducted. Meanwhile, Egger’s test and Begg’s test were applied to calculate publication bias. Additionally, we conducted a sensitivity analysis to assess the stability of the results. All statistical analyses were conducted by STATA 12.0 (STATA Corporation, College Station, TX, USA).
Results
Literature selection and characteristics
A total of 205 studies were retrieved initially after duplicates were removed. After reading the titles and abstracts, we excluded 169 because they were reviews, conference abstracts, case reports, cell or animal experiments, or unrelated research. After reading the full text, 18 studies were ruled out because HRs or ORs with 95% CIs were not reported or could not be computed from those papers. As a result, a total of 18 studies with 1476 patients were included in the current meta-analysis.23-40 The main characteristics of the 18 eligible studies are presented in Table 1. All the included studies were published from 2002 to 2017. Of the 18 studies, 16 were retrospectively designed and 2 prospectively designed. Only 1 study’s patients were from Japan, the rest were from China. There were 9 studies reporting the relationship between overall survival (OS) and HIF-1α expression, and the progression-free survival (PFS) was analyzed in 5 studies. In all studies, immunohistochemistry (IHC) was used to detect the expression of HIF-1α in the tumors. The NOS was applied to assess the quality of each study, and the mean score of included studies was 7.1 (range 6–9).
The main characteristics of included studies.
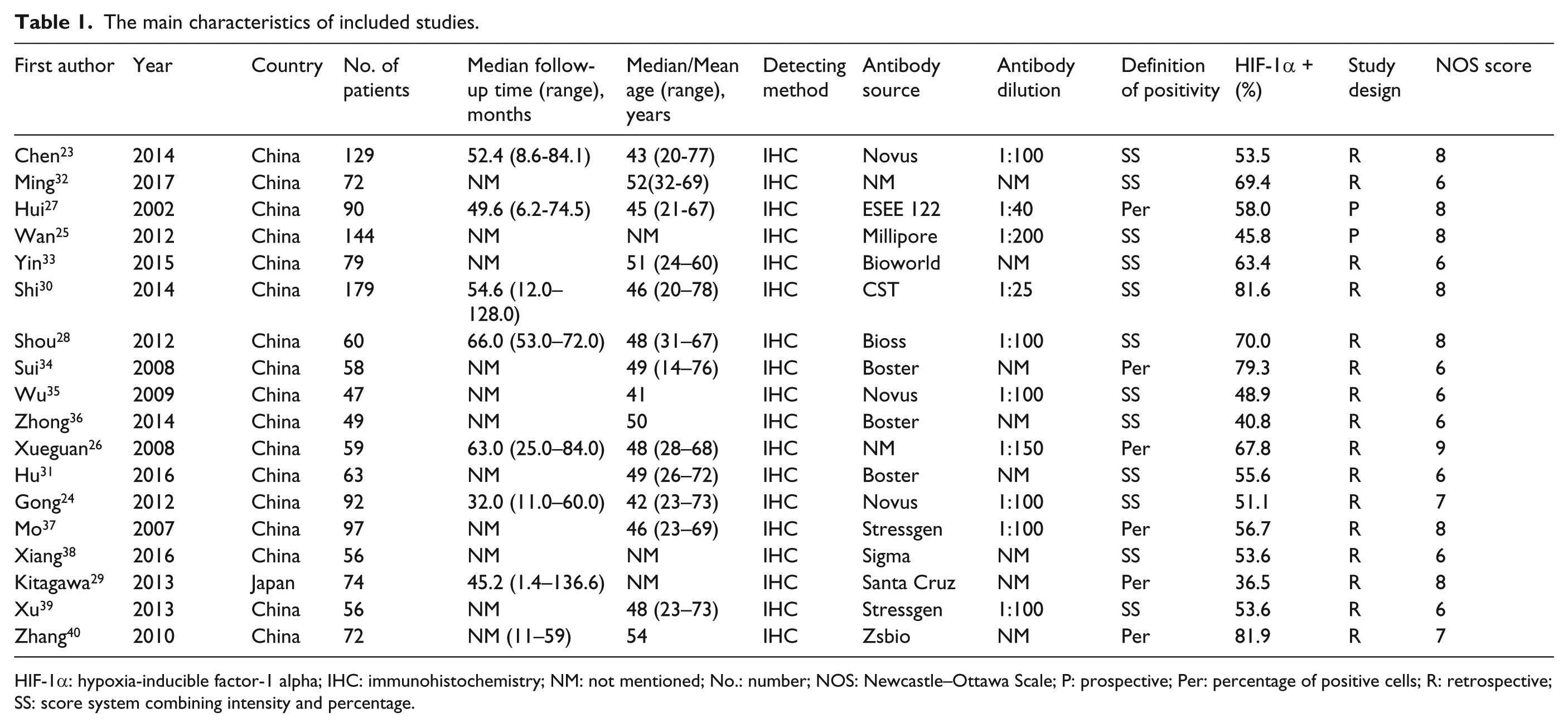
HIF-1α: hypoxia-inducible factor-1 alpha; IHC: immunohistochemistry; NM: not mentioned; No.: number; NOS: Newcastle–Ottawa Scale; P: prospective; Per: percentage of positive cells; R: retrospective; SS: score system combining intensity and percentage.
HIF-1α and survival
The analysis of OS included nine studies23-31 with 890 patients. The heterogeneity test showed no significance (I2=0.0%; P=0.566); however, we found a significant relationship between HIF-1α and OS. The expression of HIF-1α was related to shorter OS for NPC patients in a fixed-effects model (HR=1.94; 95% CI 1.46, 2.59; P<0.001) (Figure 1(a)). In addition, a subgroup analysis was performed by the study design. HIF-1α was strongly associated with poor OS in retrospective studies (HR=2.18; 95% CI 1.53, 3.10; P<0.001), but not in prospective studies (HR=1.56; 95% CI 0.95, 2.54; P=0.076).
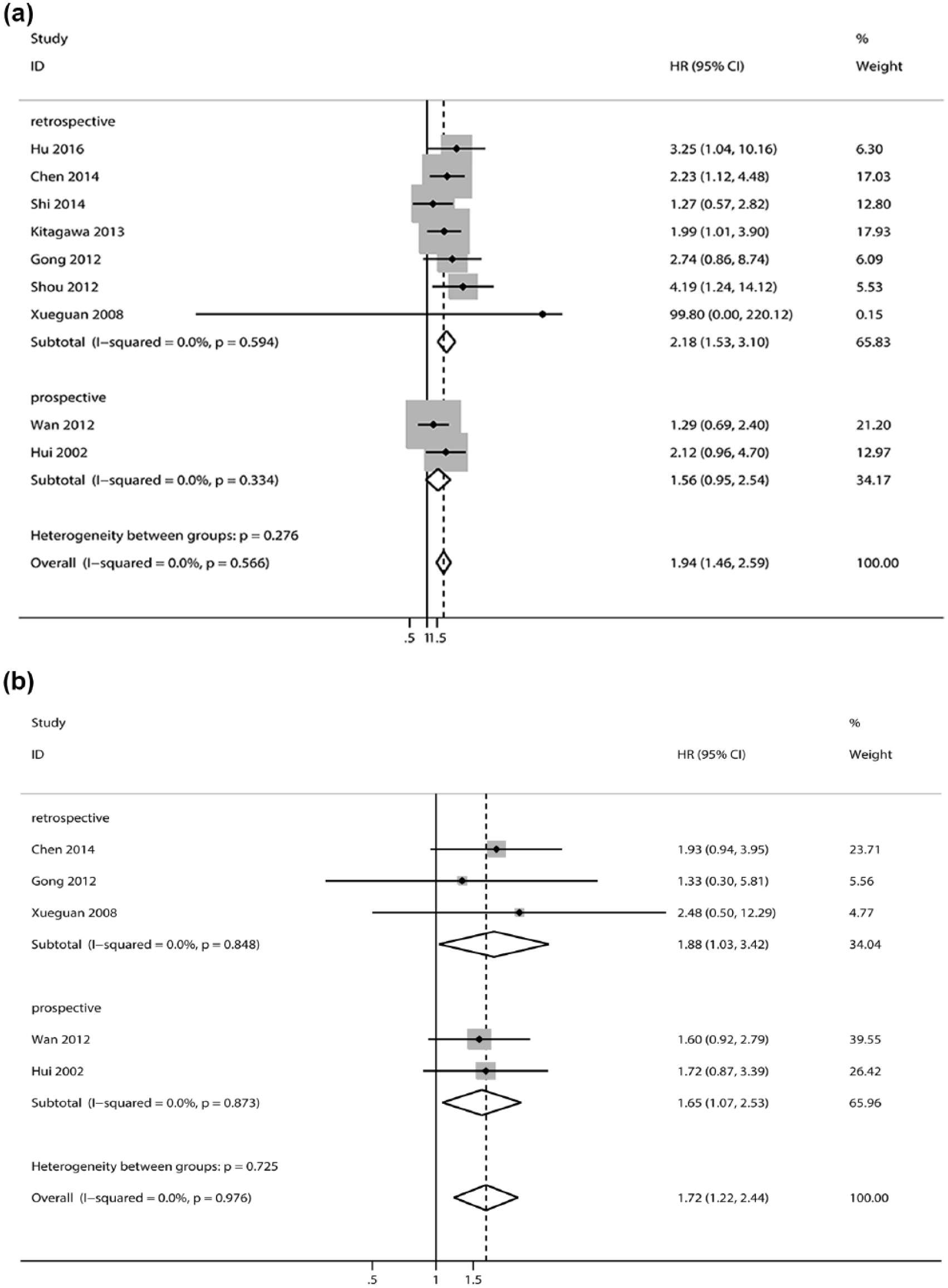
The association between HIF-1α and overall survival (a) and progression-free survival (b).
In the analysis of PFS, a total of five studies23-27 with 514 patients were included. The heterogeneity test showed no significance (I2=0.0%; P=0.976). The analysis also showed a significant relationship between HIF-1α and PFS in the fixed-effects model. A decreased PFS was associated with HIF-1α expression (HR=1.72; 95% CI 1.22, 2.44; P=0.002) (Figure 1(b)). Significant associations were detected both in retrospective studies (HR=1.88; 95% CI 1.03, 3.42, P=0.039) and in prospective studies (HR=1.65; 95% CI 1.07, 2.53; P=0.023).
HIF-1α and clinical characteristics
We also investigated the relationship between HIF-1α and clinical characteristics. For lymph node metastasis, 11 studies23,24,26,29,31,33-35,37-39 with 810 patients were included. The result suggested a significant association between HIF-1α expression and lymph node metastasis (OR=3.81; 95% CI 2.60, 5.58; P<0.001). For the tumor stage, 15 studies23,24,26,28,29,31-40 with 1063 patients were included. We detected that HIF-1α expression was associated with tumor stage (OR=2.98; 95% CI 1.79, 4.97, P<0.001). However, we did not observe that HIF-1α expression was significantly associated with gender, local recurrence, or distant metastasis. Table 2 shows these results.
The pooled data on clinical characteristics of included studies.
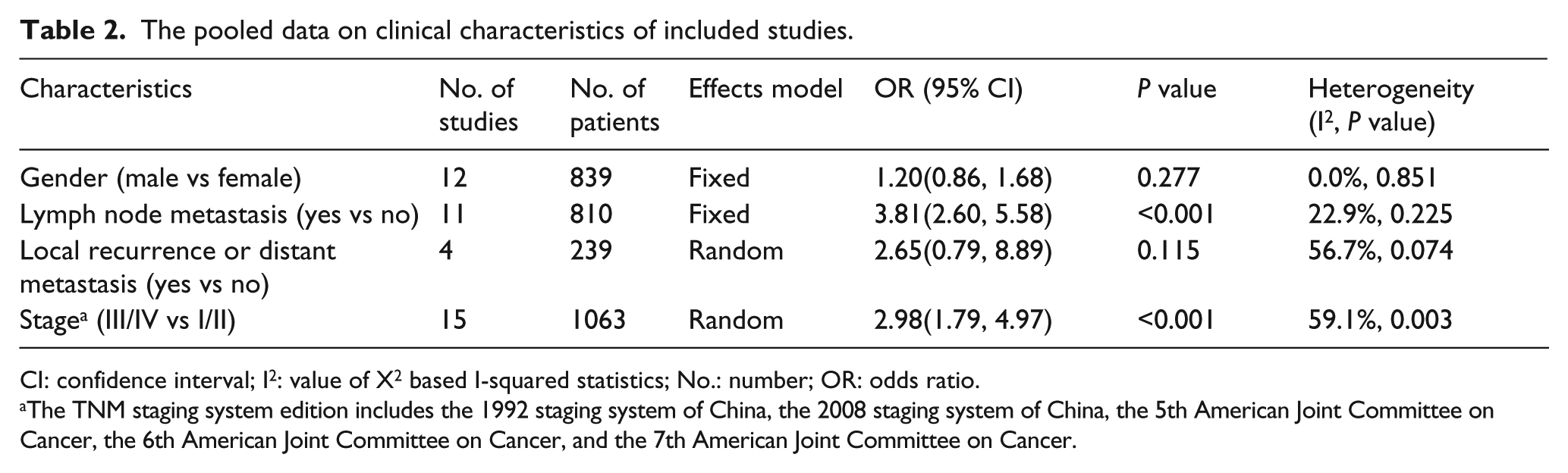
CI: confidence interval; I2: value of X2 based I-squared statistics; No.: number; OR: odds ratio.
The TNM staging system edition includes the 1992 staging system of China, the 2008 staging system of China, the 5th American Joint Committee on Cancer, the 6th American Joint Committee on Cancer, and the 7th American Joint Committee on Cancer.
Sensitivity analysis and publication bias
We conducted sensitivity analyses of OS and PFS to estimate variations. There were no significant variations in the results, which suggests their stability (Figure 2). Publication bias was detected in OS (Begg’s test Pr>|z|=0.016, Egger’s test P>|t|=0.025). Therefore, we used a trim and fill method to evaluate the asymmetry in the funnel plot. The result had not materially changed (HR=1.77; 95% CI 1.35, 2.32; P<0.001) (Figure 3(a)). We did not find any significant publication bias in PFS (Begg’s test Pr>|z|=0.462, Egger’s test P>|t|=0.674) (Figure 3(b)).
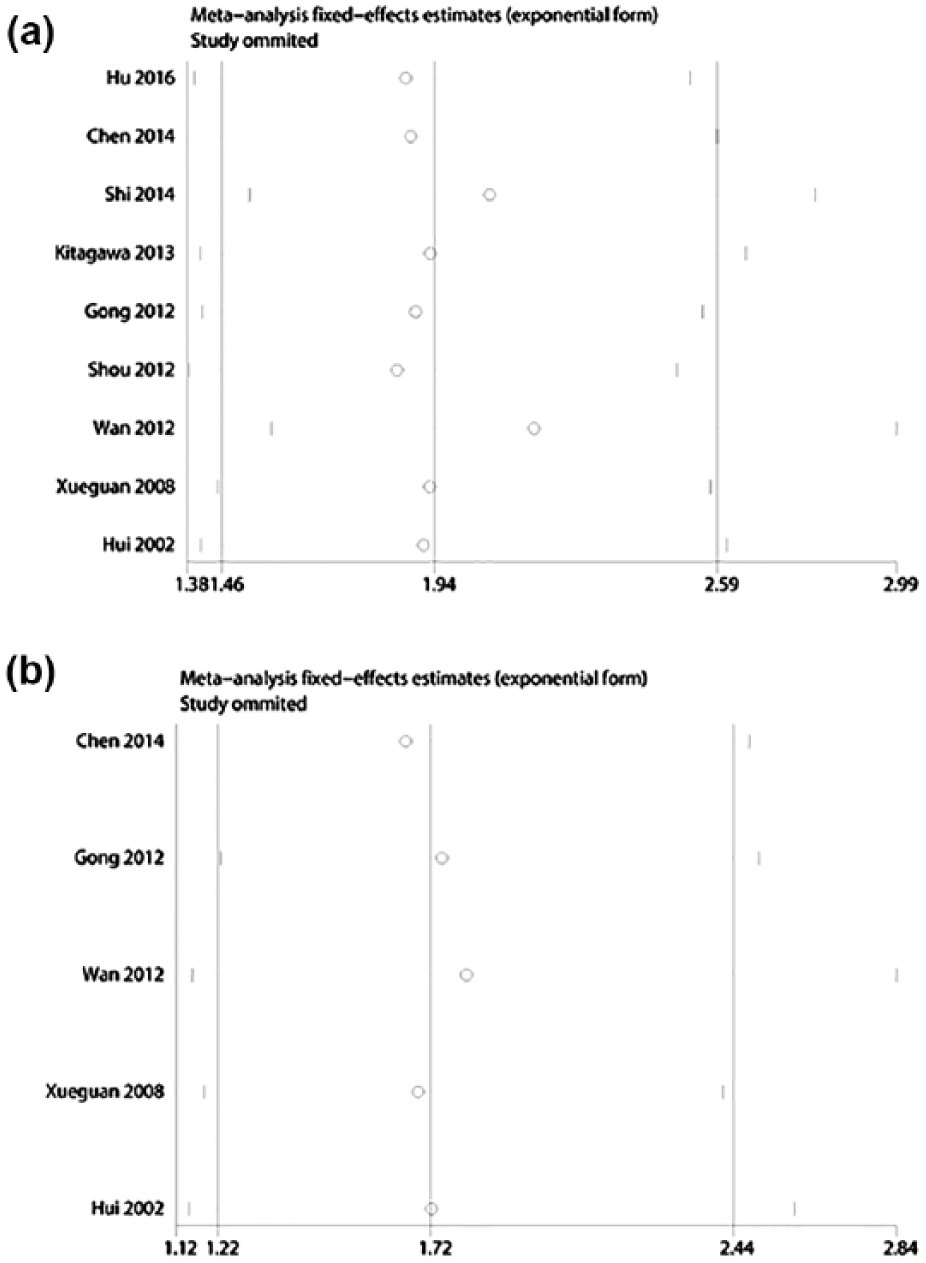
Sensitivity analysis of the effect of HIF-1α expression on overall survival (a) and progression-free survival (b).
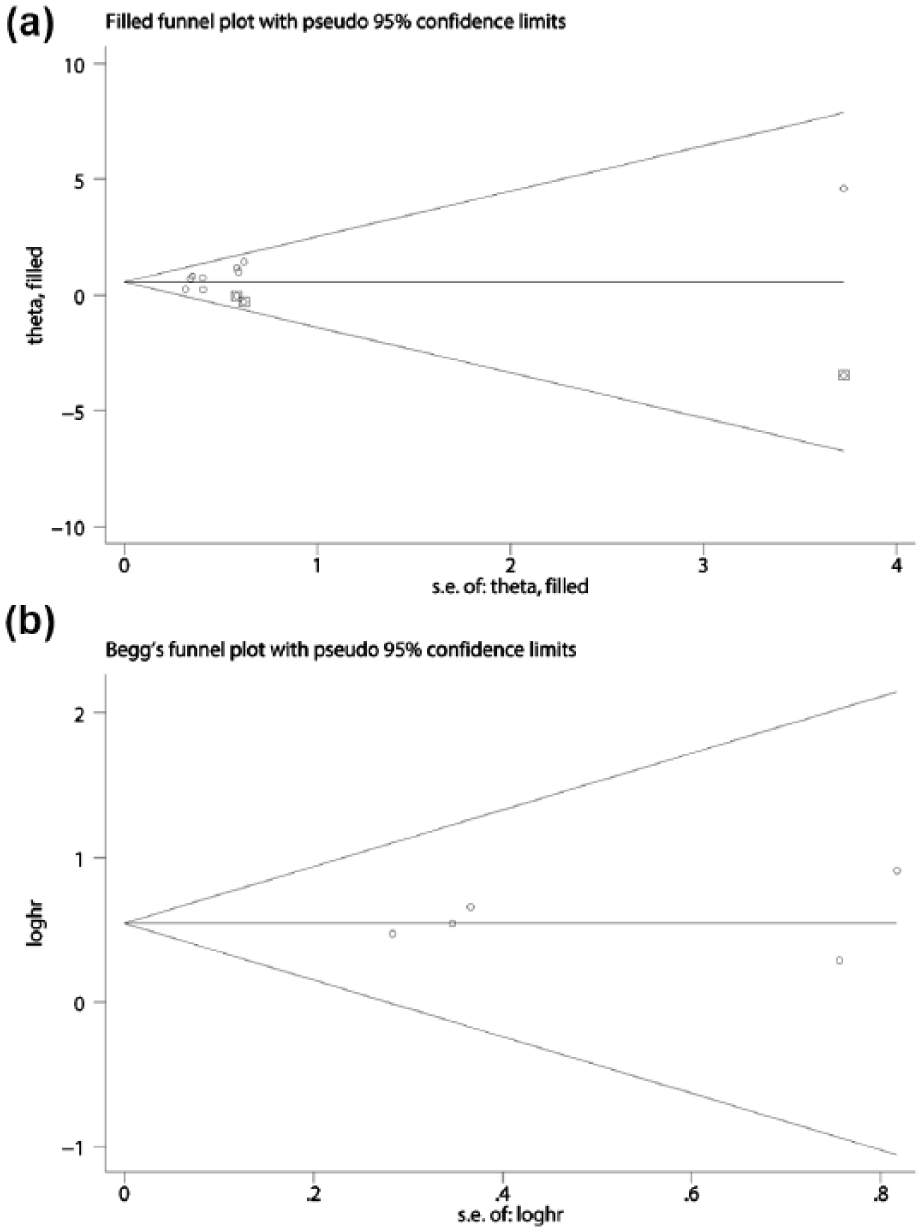
Publication bias on overall survival ((a) after the trim and fill method) and progression-free survival (b).
Discussion
In this meta-analysis, HIF-1α was indicated by the pooled data as an appropriate prognostic biomarker for NPC patients. We found that HIF-1α expression was strongly associated with poor OS and poor PFS in NPC. However, when the analysis was limited to the prospective subgroup, the HIF-1α expression was not related to OS. A possible cause for this discrepancy might be the limited number of prospective studies included. Hence, future large prospective studies are needed to validate our findings.
Our research was in line with many previous meta-analyses investigating the prognostic significance of HIF-1α in other tumors, such as esophageal carcinoma, 20 oral squamous cell carcinoma, 21 lung cancer, 22 glioma, 41 etc. All these studies had demonstrated that HIF-1α expression was correlated with poor prognosis. In addition, Gong et al. 42 published a systematic review on HIF-1α with prognostic value in head and neck cancer patients. In their review, five studies with 445 NPC patients were included, and HIF-1α was found to be associated with poor OS (HR=2.07; 95% CI 1.23, 3.49), a result which was in agreement with ours. However, compared to our study, the review by Gong failed to illustrate the correlation between HIF-1α and PFS, or to report the clinicopathological value of HIF-1α. Therefore, due to a larger sample size (1476 patients were included in our research) and more detailed analyses, our meta-analysis is superior to the previous study. We also explored the correlation between HIF-1α and clinicopathological features and found that HIF-1α was associated with a higher rate of lymph node metastasis and a more advanced tumor stage.
According to the meta-analysis, HIF-1α was not related to local recurrence or distant metastases but it was related to poor prognosis. A possible explanation for this might be that HIF-1α plays an important role in treatment resistance. 43 In a hypoxic environment, the degradation of HIF-1α is inhibited 44 and the downstream multidrug resistance 1 genes, also known as ATP binding cassette subfamily G member 1, is activated and results in a decrease of intracellular chemotherapeutic drug accumulation. 45 Sasabe et al. 46 reported that HIF-1α up-regulates antiapoptotic protein Bcl-XL and Bcl-2, and down-regulates pro-apoptotic protein Bak and Bax. Therefore, the effect of cytotoxic drugs is weakened. Apart from chemo-resistance, radio-resistance is also associated with HIF-1α. 47 It has been reported that HIF-1α suppresses mitochondrial biogenesis and respiration by down-regulating the level of c-Myc.48-50 As a result, a less reactive oxygen species is generated or accumulated. 19 A reactive oxygen species has been reported leading to DNA damage and cell apoptosis in irradiated cells.43,51 In this way, HIF-1α reduces the radio-sensitivity. Accordingly, HIF-1α inhibitors combined with radiotherapy are expected to be able to overcome the problem of radio resistance.52,53 For instance, the PX-478, which is an HIF-1α inhibitor, enhances sensitivity to radiation in vitro 54 and in vivo. 55 Therefore, it is believed that HIF-1α might be a promising marker and a potential target for survival prediction and individual therapy.
On the other hand, HIF-1α is up-regulated by EBV latent membrane protein 1 and is involved in EBV-mediated tumorigenesis. 56 It is now generally recognized that EBV is associated with NPC. 1 Wang et al. 57 have reported that plasma EBV DNA levels might be an effective prognostic marker for NPC patients. Both pretreatment EBV DNA and posttreatment EBV DNA could predict poor survival outcomes. 13 However, a consensus of the best cut-off value of EBV DNA has not been reached until now. Different cut-off values, such as 0 copy/mL, 58 1000 copy/mL, 59 and 8000 copy/mL, 60 have been reported in some studies. As the substantial false positive rate limits the value of plasma EBV DNA, 8 HIF-1α combined with EBV DNA might be more reliable in predicting the prognosis.
There were some limitations in our study. First, we detected a publication bias in OS. A possible explanation for this was that the included studies (n=9) were in a comparatively small number. 61 After the trim and fill method, the HR changed slightly but remained significant. Second, some studies did not offer HRs directly; we calculated HRs from the Kaplan–Meier curves. These facts may have influenced the precision of the results. Third, although significant heterogeneity was not observed in the analyses of OS and PFS, some potential problems should be noted, such as follow-up time, antibody source, antibody dilution, the definition of positive expression, and the positive rate of HIF-1α.
In summary, our meta-analysis has demonstrated that HIF-1α expression predicts a poor survival of NPC. Thus, HIF-1α might be a valuable biological marker in prognostic prediction and targeted therapy. However, further prospective studies are required to confirm our findings.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.