
Abstract
In the mid-1990s, a number of key publications and meetings of experts identified major technical issues associated with prosthetic technologies intended for developing countries. These included inadequate durability of prosthetic feet, poor socket quality and prosthetic fit, improper alignment of prostheses, and inferior function of components. To examine the progress that has been made since then in addressing these issues, a comprehensive review of literature was performed. In total, 106 articles were selected and included in the review. The review examined prosthetic technologies categorized into feet and ankles, knees, sockets and suspension, and matehals, structures, and alignment methods. Moreover, publications were categorized as technical development, clinical (lab-based) testing, or clinical field testing studies. The results reveal important work that has been carried out to develop and implement standardized outcome measures during field testing, allowing various existing prosthetic technologies to be evaluated in terms of their use, function, durability, and other factors. Progress has also been made toward addressing the aforementioned limitations of prosthetic technologies, however, more research and development is required. This includes improving the durability of the external cosmetic features of prosthetic feet, developing more functional prosthetic knee joints, and simplifying fabrication techniques to further improve outcomes associated with socket fit and prosthetic alignment. Research and development collaborations between developed and developing countries, and the dissemination of ongoing research, development, and evaluation activities are essential to the advancement of prosthetic technologies in these regions.
Introduction
In the mid-1990s, a number of key publications elucidated and documented prosthetic rehabilitation in developing countries, also commonly referred to as under developed, non industrialized, low-income or third world countries or nations. These publications helped to identify the deficits in prosthetic services in these nations, and more importantly the steps that would be needed to improve existing practices. 1–8 At that time, key issues relating to prosthetic practices and technologies included poor prosthetic durability and comfort; the former being primarily associated with the premature failure of prosthetic feet, 2,3,5,7 While the latter being due to inadequate prosthetic socket fit, 4,5,7 poor prosthetic alignment 4 and poorly functioning components, including knee joints. 8 Acceptable prosthetic durability and comfort are critical for the effective utilization of prostheses, for the simple reasons that broken prostheses that cannot be readily repaired are not useful, and ones that are highly uncomfortable to use (resulting in stump pain and skin breakdowns, highly fatiguing gait or back problems etc.) are likely to become underutilized or abandoned altogether. Furthermore, the need to develop standardized procedures and outcome measures to better evaluate and compare technologies, so that existing technologies could be improved and/or better utilized, was also recongnized. 2–4
The primary areas of focus have since been on establishing programs for prosthetic services, including the training of qualified personnel, but also the determination and provision of prosthetic technologies deemed to be appropriate for these developing regions. 3,5 Follow-up meetings and publications such as the 2001 International Society for Prosthetics and Orthotics (ISPO) consensus conference have since stressed “the urgent need for research, development and evaluation activities in relation to appropriate orthopaedic technology” where “appropriate technology is a system providing proper fit and alignment based on sound biomechanical principles which suit the needs of the individual and can be sustained by the country at the most economical and affordable price”. 9
In order to better understand and evaluate recent progress and achievements that have been made in this regard, we performed a comprehensive review of the literature, presented in this paper. The goal of this review was to provide information about the prosthetic technologies and related research, development and evaluation activities that have been published since the previous literature review. A further goal of this review was to assess and summarize the amount and type of work that has been done since 1994 (the previous review), that actually dealt with the problems that were identified at that time. However, for those interested in a review of prosthetic technologies prior to 1994, the full list of reviewed literature along with a number of reports and papers, can be found in the report of the ISPO consensus conference on appropriate prosthetic technology for developing countries, 1 and further summarized within three key articles. 2,3,5
Methods
A literature search was performed through Medline, CINAHL, EMBASE, EBM Reviews and RECAL using a combination of subject heading and text word search strategy outlined in Table I for Medline. No language restrictions were applied. The strategy was adapted for use with the other databases. Searches were performed covering the period of the earliest date of each database through December 2009. Since research and development activities from developing countries may not necessarily be disseminated in peer-reviewed journals, secondary sources were also reviewed. These included conference proceedings, organizational reports, newsletters, media stories and information from websites found via internet searches. Moreover, the cited references in reviewed articles were examined.
Given the diversity of articles (i.e., in terms of study designs, quality of reporting etc.) and so as not to exclude potentially relevant studies, the following broad selection criteria were applied. The two conditions for including an article were that: (i) The article must relate to major lower-limb amputations, and (ii), it must relate to, or at least provide some information on prosthetic technologies. The screening was performed by reviewing titles and abstracts, and where the abstract did not provide sufficient information to make this determination, the full text was reviewed. In summary, articles were excluded if they did not pertain to major lower-limb amputations (i.e., implantable or endoprostheses, upper-limb prostheses) or did not report on a technology or technology-related aspect of amputation and/or prostheses. In large part, the excluded articles were articles reporting solely on epidemiological studies and medical subject matter such as surgery and the prevention of diabetic foot.
Search strategy used for Medline (OVID) and adapted for other databases.
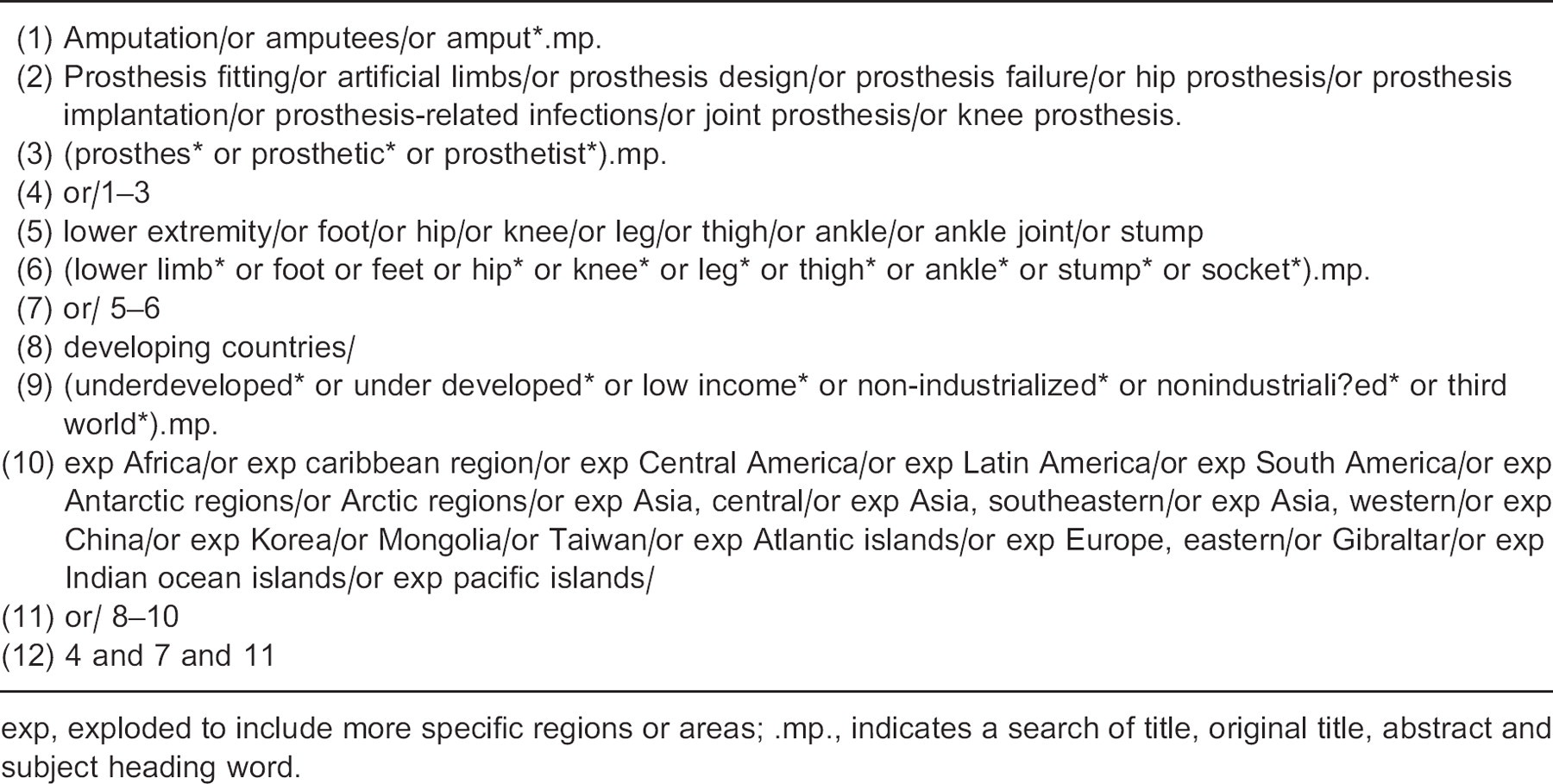
exp, exploded to include more specific regions or areas; .mp., indicates a search of title, original title, abstract and subject heading word.
Since a previous review of prosthetics in developing countries was already available for technologies prior to 1994, 1 this review focused on articles that were published since that time. The previous review involved a search of the RECAL database from 1961 to October 1994, although the details of the search strategy were not extensively reported. 1 In order to examine the thoroughness of this previous review, we compared the cited references against those retrieved in our search, and concluded that it was in fact comprehensive. Hence, only articles from 1994 onward that were not part of the previous review were included in this review. After the elimination of duplicates, precisely 106 articles remained.
Data were synthesized by reviewing the full text of all remaining publications and categorizing these studies in terms of technology type and study design. Technology types were broadly categorized as: feet and ankles, knees, sockets and suspension, and where the technologies related to entire prostheses, transtibial and transfemoral prostheses, with a focus on prosthetic materials, structures, and alignment methods. Furthermore, technologies were categorized in a tabular format by the specific name of the technology, so that studies could be referenced to a specific technology.
Articles were categorized by study design as either technical development, clinical (lab-based) testing, or clinical field testing studies and each category was defined as follows. Technical development included those studies which primarily focused on technology-related research and development without experimentation on human subjects. Clinical (lab-based) testing studies were those that involved human subjects and lab-based tests and outcome measures such as biomechanical or functional analyses. Typically subjects would not use the device for an extended amount of time (i.e., weeks), except for the purposes of acclimation. Clinical field testing studies typically involved testing for extended periods of time (months and years) in real world conditions. Here, field testing studies were further subdivided into ones where the study authors were involved in the development of the technology, and those where they were not. These independently performed evaluations were termed independent field testing. Publications that did not fit these categories were labelled as other. This general categorization follows the typical stages and cycles of prosthetic technology development, with the early stages involving highly technical aspects, and the later stages including clinical verification to ensure the technology is ready for general deployment in prosthetic rehabilitation (refer to figure 1). 10
Results
Of the total number of publications included in the review, 49 came from peer-reviewed journals and the remaining 57 from secondary sources. Of the peer-reviewed articles, about half were found in the journal of Prosthetics and Orthotics International. The majority of secondary publications came primarily from the International Society for Prosthetics and Orthotics World Congress proceedings. However, as expected these typically provided much less detailed information than the journal articles. Figure 2 presents a summary of the types of studies and technologies that were included in the review. Detailed information relating to the technologies is presented in Tables II–V.
Prosthetic feet and ankles
Prosthetic feet and ankles serve a number of important functions during gait such as providing shock absorption during loading response, stability during weight bearing, and smooth progression of the limb. 11 For feet used in developing countries, inadequate durability was identified as a primary issue a decade and a half ago. 2,3,5,7 Since then, an important body of work has helped to elucidate the extent of the problem. Using standardized measures, 12 independently run field trials have generated important data relating to the failure modes and rates of prosthetic feet that are used in developing countries, and the data suggest a diverse spectrum of outcomes when it comes to durability and structural failure. For example, in one field trial, 100% of the Fujian feet structurally failed and required replacement within 18 months. 23 The CR-SACH foot also presented with high rates of failure of 69% at 18 months. 23 Some of the more durable foot components included the Jaipur foot with a mean 70% chance of survival after 16 months, and the VI-solid foot with a 97% survival rate after approximately 18 months. 20,15 One of the determining factors in terms of prosthetic foot durability appears to be associated with the construction materials. Vulcanized rubber (as is used in both the Jaipur and VI feet) typically outperformed the lighter foam constructions.
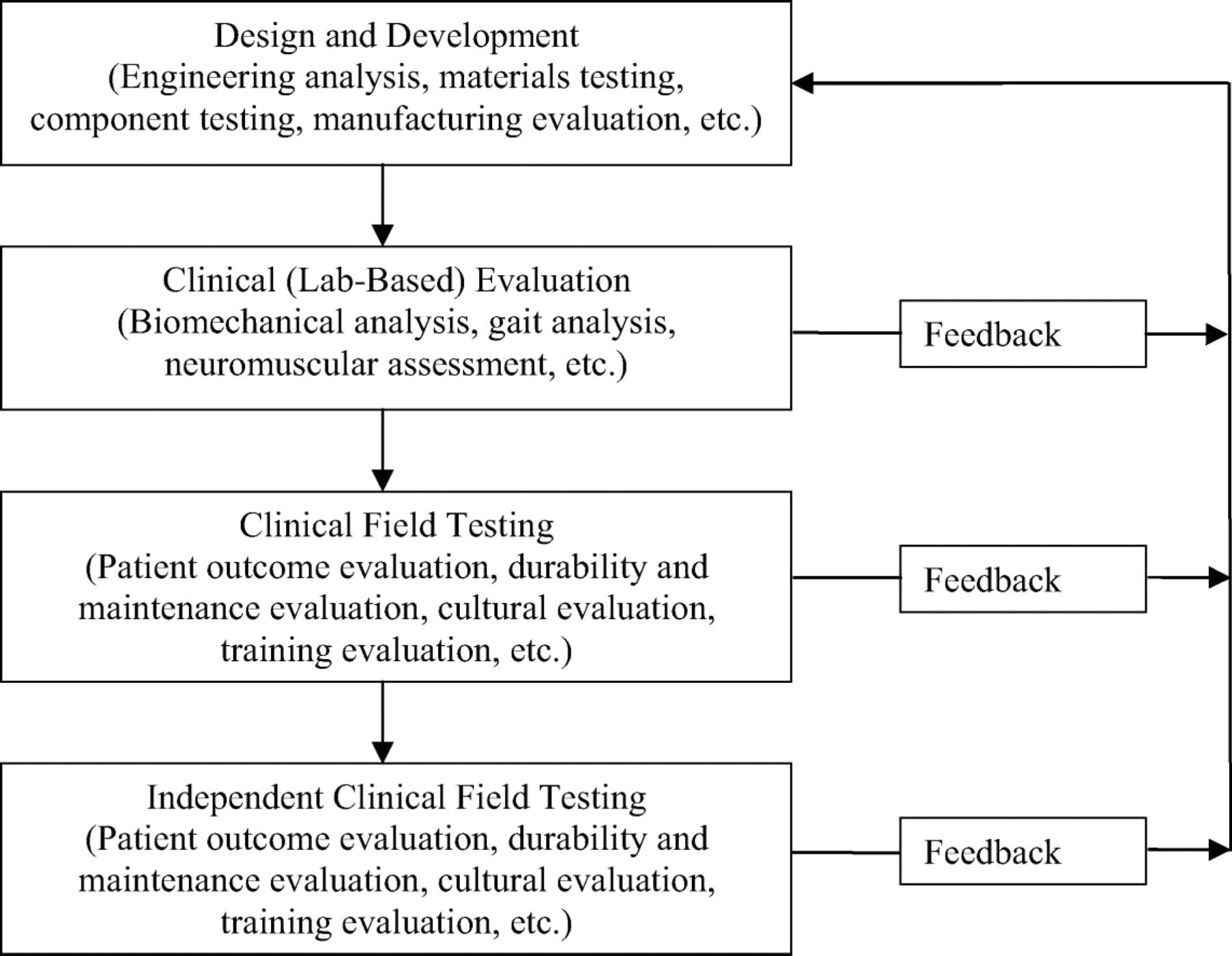
Product development strategy for prosthetic technologies. At each stage of the development process, and moving from top to bottom, higher levels of evidence are produced toward the development and adaptation of a prosthetic technology. Adapted from Gonzales et al. 10
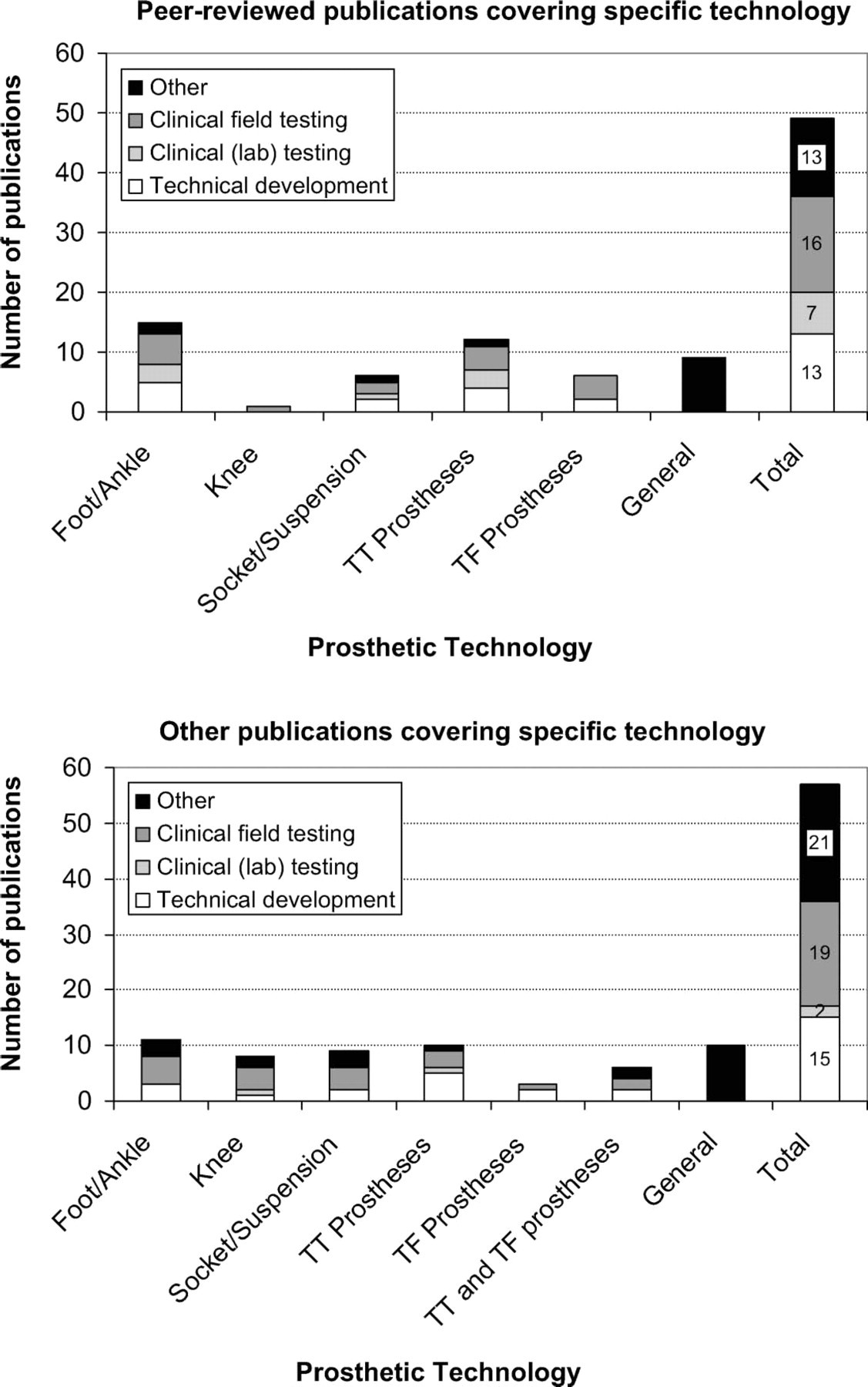
Summary of reviewed publications by type of study and technology including peer-reviewed publications (top) and non peer-reviewed publications (bottom). Where possible, studies were categorized by types of technologies and studies. Studies (i.e., review articles, media stories etc.) that could not be categorized as either clinical field testing, clinical (lab) testing or technical development, were categorized as ‘others’. Articles that dealt with technologies in general (i.e., review, editorial) were categorized as ‘general’. Abbreviations: TT, Transtibial; TF, Transfemoral.
List of foot/ankle technologies based on the literature review. Not all the feet used in 13,14 are presented here, since many are simply variations of the SACH foot.
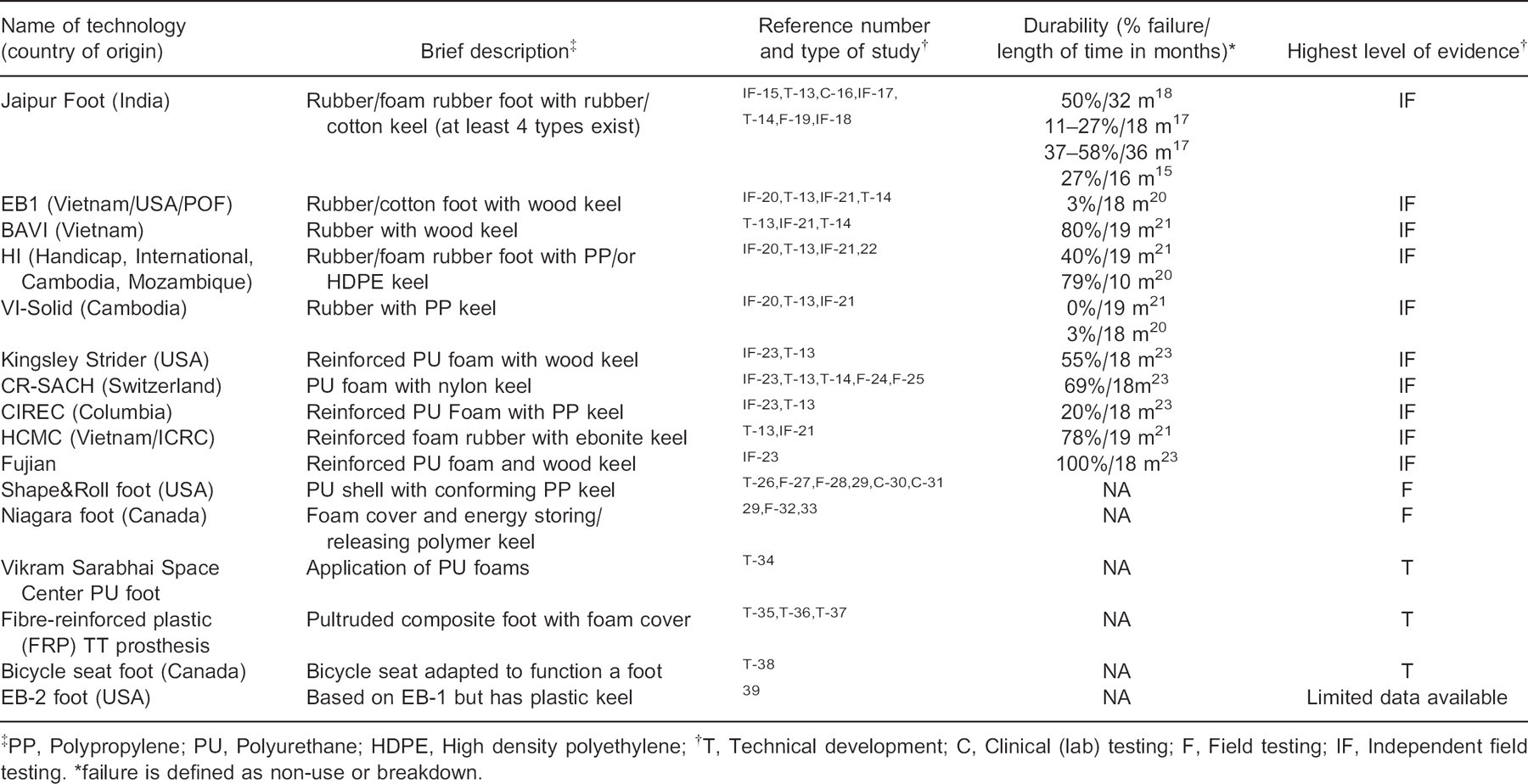
PP, Polypropylene; PU, Polyurethane; HDPE, High density polyethylene;
T, Technical development; C, Clinical (lab) testing; F, Field testing; IF, Independent field testing.
failure is defined as non-use or breakdown.
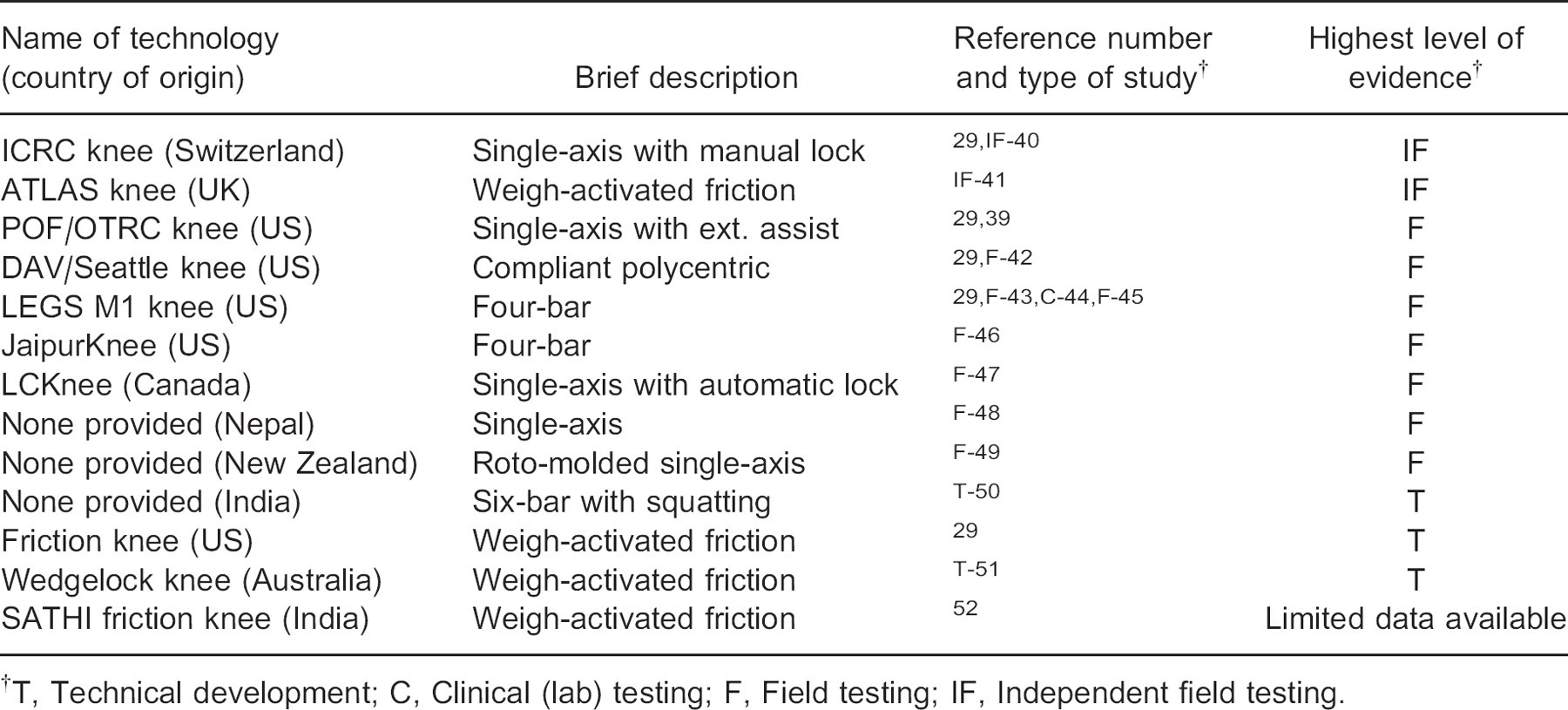
List of knee joint technologies based on the literature review.
T, Technical development; C, Clinical (lab) testing; F, Field testing; IF, Independent field testing.
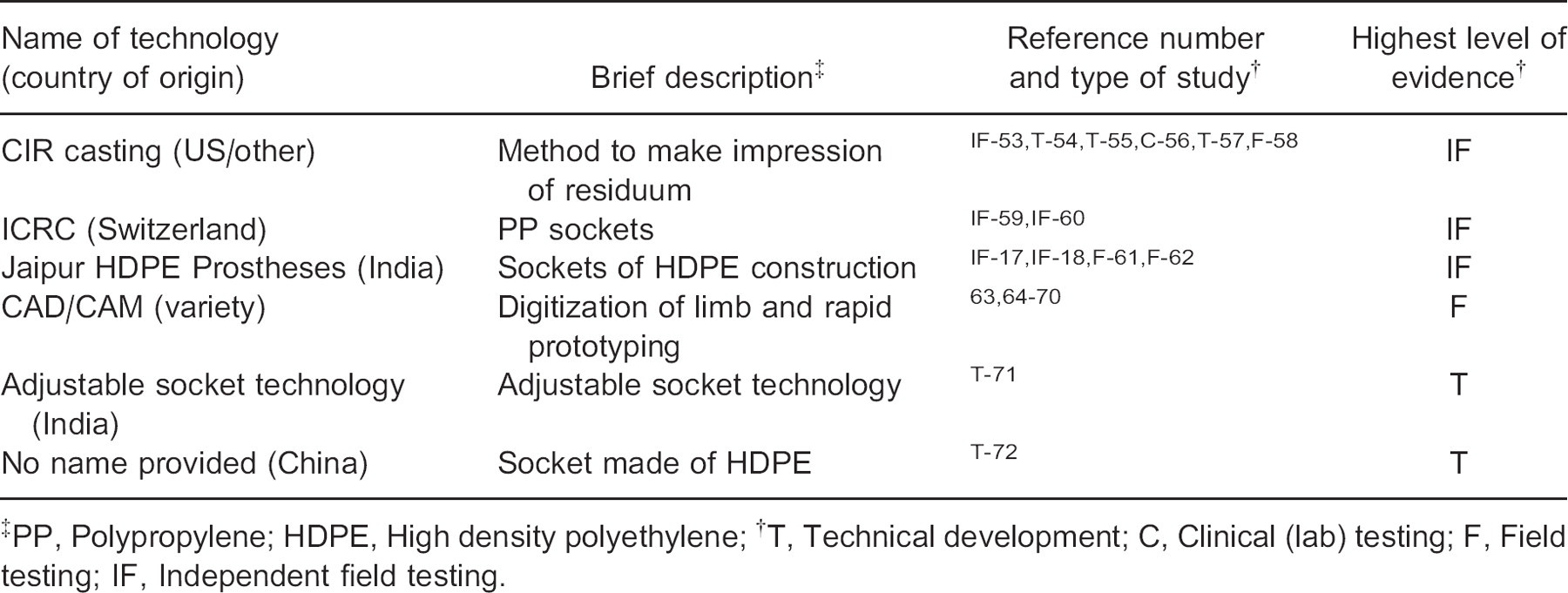
Socket/suspension technologies based on the literature review.
PP, Polypropylene; HDPE, High density polyethylene;
T, Technical development; C, Clinical (lab) testing; F, Field testing; IF, Independent field testing.
Supplemented by standardized mechanical testing, 13,73 results from independent field trials have helped to provide information on the types of failures that are occurring and their associated causes. Some of these include structural failure caused by rot (due to excessive moisture), 20 excessive wear of the sole resulting in the penetration of the keel (which is more prevalent in cultures where shoes are not customarily worn), 23 fracture of the forefoot and delamination between foam layers with repeated loading 23,13 , and deterioration due to direct exposure to sunlight. 13 These findings provide a definite indication of the design challenges that need to be addressed in order to improve the long-term performance of foot components, as well, as important feedback into the design process as outlined in Figure 1.
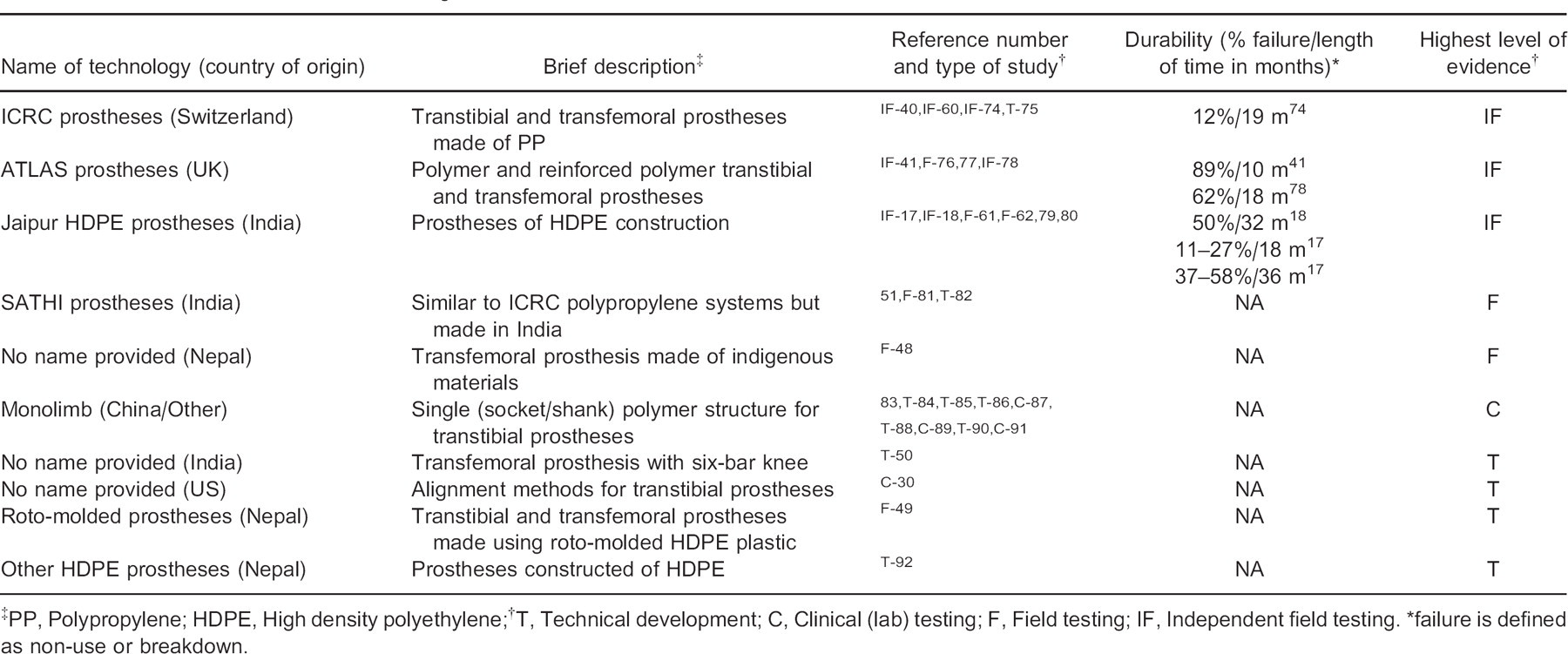
Transtibial and transfemoral technologies based on the literature review.
PP, Polypropylene; HDPE, High density polyethylene;
T, Technical development; C, Clinical (lab) testing; F, Field testing; IF, Independent field testing.
failure is defined as non-use or breakdown.
Whether imported or produced regionally in developing countries, most of the feet used in developing countries are based on the SACH foot design (Table II). 21,23 In their field trials Jensen et al. have primarily categorized the SACH feet by the type of construction material, which is either polyurethane foam or vulcanized rubber, the latter being more durable but also substantially heavier. 7,20,21 In general, durability issues were found to persist across most types of SACH feet, which are typically constructed from foam rather than the more durable vulcanized rubber. Moreover, SACH feet have been recognized (in studies performed primarily for developed countries) as being biomechanically inferior to other types of foot and ankle mechanisms, when used by physically active individuals. 93,94 To address these limitations of durability and biomechanical performance associated with existing SACH feet, a number of initiatives are targeting the development of feet that can still be produced at a low cost, but that improve biomechanical performance.
The Shape&Roll foot is intended to provide a smoother and more natural gait by more accurately mimicking the physiological functions of the foot and ankle complex of non-amputees. It accomplishes this by using a ‘programmed’ keel shape that is produced when the foot is under weight bearing. 26–28,97 Low-tech fabrication methods for the Shape&Roll foot have also been developed that make it possible for the foot to be produced locally in developing countries. 26,96,97
Another approach aimed at improving the biomechanical performance of prosthetic feet has been through foot mechanisms that have energy-storing and releasing capabilities, a technology that is regularly prescribed for active amputees in developed countries. The Niagara Foot uses a specially designed keel and ankle system that stores energy in early stance-phase and releases it in late stance-phase to mimic the normal plantar-flexion push-off action, thus potentially decreasing muscular effort and improving spatiotemporal measures, although only limited clinical data for the Niagara Foot are available to support this. 29,32 Field testing suggests the inner foot structure to be adequately durable but as with many other feet, durability issues arise with the softer, more cosmetic aspects of the foot. 29 Other similar technical developments include a durable mass-produced pultruded fibre-reinforced plastic foot 35–37 and the innovative adaptation of a bicycle seat assembly to function as a prosthetic foot, although limited information about field testing was found relating to these initiatives. 38
One of the most widely studied and published prosthetic feet is the Jaipur foot, which was originally developed in the 1970s in India. 16,98–101 The Jaipur foot offers a flexible keel/ankle that makes it functionally more appropriate in countries where it is customary to squat. The flexible structure also allows the foot to better conform to uneven terrain and results in more normal gait characteristics. 16 Independent field trials have found the Jaipur foot to be one of the more durable foot components currently being prescribed in developing countries. 15,17 However, the vulcanized rubber construction does result in a substantially heavier component, a caveat that may be addressed by using alternate materials such as polyurethane. 34
In summary, an important body of work involving independent field testing has revealed that a number of foot components are available that possess acceptable durability and performance. These are primarily of rubber construction and they tend to be heavy. Therefore, the challenge remains about how to make use of alternative construction materials to make the components lighter without compromising durability, especially in terms of the outer cosmetic shell.
Prosthetic knees
The primary function of a prosthetic knee joint is to provide articulation and allow knee flexion in swing-phase, and to resist flexion during weight bearing. 29 The technologically simplestand most commonly used mechanism is a single-axis hinge joint 18,29,40,41,48,49 (see Table III). In this system, aligning the prosthesis such that the knee axis is posterior of the weight-bearing line along with voluntary control of the residuum hip muscles provides some resistance to knee flexion. However, many individuals in developing countries ambulate over rough and uneven terrain, which increases stability demands, thus decreasing the effectiveness of this approach. To address this limitation, alignment stabilized single-axis knee joints can be equipped with manual locks, such as in the case of the ICRC knee, 40 but using this feature results in stiff-legged gait which has been deemed an unacceptable long-term solution. 29 To augment stability, attempts at replicating the highly successful braking action of weight stabilized knee joints (a concept that is otherwise typically used with less active elderly patients), have been relatively unsuccessful in the ATLAS prosthesis resulting in unreliable function and high rates of structural failure. 41
The ICRC manually locking and ATLAS weight-activated knees systems are also the only technologies to be evaluated as part of independent field trials in a developing country location. Based on those studies, the ATLAS knees were deemed to be unacceptable due to failures (defined as non-use and breakdowns) being reported in 83% of cases after only 7–10 months, compared to the ICRC knee which had a more acceptable failure rate of 32% after 15 months. 40,41 For the ATLAS system, in addition to excessive structural failure, unreliable function of the knee stabilizing mechanism was a major problem. 41 Whereas, the ICRC knee was relatively successful, likely due to the simplicity of the design.
In the pursuit of a more functional prosthetic knee joint, other investigators, including teams from Georgia State 29 (Friction knee) and University of Melbourne 51 (Wedgelock knee) in collaboration with the ICRC are examining similar avenues. However, as with the ATLAS knee, the challenges associated with these technologies relate to the consistency and reliability of the braking action which is adversely affected by wear within the braking mechanism and changes in coefficients of friction due, for example to exposure to humid or wet environments. 29
An alternate approach that avoids reliance on friction may be to use a lock, as with manually locking knees, but to have the lock automatically engage and disengage in response to the loading of the prosthesis. 47 This technology, termed the LCKnee, is currently undergoing field testing in both developed and developing countries and showing promising preliminary results relating to function and durability.
Polycentric knee joint mechanisms, incorporating four and six bar mechanisms to enhance stance-phase stability and swing-phase kinematics, have been highly and successfully utilized in developed countries. However, due to their increased complexity and associated costs, repairs and maintenance, these mechanisms have been deemed less appropriate for use in developing countries. 7,29 Two technologies to combat these limitations (LEGS M1 knee and Jaipur knee) have focused on the use of low-cost engineering polymers and simple fabrication techniques that can be applied regionally. 29,43,46 Both technologies are currently still under development and undergoing field testing although early results relating to function and durabiltiy appear promising.
One interesting variation of the polycentric knee joint, termed the DAV/Seattle knee, uses compliant linkages to eliminate the number of components, and injection moulded polymers to facilitate cost-effective fabrication. 29,42 However, the testing of this technology has primarily been limited to developed countries. Lastly, Chakraborty and Patil 50 describe a six-bar linkage mechanism that also facilitates squatting, which is in many cultures considered an important function. However, the apparent mechanical complexity of this device makes its suitability for application in most developing countries questionable.
In summary, although the single-axis prosthetic knee joint with manual lock appears to be a proven technology for developing countries, a number of potentially more functional alternatives are at various stages of development and evaluation. The trend is toward the use of polymers for construction, and in the majority of cases, moulding to allow for the adoption of mass production to reduce costs. However, long-term independent field testing is needed to demonstrate the feasibility and appropriateness of these technologies.
Sockets and suspension
Sockets serve the important role of interfacing the residuum and the prosthesis, allowing an individual to not only bear weight comfortably, but to have control over the movement of the prosthesis and to receive sensory feedback in terms of proprioception. 102 The challenges associated with the socket relate primarily to prosthetic fit, which relies in large part on techniques that are employed during fabrication. The socket is the most individual and custom-made part of the prosthesis, and its quality has a major influence on the function of the overall prosthesis and on comfort of the user. 63 The most common approach to socket fabrication in both developed and developing countries is to take a plaster wrap cast of the limb residuum, from which a modified plaster model is made. 5 The plastic socket is then formed around this plaster model. One substantial technological advancement impacting developing countries has been the application of thermoplastics such as polypropylene for socket (and prosthesis) fabrication. The use of polypropylene has resolved issues of storage such as short shelf life, that are associated with other materials such as polyester and are accentuated in humid environments. 103 Polypropylene is an easier and less costly material to work with. Waste material can also be recycled, thus further reducing material costs. 83 Moreover, since polypropylene can be reheated and reshaped, it facilitates socket changes to be more readily applied as needed to achieve better socket fit. 104 Finally, polypropylene has excellent durability which helps to decrease costly repairs, maintenance and replacements. 104
Polypropylene is readily used in the sockets of ICRC prostheses, which have been shown in independent field trials to give a product of acceptable quality (Table IV). Specifically, good prosthetic fit was attained in 43–78% of cases when polypropylene sockets were used. 59,60 Some of the identified underlying issues included inadequate socket wall height and prosthetic misalignment. Similar independent field testing results were obtained using the CIR sand casting method with 68% of individuals achieving comfortable fit and 64% reporting no pain. 53 In contrast, less favourable results were reported with the Jaipur transtibial and transfemoral prostheses with satisfactory socket fit being achieved in only 22% and 37% of cases, respectively. 17,18 The poor outcomes have been primarily attributed to inadequate formal training of the prosthetic clinicians and technicians. 17,18 As a result, one of the goals has been to provide clinics in developing countries with the skills and training necessary to master the techniques required to fabricate quality and well fitting sockets. 105,106 As alternative approaches, efforts have also been directed to either decrease the technical complexities involved in socket fabrication, and/or to make it possible to have these complex tasks performed outside of the clinics. 63,107
One way of achieving faster and more consistent production of prosthetic sockets to service a larger number of individuals is by using CAD/CAM systems. 64,65 CAD/CAM systems provide the means to capture and digitally model the precise shape of the limb. Using software, modifications can be made to the model, which can then be automatically manufactured into a positive socket model or directly into a socket. Since fabrication would typically be performed offsite at a central fabrication facility, a lower demand for highly skilled personnel at the clinic exists, as does the need for equipment required for fabrication of traditional sockets. This serves as one of the major appeals of CAD/CAM systems for socket fabrication in developing countries. 63 Additional, potential benefits of this technology may include increased quality of socket structure and socket fit, reduction of costs of long distance fittings (due to travel costs), shorter times required with the patient, 63,66,67 improved cost-effectiveness compared to conventional techniques, 68 and ease of storing and manipulating socket shapes as needed by clinicians for future use. 67 As such, CAD/CAM technologies have been shown to greatly increase productivity, up to 1340% as shown in one study, when used in clinics of developing countries. 64 The primary drawback of CAD/CAM technologies is the high investment costs associated with the hardware and software and ongoing maintenance, which substantially exceed the cost of manual labour around the world. 69 Also, the consistency and accuracy with which the shape of the residuum can be obtained, and socket fabricated, have in some cases been recognized as being a limitation of existing CAD/CAM systems. 70
A contrasting approach to CAD/CAM has been to simplify socket fabrication with methods that do not rely on the use of complex equipment. Much of the work has been undertaken by the Center for International Rehabilitation (CIR), and focuses on the use of a casting technique based on the dilatancy principle. 54,55,59,108 In this technique, granules (e.g., sand or polystyrene beads) are enclosed in a flexible container, into which the desired shape of the residuum is impressed and can be held fixed through the evacuation of air out of the container. A positive plaster form for use in socket fabrication can then be made from the impression. Independent field trials found the CIR casting system to produce socket fit that was consistently on the loose side, but with the use of stump socks better fit was achieved than previously with the traditional plaster of Paris casting method. 53 Improvements have been made to the CIR casting technique since, and results of a recent pilot field study suggest that a more intimate socket fit is achievable. 56 In addition, the casting technique allows a socket to be fabricated more quickly. 57 Recent improvements include the use of polystyrene beads in place of sand to facilitate a lighter and more portable system. 57,58
Another potential avenue for simplifying the socket fabrication process is to shape the socket directly over the residuum by eliminating the casting and positive form steps. This is not a new approach, although it may be more viable with the development of fast curing resins that have the adequate mechanical properties. A technical description of a potential material for this application is presented by Cha et al. 109
The need for adjustable socket technologies exists in developing countries to allow recent amputees to achieve early ambulation without the fit-related issues that arise from residual limb volume changes at these early stages of rehabilitation. An adjustable socket also presents the opportunity of multi-client use by allowing the circumference and length of the socket to be adjusted, thus potentially decreasing costs. The technical aspects of a cost-effective adjustable transfemoral socket technology are reported by Sathishkumar et al. 71
Finally, the function of a socket is not possible without adequate suspension. The most common methods for achieving socket suspension utilize cuffs and belts, commonly fabricated from leather. 29 Despite the numerous advantages, factors such as the increased complexity and associated demand for highly skilled personnel have made the adoption of suction socket suspension in developing countries problematic. No studies specifically addressing socket suspension technologies for developing countries were found.
In summary, sockets continue to be made using conventional socket fabrication techniques and plastics such as polypropylene and high density polyethylene. Independent field testing has revealed that achieving good socket fit remains a challenge, partially because of the requirement for well trained personnel. CAD/CAM has the potential to address this issue, but limited information in terms of independent field testing data is available.
Materials, structures and alignment
An effective prosthesis can only be achieved if individual prosthetic components (feet and ankles, knees, sockets and suspension) can be appropriately and simply integrated into a functional structure. This includes a means for providing the intermediate aspects of the structure (e.g., pylons) and a means of connecting the components (adaptors) in a way that allows for prosthetic alignment changes. However, achieving the correct prosthetic alignment has traditionally been a challenge in developing countries. 4 In response, a number of systems specifically addressing the needs of developing countries have been developed and are currently used as part of transtibial and transfemoral prostheses.
One of the most widely used transtibial and transfemoral prosthetic systems is provided by the ICRC 104 (see Table V). The current versions, which are primarily constructed of polypropylene and stainless steel, have been around since the early 1990s. The prostheses offer a unique angular alignment system comprised of convex and concave disks that work much the same way as conventional pyramid-type systems. 103 Despite the provision of an alignment system, independent field trials reveal that in some 35% of cases prostheses were misaligned with the ICRC system. 40 This was primarily due to poor training and prosthetist error and to a lesser degree limitations of the technology itself. 40
The use of polypropylene for construction of the ICRC system allows waste material to be reprocessed and recycled during fabrication, thus further reducing overall costs. 110,111 Polypropylene is lightweight and relatively durable as demonstrated via field trials of ICRC transtibial prostheses 60 and more recently in independent field trials. 74 Similar findings were obtained for transfemoral prostheses despite some functional and structural issues mainly associated with the design of the knee joint. 40 A knee disarticulation version of the prosthesis is also available. 75
Another system, developed by Blatchford and Sons, termed the ATLAS prosthesis, uses an injection moulded fibre-reinforced nylon construction for the various components and polypropylene for the socket. 76,77 The goal of the system was to provide appropriate biomechanical function, cosmesis, durability and ease of fitting at a reasonable cost. 76 Independent field trials revealed critical structural deficiencies in the shank portions of the transtibial prostheses 78 and in the knee joint of the transfemoral prostheses. 41 For summarized data on failures refer to Table V. Moreover, high rates of prosthetic misalignment were reported and as a result, both types of prostheses were considered unacceptable for general use. 41,78
Independent field testing has also been performed on Jaipur prosthetic technologies utilizing high density polyethylene (HDPE) construction. The technology, which was originally developed in India, involves the heating and moulding of HDPE drain pipes into the structure of a leg. 18 For the transfemoral version of this prosthesis, various knee joints were used including sidebars and a drop lock metal knee joint in the clinical field trials. 18 Attributed primarily to the poor training and education of the individuals constructing both the transfemoral and transtibial versions of these prostheses, the technical and clinical outcomes (including durability, alignment and socket fit) associated with this technology were deemed highly inadequate, 17,18,61 although recent efforts have been initiated to address some of the inadequacies. 79,112 Also as part of recent efforts to further improve socket fit and decrease fabrication costs, the use of the CIR sand casting technique was explored during field testing. 62 The application of HDPE drainpipes is not exclusive to the Jaipur prosthetic systems, and variations of this approach exist elsewhere. 72,92
The SATHI transtibial and transfemoral prosthetic systems are similar to the ICRC systems, but are more affordable (costing $85 for a finished transtibial prosthesis) since manufacturing is done locally in India. 81 These polypropylene moulded systems are lightweight and provide easy alignment, 82 although further design modifications have been suggested to decrease structural failures and improve function. 81
The concept of the monolithic transtibial prosthesis, or monolimb, is intended to simplify the construction of the socket and connecting pylons of a conventional prosthesis into a single structure comprised of thermoplastics such as polypropylene. 84–86 A disadvantage of this approach, is that alignment changes are not readily possible once the prosthesis is made, so a number of studies have focused on methods to accurately determine initial prosthetic alignment. 83,87–89 More recently, the monolimb concept has undergone technical development and biomechanical evaluations to optimize its structural properties. The goal has been to provide a shank that is flexible and can provide dynamic elastic response in similar fashion to energy response feet such as the FlexFoot. 90,91
Low cost and low weight transtibial and transfemoral prostheses are also being fabricated using roto-moulding. 49 This process requires moulds to be manufactured, which is possible to do locally in developing countries using low-level technology. Plastic powder (HDPE) is placed within the mould, which is heated to 270°C, and then slowly rotated so as to achieve even distribution of the melted plastic. Preliminary results from field testing are reported demonstrating the devices to be of adequate strength. 49
A number of other initiatives have been reported to some extent. Meanley and Reed 48 describe a longitudinal follow-up of a single subject field testing trial of a transfemoral prosthesis fabricated using only materials available locally in Nepal. Suspension is a combination of suction and a belt, the socket is constructed of HDPE pipe, and the knee joint is a single-axis design with the hinge constructed from the front axle of a bicycle. The prosthesis includes a SACH foot constructed of hardwood and rubber. A three year follow-up found that the prosthesis required 3–4 minor repairs, and was well utilized by the user. Other projects that are trying to utilize locally available materials are investigating the application of locally grown vegetation for reinforcing fibres in composite materials for prostheses. 113
A significantly more sophisticated prosthesis is described by Chakraborty and Patil, 50 which utilizes a six-bar knee that also controls ankle dorsi/plantarflexion motion. A technical description and results of biomechanical analysis of a single subject are provided.
Lastly, Hansen et al. 30 investigate the ideal prosthetic alignments in transtibial prostheses utilizing roll-over shape principles. The goal of this work is to develop methods that lead to a better a priori prosthetic alignment, therefore eliminating the need for special ‘alignment’ hardware.
In summary, as plastics become more readily available in developing countries, they are also being more commonly utilized in the fabrication of prostheses. To make it possible to use these lower grade materials, alternate structures are used. This includes shell structures rather than typical modular or endoskeletal structures and attachment and alignment points with large contact surfaces to better distribute loads. Independent field testing has revealed that these approaches can deliver good results in terms of durability, but challenges remain when it comes to achieving acceptable prosthetic alignment.
Discussion
In the mid-1990s a number of publications and key meetings of experts identified major technical issues associated with prosthetic technologies intended for developing countries. More specifically, these included inadequate durability of prosthetic feet, 3,5,7 poor quality, fit and alignment 4,5,7 and inferior prosthetic function. 8 A decade and a half later, the extent to which progress has been made has been reviewed in a search of available literature.
Since the mid-1990s, an important body of work had been undertaken to manage the technical and functional quality of prosthetic technologies. 114 This includes the development and application of standardized outcome measures, namely the ISO standards for mechanically testing the structural integrity of prosthetic components, 13,73 and perhaps more importantly outcome measures to evaluate the use, function, and durability of components in the field. A body of work by Jensen et al., involving the independent field testing of various prosthetic technologies, has played an important role in elucidating and quantifying the issues relating to foot durability, socket fit, prosthetic alignment, and others. As seen in the results section, these publications have provided standardized data to help assess and compare technologies in terms of their appropriateness for use in developing countries. Just as importantly, these studies provided real world information about which designs and technologies are most effective (in terms of durability, workmanship and performance), as well as, feedback information (a critical element of the design process) that facilitates the development of better prosthetic devices (Figure 1). Examples of this include the durability inadequacies found in the CR-SACH foot (ICRC) during field testing 23 and the follow-up work to address these shortcomings, 24 or similarly the Jaipur systems. 17,18,79
However, specifically addressing the issue of foot durability, only two papers were found that provided some level of detail about the progress on this front. 24,25 The main problem with foot durability relates to the softer (cosmetic) aspects, rather than the structure itself, 23,25 yet little new information has been published addressing this aspect. The primary objectives of most of the papers found in the review pertaining to prosthetic feet focus on the improvement of biomechanical function 26,28,32,95 or durability of the rigid structure of the foot, 36,37 which while important, may be somewhat misdirected from addressing the primary problems. 115 Certain prosthetic feet, such as the Niagara foot are composed of separate keels and cosmetic covers, making it possible to replace a damaged cover. However, frequent replacements can be costly and in some cases impractical, especially when individuals are required to travel long distances to access a clinic. Therefore, based on this review, a recommendation is that future initiatives focus on the development of lightweight foot components with improved durability of the entire prosthetic foot structure including the cosmetic shell.
Improving biomechanical performance should remain an important goal in the development of prosthetic components for developing countries, but not at the expense of durability. More biomechanically sophisticated devices are typically comprised of more complex mechanisms, which are more likely to break down when compared to simpler ones. They may also require more maintenance and repairs once they do break down. Similarly, due to limited resources, or perhaps long travel distances to clinics, these devices may continue to be used even though badly damaged. So the added functional benefits of a more sophisticated prosthetic component should be evaluated over the lifespan of the device. Such a component may be more functional initially, but it may also be prone to more rapid structural and functional deterioration.
The development of prosthetic knees is one area where the balance between biomechanical function and durability requires careful consideration. The functional norm in developing countries is a manually locking singles-axis knee, 29 which typically results in stiff-legged gait. This is a major limitation, which a number of initiatives are presently trying to address. As part of ongoing work, independent field trials are recommended to evaluate the use of these more complex technologies in developing countries.
Addressing the high priority areas of socket quality and fit are primarily dominated by two philosophies; one is to use high-end technology and centralize operations (CAD/ CAM), and the other is to develop simpler socket fabrication techniques (CIR Casting). Evidence demonstrating either of these technologies to be substantially better than conventional plaster of Paris techniques is generally limited, although each technique reports success at some level of implementation. Because achieving good socket fit relies so much on the skills and experience of the prosthetic clinician or technician, it may be unlikely that a technology will replace the training and education that are needed to achieve this. Nevertheless, techniques such as CAD/CAM and CIR casting may help to mitigate some of the burden. This similarly applies to prosthetic alignment, where technologies can help to facilitate trained personnel in achieving good prosthetic function. Two approaches dominate the published literature. Both are based on the use of polymers such as polypropylene or high density polyethylene (HDPE), but one approach utilizes modular systems, and the other a monolithic structure. For the monolithic systems, where alignment is not readily adjustable at the time the prosthesis can be worn, the focus has been on determining alignment a priori. More generally, this work may help to simplify the prosthetic alignment process, enabling personnel in developing countries to achieve better clinical outcomes.
One of the challenges of performing a literature review to paint a picture of the technological landscape of developing countries is that research and development work that is being conducted in developing countries may be restricted when it comes to dissemination in peer-review publications. As a result, it is important that such reviews attempt to access other less formal forms of information as was the goal of this initiative. However, we recognize that there still may be important work that is being conducted which was not captured by this review. This raises an important point: if information is not published, or if it is very difficult to access, then it will have very limited impact on advancing the respective field of research, in this case prosthetic technologies in developing countries. Collaboration between teams in developed and developing countries is one way of facilitating high quality and clinically relevant research, development and evaluation activities that are publishable in peer-reviewed journals. Moreover, where applicable, projects and resulting publications should aim to cover the breadth of activities including technical development, clinical assessment and field trials, as outlined in the design cycle of Figure 1. In this way, the development of simple, durable and functional prosthetic technologies to address the diverse needs of developing countries may be an attainable goal.
Conclusions
It remains a challenge to design prosthetic technologies for developing countries given the conflicting design requirements. Components should be functional since they are typically used by active young individuals, but at the same time they must also be affordable, highly durable, and culturally and environmentally appropriate. The review of literature suggests that important steps have been, and are continuing to be taken to improve the prosthetic technologies used in developing countries. An important part of the road ahead continues to be the close collaboration between developed and developing countries, and the undertaking and dissemination of formal research, development, and evaluation activities, which should be a pivotal part of the process.
Acknowledgements
I would like to thank Pui Ying Wong for her expertise and many hours of help in performing the literature searches.