
Abstract
Background:
Silicone toe separator is considered as a conservative treatment for hallux valgus. The prefabricated toe separator does not fit all. However, effectiveness in prescription of the custom-mold toe separator is still unknown.
Objectives:
To investigate the effect of using a custom-mold room temperature vulcanizing silicone toe separator to decrease hallux valgus angle and hallux pain. The compliances, complications, and satisfactions of toe separator were also explored.
Study design:
A prospective, randomized single-blinded controlled trial.
Methods:
A total of 90 patients with a moderate degree of hallux valgus were enrolled in a study at the Foot Clinic, Siriraj Hospital, Thailand. Patients were randomized into two groups; the study group was prescribed a custom-mold room temperature vulcanizing silicone toe separator for 6 h per night for 12 months. Patients in both groups received proper foot care and shoes and were permitted to continue drug treatment.
Results:
In total, 40 patients in the study group and 39 patients in the control group completed the study. The hallux valgus angle was obtained through radiographic measurement. At month 12, both groups had significant differences in mean hallux valgus angle with a decrease of 3.3° ± 2.4° for the study group and increase of 1.9° ± 1.9° for the control group. There were statistically significant differences of hallux valgus angle between the two groups (p < 0.05) at the end of the study. Hallux pain was decreased in the study group.
Conclusion:
A custom-mold room temperature vulcanizing silicone toe separator can decrease hallux valgus angle and pain with no serious complications.
Clinical relevance
The custom-mold room temperature vulcanizing silicone toe separator for treatment of hallux valgus reduces deformity and hallux pain.
Keywords
Background
Hallux valgus is a common forefoot deformity that refers to an abnormal angulation of the great toe deviated laterally and the first metatarsal deviated medially. 1 Pulling forces from the long flexor and extensor tendons cause the metatarsal head to move medially 2 and the great toe to crowd toward the second or third toes. Unquestionably, the cause of HV is multifactorial. The combinations of intrinsic and extrinsic factors have been considered, 3 such as the structure of pes planus, 4 functional tightness of the Achilles tendon, 5 and degenerative joint disease at the first metatarsophalangeal joint. 6 A family history of the condition has also been found as a major causal factor.7,8 Moreover, HV has a tendency to present itself in individuals who wear ill-fitting shoes with pointed toe box and high heels,3,9,10 which have been shown to increase the risk of developing the condition by upward of 15 times compared to use of regular footwear. 11
Major complaints from patients who visit physician offices are pain in the form of a bunion or calluses and corns. Shearing and distension occurs at the medial capsule or the proper plantar digital nerves of the medial plantar nerve. Without treatment, the deformity can continue to develop. The degree of severity of HV is classified by various ranges of the hallux valgus angle (HVA) and deviation pattern. 12
Treatments for HV are either conservative or operative in nature. 13 The common conservative interventions are proper fitting footwear with a wide deep toe box, 14 stretching exercises,15,16 therapeutic cold treatment, 17 nonsteroidal anti-inflammatory drugs (NSAIDs), 18 and muscle relaxants. 19 A variety of orthoses have been prescribed as treatment: insoles, 20 pads, night splints, and toe separators (TS). 21 Previous studies have suggested that TS is one of the most common treatments to alleviate pain, improve toe alignment, increase biomechanical function, and improve walking patterns.22,23
The TS is commonly made of silicone. Prefabricated silicone TS are commonly prescribed to slow the progression of HV. However, this type of device does not provide the ideal intimate fit. 24 A loose fit and slippage 22 can cause shear forces and lead to pain over affected toes. As a result, potential acceptance and compliance by the patient can be decreased. A custom-made TS is another option that can reduce these problems by providing a more intimate and improved fit.
Although there are benefits to using custom options, some patients cannot afford high-cost TS which typically cost about US$250. Using a low-cost material that is not traditionally utilized for a TS is potentially a novel approach to HV treatment. It is because of the aforementioned issues that the authors decided to investigate the effectiveness of a custom silicone orthosis as a formidable low-cost option for treating HV.
We choose to use a room temperature vulcanizing (RTV) silicone (RTV585) which costs US$17 per kilogram. Previous research utilized liquid silicone to fabricate medial arch supports and foot orthoses for treatment of foot problems.25,26 However, there are no studies reporting the effectiveness of a TS made from RTV silicone to decrease the HV deformity. Therefore, a randomized control trial study consisting of a treatment group and control group was conducted.
The primary objective of this study was to determine the effectiveness of the custom-mold RTV silicone toe separator to decrease HVA in individuals diagnosed with HV.
The secondary objective was to determine the effectiveness of the custom-mold RTV silicone toe separator to decrease hallux pain (pain of the big toe) as well as investigate possible complications, patient compliance, and satisfaction.
Methods
Subjects
The study protocol was reviewed and approved by the Institutional Review Board at Siriraj Hospital, Bangkok, Thailand (Si361/2013) and was supported by the Siriraj Research Development Fund (managed by Routine to Research: R2R). From January to December 2013, 90 patients who had HV were recruited to participate in the study. A physiatrist who specialized in foot problems performed a complete foot examination and provided the clinical diagnosis of HV. The inclusion criteria for participation in the study were males and/or females from 18 to 80 years with a moderate degree of HV (HVA: 20°–40°). 12 Previous literature identified a mean HVA of 30° as a “moderate to severe degree of deformity.” 27 The patients were excluded from the study if the following were present: foot numbness or foot ulcer, having acute inflammation of first metatarsophalangeal joint, having hallux rigidus or hallux limitus, continuously using any types of TS or HV strap in the past year, or having silicone allergies. If the patients had a moderate degree of HV bilaterally, the more severe of the two was chosen for the study, as determined by radiographic measurement.
Sample size calculation
Our sample size calculation was based on the ability to detect a clinically important difference in HVA, where the clinically significant change of HVA was 5°. Based on a power of 0.80 to detect a significant difference (5% type I error and 20% type II error, p = 0.05, two-sided), 37 patients were required for both the study group and the control group. The recruited sample size was 90 subjects in total (45 subjects per group with an estimated 20% drop-out).
Study protocol
Once the study eligibility was confirmed, an information sheet and verbal explanation were provided to the patients, and a signed informed consent form was obtained prior to study participation. The patients were then randomly allocated to either a study group or a control group by a research coordinator. The patients had an equal probability of assignment to each of the groups.
Patients in both groups were given standard treatment including proper foot care which included removing any calluses at the plantar or medial side of the foot and provision of low-heel shoes with a wide-and-deep toe box. Only the patients who were randomized to the study group were referred to the orthotist who prepared the custom-mold RTV silicone toe separator.
Apparatus
Each patient in the study group was cast in a corrected position for a mold. A silicone TS was then produced from the mold (Figure 1).

The custom-mold room temperature vulcanizing silicone toe separator.
Patients were recommended to wear the device at least 6 h/day during the night. If any signs of irritation or discomfort occurred, the patients were instructed to contact the physiatrist immediately. Patients were provided with logbooks, questionnaires, and follow-ups every 3 months.
Data collection
At baseline, patient demographics were collected, as well as average hours worn in walking shoes, foot issues on side of deformity, duration of HV, and family history (Table 1). The impact of deformity on the patient’s ability to walk and shoe-fitting problems were recorded using a numeric rating scale (NRS). The questions were scored from 0 (no problem) to 10 (worst problem).
Baseline demographic and clinical characteristics.
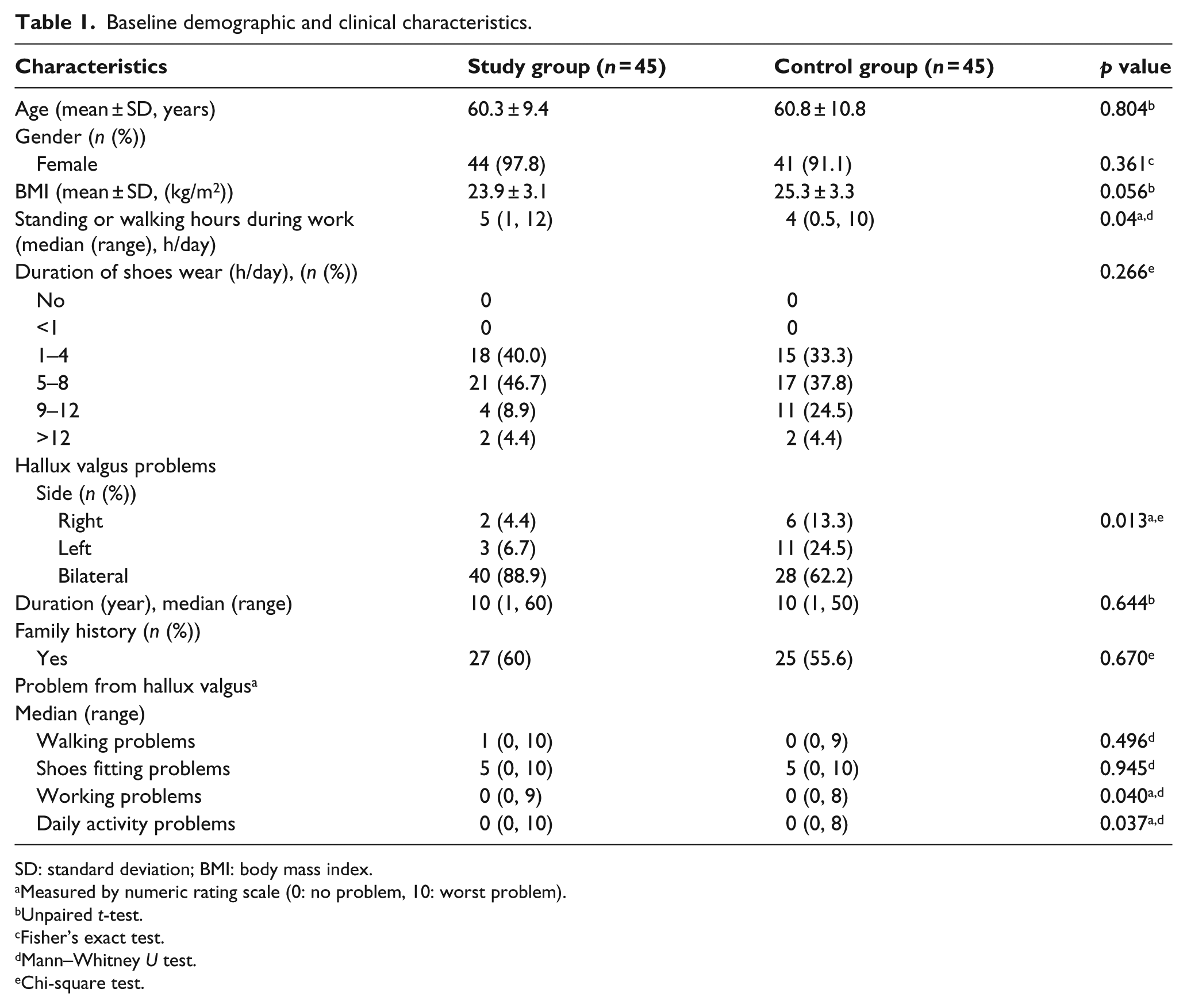
SD: standard deviation; BMI: body mass index.
Measured by numeric rating scale (0: no problem, 10: worst problem).
Unpaired t-test.
Fisher’s exact test.
Mann–Whitney U test.
Chi-square test.
The primary outcome measure in this study was the HVA, which was obtained from both the study group and the control group through measurement of a weight-bearing anteroposterior radiograph. Each radiographic image was evaluated at months 6 and 12 by a physiatrist and a radiologist who were blinded to the groups of participants. The HVA of months 6 and 12 were averaged by taking recorded values obtained by both raters.
The secondary outcome measures were hallux pain, compliance, complication, and satisfaction. At baseline and every 3 months, hallux pain experienced within the last 24 h was obtained from a questionnaire which used an NRS scored from 0 (no pain) to 10 (worst pain).
Compliance was measured by recording the hours of device usage per day which was then averaged each week and reported in the logbook. Any complications caused by the device such as abrasions or rashes were also recorded. Furthermore, at the end of the study, the treatment satisfaction in six sub-domains—fitting, comfort, perspiration, cosmetic appearance, maintenance, and overall satisfaction—were recorded. An NRS scored as 0 (dissatisfaction) to 10 (most satisfaction) from both groups was used. Intentions for future use as well as suggestions for improving the quality of the device were recorded.
Statistical analysis
All statistical analyses were performed using PASW Statistics (SPSS) 18.0 (SPSS, Inc., Chicago, IL, USA) and a p value of less than 0.05 was considered a statistically significant difference. The outcome measures were reported by both per protocol (PP) and intention-to-treat (ITT) analysis. In PP treatment, tests were performed to perform statistical analysis solely on participants who completed the full treatment. The ITT was performed because it is a reliable test which takes into account the “last value carried forward” regardless of whether or not the subject drops out of the study.
The median (range) was calculated for duration of HV problem (years), impact of the HV deformity, hallux pain, and satisfaction (NRS from 0 to 10). Patient compliance using the RTV silicone toe separator (h/day) was calculated by mean and standard deviation (SD). Any complications and the participant’s future intention of using the device were calculated as a number and percentage. For demographic data, an unpaired t-test and Mann–Whitney test were used to analyze the differences of quantitative data with normal distribution and non-normal distribution, respectively. Additionally, Fisher’s exact test and chi-square test were performed to analyze the differences of categorical data.
To explore the primary outcome of HVAs, as measured in degrees, a repeated-measures analysis of variance (ANOVA) with the use of a Bonferroni correction for multiple comparisons was used to analyze the differences between the study group and the control group at baseline, month 6, and month 12 as well as the relationship of the data in the same group between different timelines.
To explore the secondary outcomes of hallux pain, compliance, complication, and satisfaction, the Friedman test was performed, and Bonferroni correction for multiple comparisons was used to analyze the difference of the data between pre- and post-intervention in the same group. The Mann–Whitney U test was used to analyze the differences between the study group and the control group at the baseline and months 3, 6, 9, and 12.
Results
A total of 90 patients participated in the study. Half of them were randomly allocated into the study group and another half into the control group. In total, 43 patients from the study group (95.56%) and 42 patients in the control group (93.33%) returned for follow-up at months 3 and 6. In addition, 40 patients from the study group (88.89%) and 39 patients in the control group (86.67%) returned for follow-up at month 9 and continued participation until the end (Figure 2).
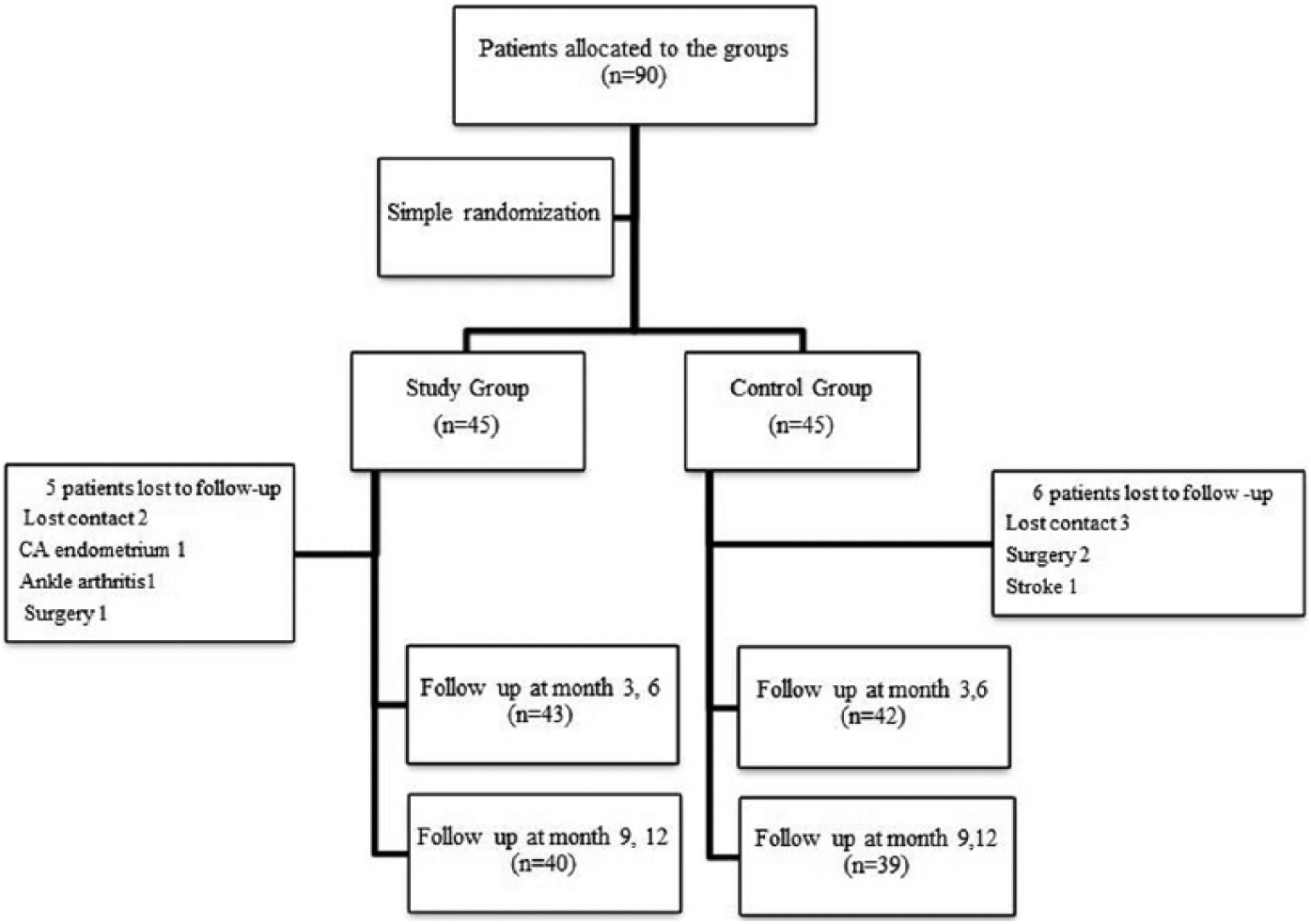
Flow diagram explaining patient participation. CA: cancer.
Table 1 summarizes the characteristics and foot problems of participants. The analysis of the baseline measurements of two groups reveals the similarities with regard to age, gender, body mass index (BMI), duration of shoe wear, duration of HV history, family history, and walking and shoe-fitting problems from HV. The analysis indicated that there were no significant differences between the two groups for the aforementioned measurements (p > 0.05). At baseline, there was a significant difference in the number of hours spent standing and/or walking at work between the two groups, 5 and 4 h, respectively. The differences in location of HV deformity with reference to foot side are noted.
Primary outcome
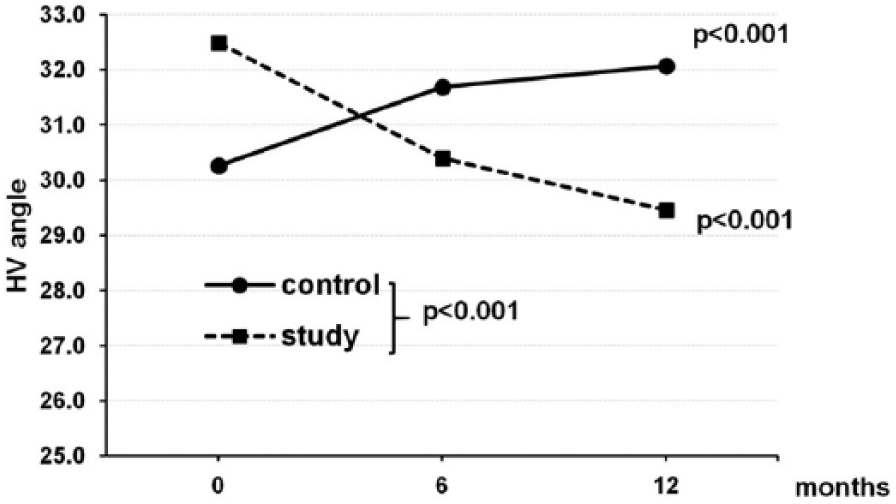
The HVA was measured at baseline, month 6, and month 12 and reported in both PP and ITT analysis as presented in Table 2. At baseline, there was no significant difference in HVA between groups, although the study group had more severe HVA (of 32.0° ± 4.8° compared to 30.6° ± 5.2°). After 12 months of using the TS, the HVA of the study group decreased 3.3° ± 2.4° from 32.0° ± 4.8° to 28.8° ± 5.8°, whereas the HVA of the control group increased 1.9° ± 1.9° from 30.6° ± 5.2° to 32.5° ± 5.4° (Figure 3).
Hallux valgus angle (mean ± SD), hallux pain median (min, max), and difference of hallux valgus angle pre- and post-intervention using the custom-mold RTV silicone toe separator.
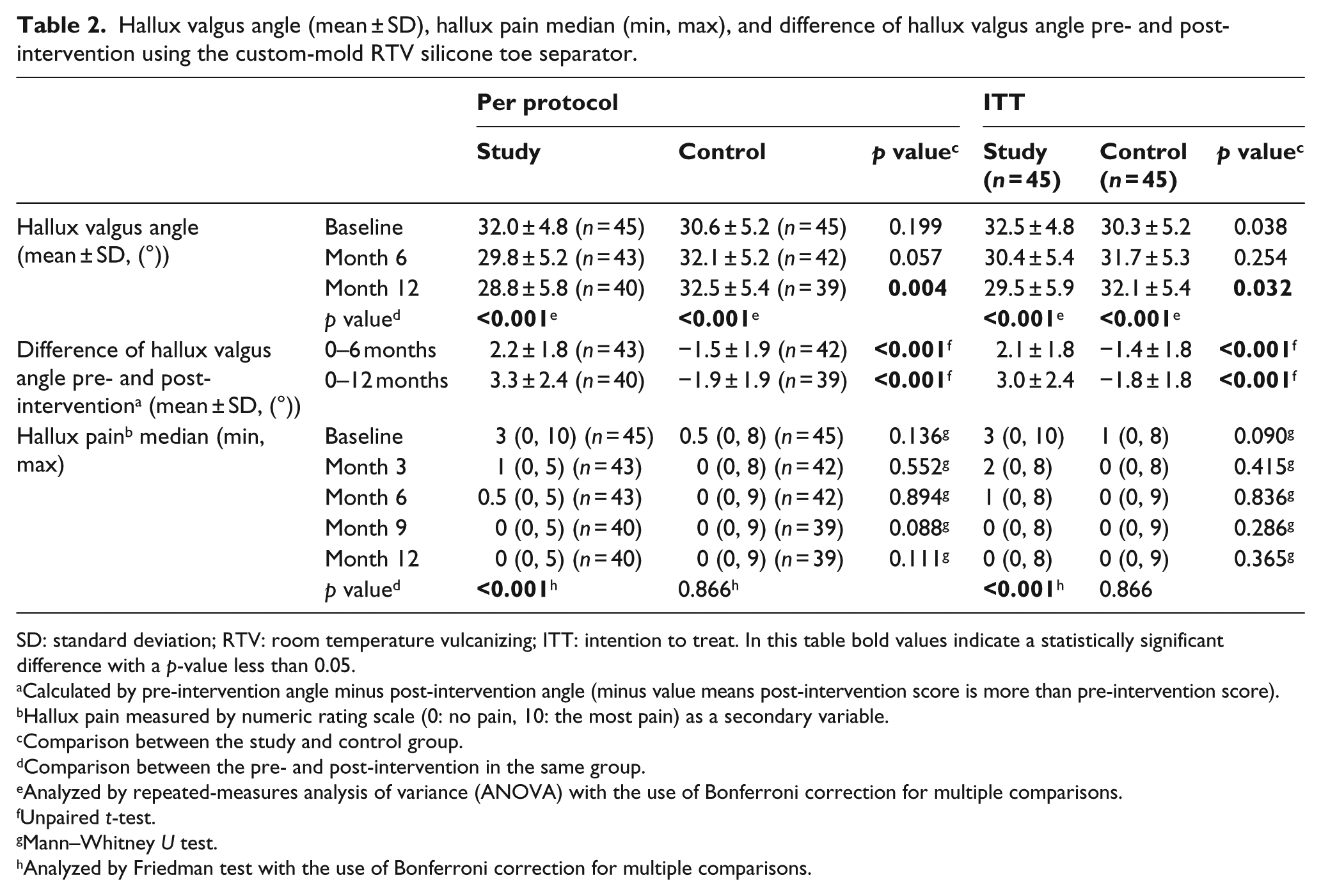
SD: standard deviation; RTV: room temperature vulcanizing; ITT: intention to treat. In this table bold values indicate a statistically significant difference with a p-value less than 0.05.
Calculated by pre-intervention angle minus post-intervention angle (minus value means post-intervention score is more than pre-intervention score).
Hallux pain measured by numeric rating scale (0: no pain, 10: the most pain) as a secondary variable.
Comparison between the study and control group.
Comparison between the pre- and post-intervention in the same group.
Analyzed by repeated-measures analysis of variance (ANOVA) with the use of Bonferroni correction for multiple comparisons.
Unpaired t-test.
Mann–Whitney U test.
Analyzed by Friedman test with the use of Bonferroni correction for multiple comparisons.
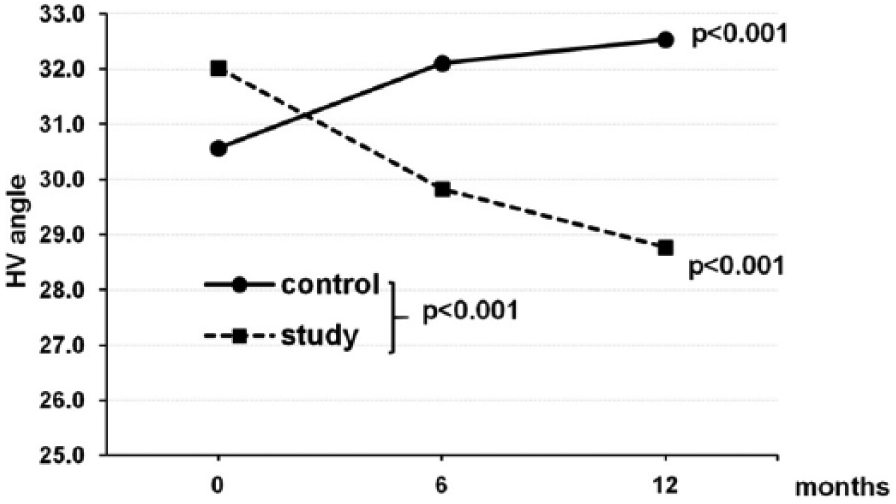
Hallux valgus angles (HVA) at baseline of the study, month 6, and month 12 as reported in per protocol analysis.
For the baseline of ITT, the study group showed a more severe HVA of 32.5° ± 4.8° compared to 30.3° ± 5.2°, which made a significant difference in the HVA between groups (p < 0.05). After 12 months of using the TS, the HVA of the study group improved 3.0° ± 2.4° from 32.5° ± 4.8° to 29.5° ± 5.9°, while the HVA of the control group increased 1.8° ± 1.8° from 30.3° ± 5.2° to 32.1° ± 5.4° (Figure 4). The analysis showed significant differences of HVA between pre- and post-intervention, at months 6 and 12, respectively, in both groups (p < 0.05) (Figures 3 and 4). In Table 2, there were significant differences of HVA at month 12 between both groups as analyzed by a repeated-measures ANOVA with use of the Bonferroni correction for multiple comparisons. Further analysis by an unpaired t-test revealed that there were significant differences of the mean of pre- and post-intervention HVA (months 0–6 and 0–12) between both groups (p < 0.05).
Hallux valgus angles (HVA) at baseline of the study, month 6, and month 12 as reported in the intention-to-treat (ITT) analysis.
Secondary outcomes
Hallux pain is reported in both analysis methods (Table 2). There was no significant difference of hallux pain between two groups at baseline (p > 0.05). Analysis from both methods showed similar outcomes. However, the results show a decrease of hallux pain in the study group. The analysis of hallux pain showed significant differences in pain between pre-intervention and at months 6, 9, and 12 but only for the study group (p < 0.05). The analysis by Mann–Whitney U test revealed that there were no significant differences of hallux pain between two groups at the end of the study.
A summary of compliance with using the RTV silicone toe separator in the study group showed that 42 patients (93.33%) returned their logbooks at months 3 and 6, and only 39 patients (86.67%) returned their logbooks at months 9 and 12. Data from logbooks of the study group showed the highest mean ± SD of compliance in the first 3 months at 7.0 ± 2.7 h/day and 44.7 ± 18.5 h/week and the lowest mean ± SD of compliance in the last 3 months at 6.9 ± 3.6 h/day and 42.6 ± 25.6 h/week.
Complications from using the device were seen in six patients (15% of the study group), but the number of affected patients was not significant according to our sample size. No subjects had serious complications, yet mild pain at the hallux and second toe were noted.
Satisfaction with the RTV silicone toe separator are presented in Table 3. The satisfaction scores were high in every category. The median (range) satisfaction score of the overall treatment of the study group was 9 (3, 10) and only 5 (0, 10) in the control group. There was a significant difference in the overall treatment satisfaction score between two groups (p < 0.001).
Satisfaction with the custom-mold RTV silicone toe separator using the NRS (n = 40).
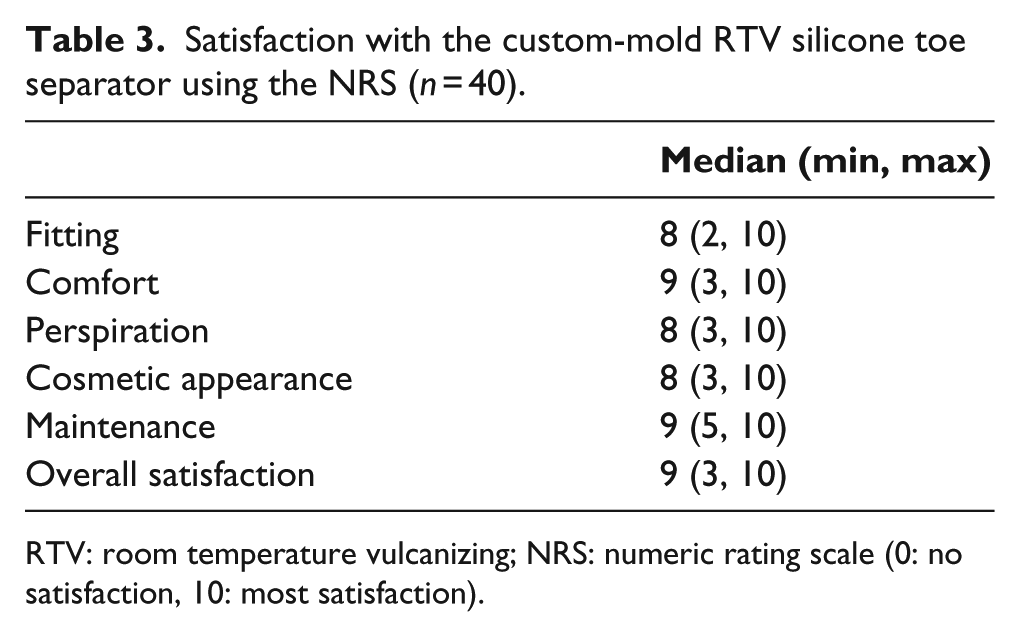
RTV: room temperature vulcanizing; NRS: numeric rating scale (0: no satisfaction, 10: most satisfaction).
As for the intent of the patient to use this device in the future, 31 patients (81.6% of study group) confirmed that they would continue using their devices. Six patients (15.8% of study group) reported that they might continue using their devices and one patient stated she would stop using the device and made no reference as to why.
Discussion
Our study examined the role a low-cost silicone custom-mold toe separator for HV had on reducing HVA, pain, and compliance as well as the satisfaction of the device. The results demonstrated a significant decrease in HVA in the study group and an increase in HVA in the control group which was provided with a proper shoe only. Previous investigations with interventions focused on management of HV have suggested that a reduction in HVA might be due to a prolonged corrective positioning of the hallux, which facilitates stretching of the soft tissues and strengthening of the abductor hallucis muscle. 14
The results presented from both ITT and PP methods provided significant differences of mean HVA for comparisons between the study and control group. The PP analysis method excluded participants dropping out while ITT included all participant data. The significant difference seen in the ITT is more indicative of real clinical situations and helps to identify the effect of the intervention. Participants felt the custom-mold RTV silicone TS was comfortable to wear. Personalizing the TS takes into consideration the unique and individual anatomy of the patient. Previous studies comparing custom and off-the-shelf interventions for HV observed an increase in comfort when using custom-fabricated devices. 24
The complications of the TS were reported during the first 3-month period of use. A limited number of patients needed minor adjustment due to discomfort of the second toe space. Mild pain at the hallux as a result of unaccustomed adjustment was observed in these cases but later subsided. These patients felt satisfied to continue using the TS with no further reports of disuse or complications.
Participant compliance was highest in the first 3 months but lower for the remaining duration of treatment. A previous study comparing the compliance of nighttime HV strap elicited use of 5–6 h per night while the compliance of RTV silicone toe separator was higher at about 7 h. In addition, the custom-mold RTV silicone toe separator elicited the greater HVA reduction at 3.3° ± 2.4°, while a study using a commercial nighttime HV strap presented the mean difference of HVA at −0.8° ± 3.7°. 27
The cost of the custom-made RTV silicone toe separator is approximately US$30 each, whereas the commercially custom-made TS made from medical grade silicone is approximately US$250 each. Therefore, the custom-mold RTV silicone toe separator not only enhances clinical effectiveness in the treatment of HV, but it is also a cost-effective option.
Previous literature has revealed an intrinsic role pes planus plays in exacerbating HV, 5 and intervention such as foot orthoses might influence HV.22,23 Our rationale for omitting measurements of baseline pes planus was due to the fact that our device was intended for use in non-weight bearing during sleeping hours. Taking into account the role of pes planus in interventions designed to address HV is an important point that can be considered in future research.
Conclusion
The prescription of custom-mold RTV silicone toe separator during the night for 1 year as treatment for patients who have a moderate degree of HV decreased the HVA and hallux pain and provided good satisfaction with the device without serious complications. The benefits of using this conservative treatment method could appeal to practitioners desiring to provide a low-cost and effective device for individuals with HV.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Siriraj Research Development Fund (managed by Routine to Research: R2R).