
Abstract
The effects of tuning the AFO footwear combination (AFOFC) for an adult with post-stroke hemiplegia were investigated. Gait analysis and tuning were carried out using a Vicon 3D motion analysis system and two force plates. Tuning of the AFOFC was accomplished by gradually modifying its design over a number of gait trials, to achieve optimal (i.e., as close as possible to normal, within the capability of the patient) knee kinematics and alignment of the Ground Reaction Force vector (GRF) relative to the knee joint. Heel wedges and a stiff rocker were used to tune mid-stance and terminal stance, respectively. Temporal-spatial parameters and selected kinetic and kinematic variables were compared between the non-tuned AFOFC, the tuned AFOFC immediately after tuning, and the tuned AFOFC after three months. There were several changes after three months compared to the non-tuned AFOFC, including improvement in stride length and a reduction in knee hyperextension. A subjective reduction in knee pain and improvement in function were also reported. The feasibility and the lack of objective evidence of tuning AFOFCs as a part of a clinical service need to be addressed in future research.
Introduction
Ankle-Foot Orthoses (AFOs) are commonly prescribed for patients with hemiplegia. 1 Optimizing the design of both the AFO and footwear, by tuning the AFO Footwear Combination (AFOFC) in order to improve gait, has been identified as vital in various gait disorders. 2–4 The key features of the AFOFC design which have been identified as relevant for optimization of gait during tuning are: The alignment of the ankle joint Ankle Angle in the AFO (AAAFO), 4,5 alignment of the lower leg relative to the vertical when standing in the AFOFC-Shank to Vertical Angle (SVA), 2–4,6 and the design of the shoe's heel and sole. 2–4,7 Modification of the AFOFC design during the tuning process aims to optimize gait. In the current study, optimization of gait is defined as normalizing joint kinematics, and the moment
arm of the ground reaction force vector (GRF) relative to the knee joint as far as possible; this aims to correct abnormal joint moments created by pathological gait.
While previous studies have demonstrated the effects of tuning of AFOFC on the gait of children with Cerebral palsy, 8–10 few have addressed the effects of tuning the SVA and footwear design of AFOFC in adults with gait abnormalities. One study of a patient with post-traumatic hemiplegia investigated the effects of tuning the AFOFC. 11 This study reported short and long-term improvements in the moment arm acting at the knee joint, and a reduction in knee pain. While the case study demonstrated the use of tuning to alleviate the specific gait abnormality and resultant pain suffered by the patient, the kinematics and moments of the knee joint were not reported. Although the AAAFO was stated to be ‘neutral’, the footwear sole design was not stated. Furthermore, the optimized SVA was not reported, which is considered important in the tuning of AFOFC. 4 Objective data are needed to investigate the use of tuning to address specific gait abnormalities. Hence, the aims of this case study are:
(a) To demonstrate the process of tuning of the AFOFC to address a specific gait abnormality in an adult with hemiplegia - in this case, knee hyperextension during stance phase; and
(b) To investigate immediate and short-term effects of tuning on the gait of an adult with hemiplegia, using objective data such as kinematics and moments of the knee joint, walking speed and stride length.
Case presentation
The case presented is of a 61-year-old female with a left hemiplegia, 15 months post-stroke. She presented with left-sided hypertonicity, especially in the calf muscles, and reduced muscle power on the left, particularly in the ankle dorsiflexors. She was ambulant with one stick and had been using a solid custom-made polypropylene left AFO of 4 mm copolymer for seven months prior to the study. The AFO was cast at 90°, which was assessed to be appropriate for the length and tone of gastrocnemius. The available length of gastrocnemius allowed passive dorsiflexion of the ankle (with the knee extended) up to neutral. The current AFO was five months old, worn with her own footwear, and had not been tuned in a gait laboratory. The AFO and footwear were flexible at the metatarsal phalangeal joints (MTPJs). The patient complained of swelling and pain in her left knee, sufficient to require analgesia and prolonged periods of non-ambulation to rest the knee.
Data collection and analysis
Tuning was carried out as a part of routine clinical gait analysis (Visit 1). Written consent was obtained from the patient to allow the use of the data for research purposes; this is routinely requested and is required by the National Health Service (NHS) research ethics guidelines for case studies. A follow-up gait analysis session (Visit 2) was carried out three months later in the same motion analysis laboratory, based on the assumption that the patient would have become accustomed to the prescription during this time. The laboratory contained a Vicon 612 3D motion analysis system with eight cameras and a sampling frequency of 100 Hz. Two AMTI force plates with a sampling frequency of 1000 Hz were embedded in the middle of a 10 m walkway. Data were processed using Vicon Plug-in-Gait (PiG) software, 12 which uses a Woltring filter to filter the kinematic data; 13 the force plate data was not filtered.
The method of tuning was in line with previous suggestions, 2,3,7 and aimed at optimizing the kinematics and GRF orientation in relation to the lower limb joints, especially the knee joint during various stages of the gait cycle, within the capability of the patient. The optimal kinematics and orientation of the GRF were judged by a physiotherapist with over 10 years of experience of regularly tuning AFOFCs in a gait laboratory. There was particular focus on mid-stance and terminal stance, as the patient's main concern was knee pain, which was considered by the expert to be due to knee hyperextension during mid-stance and terminal stance. The knee kinematics and orientation of the GRF were deemed to be optimal for this patient at the point where there was no knee hyperextension during mid-stance and terminal stance, and a timely knee flexion during pre-swing. Decisions as to whether kinematics and GRF orientation were optimal for the patient were made by the expert, based on visual feedback from the Vicon system. For this patient, mid-stance (10–30% of gait cycle) was tuned first, followed by terminal stance (30–50% of gait cycle), and pre-swing (50–60% of gait cycle). The procedure through which optimal alignment was achieved for this patient is explained below.
Fifteen retro-reflective markers were attached to the pelvis and lower limbs of the patient, as required by the PiG model; 12 none of the markers were moved or changed during the session.
Visit 1. Tuning was achieved through four trials during the first visit. For each trial, the SVA was measured in standing, modifications to the footwear were made, and the patient performed walks along the walkway until three walks with clean strikes of the hemiplegic leg on either of the force plates were obtained. Data were processed using Vicon PiG software to create ankle, knee and hip joint centres on the moving stick figure with the GRF superimposed; this was displayed on a monitor in the Vicon workstation software interface.
Trial 1. During the first trial (Visit 1, trial 1), the patient wore her original AFOFC (SVA 0°). It was observed from the Vicon footage that there was knee hyperextension in mid-stance and terminal stance, and the GRF orientation was excessively anterior to the knee joint from mid-stance onwards.
Trial 2. During the second trial (Visit 1, trial 2) the heel to sole height differential was increased through the addition of wedges at the heel, modifying the SVA in standing to 12° inclined. It was observed that, although somewhat reduced, the knee hyperextension in mid-stance and terminal stance remained and that the GRF was still oriented anterior to the knee joint from mid-stance onwards.
Trial 3. During the third trial (Visit 1, trial 3) more wedges were added to further increase the SVA to 14° inclined. From the Vicon footage it was observed that while knee hyperextension was reduced during mid-stance, it was still present during terminal stance and there was delayed knee flexion during pre-swing. The orientation of the GRF was optimized for mid-stance, but remained anterior to the knee joint through terminal stance to pre-swing.
Trial 4. During the fourth trial (Visit 1, trial 4) a stiff rocker sole was added to tune terminal stance and pre-swing, while maintaining the SVA at 14°. It was observed that there was no hyperextension of the knee joint during terminal stance and earlier flexion of the knee during pre-swing. The orientation of the GRF was posterior to the knee joint during terminal stance and pre-swing. Trial 4 was judged to have achieved the optimum design of AFOFC to optimize knee kinematics and kinetics, within the individual's capability. All modifications made to the AFOFC were repeated on the opposite leg to maintain symmetry. Permanent modification was made to both shoes (Figure 1).
Visit 2. Gait analysis was repeated after the patient had used the tuned AFOFC for three months.
The tuning process was mainly focused on the knee; therefore, data were analysed by comparing kinematic and kinetic parameters relating to the knee between the trials of Visit 1 and Visit 2. Walking speed and stride length were also compared to identify any improvements in overall walking ability. Comparisons were made between graphs demonstrating knee kinematics and values representing key points in knee kinematics, and external knee moments during the gait cycle. To demonstrate the tuning process, a comparison was made between trials 1, 3 and 4 of Visit 1. To demonstrate the immediate and short-term effects of tuning, a comparison was made between Visit 1 trial 1 (non-tuned), Visit 1 trial 4 (immediately after tuning) and Visit 2 (after three months). Visit 1 trial 2 was not included in any data analysis because no part of the gait cycle was optimized at this stage.
Results
The results showing important changes are summarized in Table 1 and Figure 2.
With the non-tuned AFOFC (trial 1), the SVA was insufficiently inclined and knee hyperextension was apparent (Table 1 and Figure 2). For trial 3 the SVA had been modified to 14° inclined (Table 1), and knee hyperextension in mid-stance was eliminated (Figure 2; Visit 1, trial 3). However, abnormal knee hyperextension persisted during terminal stance. For trial 4 the SVA was maintained at 14° inclination (Table 1), knee hyperextension in terminal stance was eliminated, and knee flexion during pre-swing improved (Figures 2; Visit 1, trial 4).

Ankle Foot Orthosis Footwear Combination - with shoes permanently modified according to the prescription.
Mean (SD) temporal, spatial, kinematic and kinetic parameters between Visit 1, Trials 1, 3 and 4 and Visit 2, three months later.

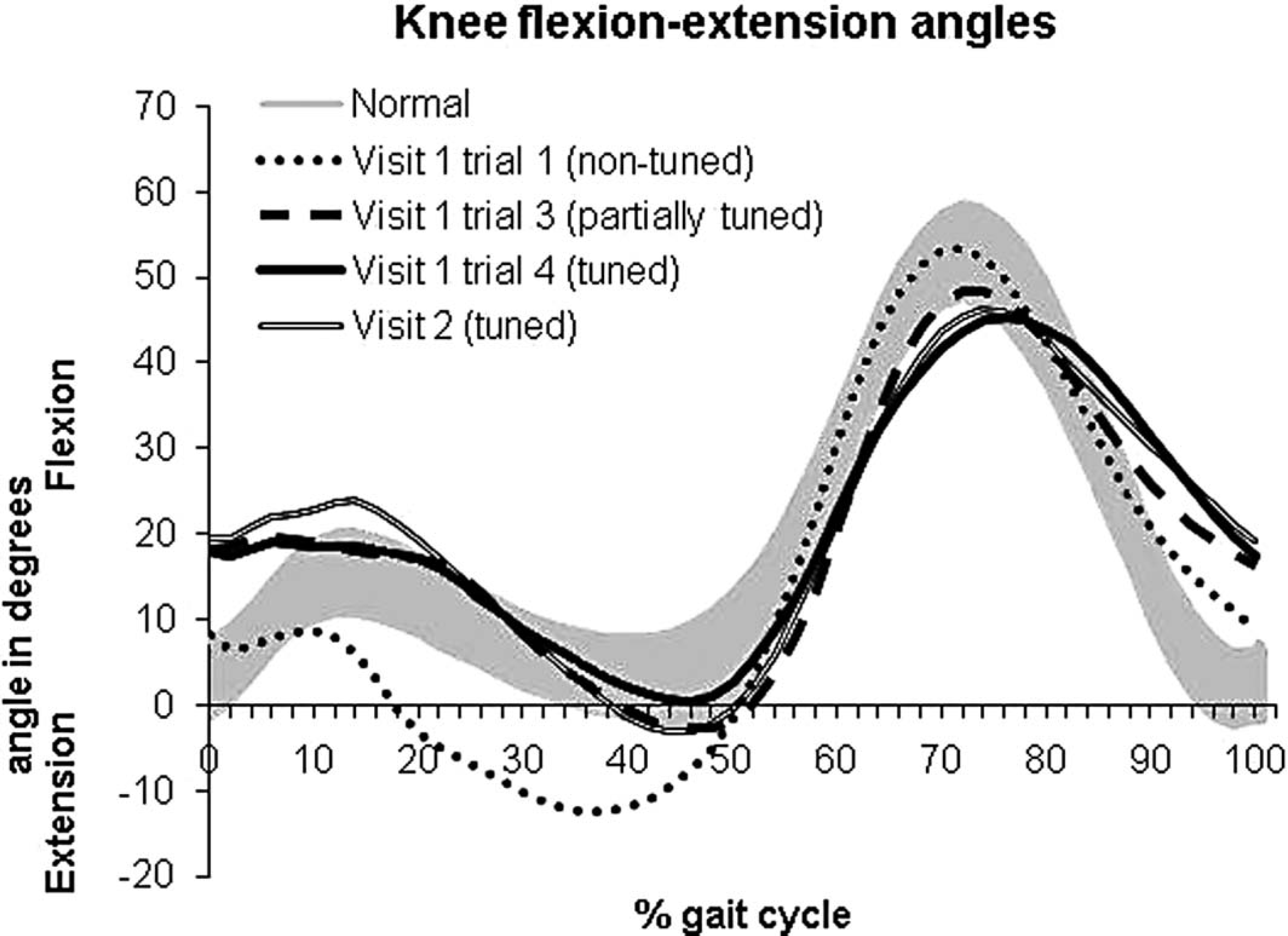
Knee joint flexion-extension angle during gait cycles of Visit 1, trial 1 (non-tuned AFOFC), Visit 1, trial 3 (partially tuned AFOFC), Visit 1, trial 4 (tuned AFOFC) and Visit 2 (tuned AFOFC). Shaded area denotes normal (± 1 SD).
While there was a reduction in stride length immediately after tuning (Figure 2, Visit 1, trial 4), it increased at Visit 2. Knee hyperextension during stance phase was eliminated after tuning (Figure 2, Visit 1, trial 4), but there was slight knee hyperextension at Visit 2. There was an increase in knee flexion at initial contact after tuning, which increased further at Visit 2. The peak knee flexion moment increased after tuning and decreased at Visit 2, whereas the peak knee extension moment decreased after tuning and increased at Visit 2 (Table 1).
Discussion
The patient demonstrated knee hyperextension in mid and terminal stance (10–30% and 30–50% of gait cycle, respectively) (Figure 2; Visit 1, trial 1). Elimination of hyperextension in mid-stance was achieved during trial 3 of tuning, in which the SVA had been modified to 14° inclined using wedges. Previous studies have reported the use of heel raises to optimize the mid-stance orientation of the GRF in relation to the knee joint, reducing the knee extending moment arms in an adult with hemiplegia, 11 and knee hyperextension during stance in children with CP. 9
Finally, the persistence of abnormal knee hyperextension during terminal stance in trial 3 of the current study may have been due to insufficient heel-rise. Elimination of knee hyperextension in terminal stance and improvement of knee flexion during pre-swing were achieved with the addition of a stiff rocker, which promoted heel-rise. A previous study in children with Cerebral palsy has recommended reduction of knee hyperextension through the use of a stiff rocker and a heel raise to control GRF orientation from mid-stance onwards. 7
In the current study, the reduction of knee hyperextension with tuning was only partially maintained at three months, with 4° of hyperextension occurring during terminal stance. Reduction in the peak knee extension moment was also only partially maintained after three months. This may have happened because the patient was walking slightly faster and with longer steps at three months, which may have required a further increase in SVA to control knee hyperextension. A previous study which investigated the effects of tuned AFOFC on the gait of a patient with hemiplegia reported a reduction in the knee extending moment arm, which was maintained for one year. 11 However, the data compared were collected while walking barefoot, and stride parameters were not reported.
In the current study there was an increase in knee flexion at initial contact to greater than normal immediately after tuning, and after three months. Similar findings were also reported after tuning of AFOFC of children with Cerebral palsy. 9 The clinical significance of this effect should be established with further research.
One limitation of the current study was that tuning was performed in order to address a specific gait abnormality - hyperextension of the knee. Hence, the main focus of this case study was the knee joint. The effects of tuning to address other gait abnormalities and joints require further investigation. In addition, as this is a case study, the findings cannot be generalized.
At the three-month visit, the patient reported that she was well adapted to the new prescription and the pain and swelling were eliminated. She could walk further and without the aid of a stick, and no longer required analgesic pain management. She commented that tuning had been ‘a life-changing experience’ because of the reduction in pain and improvement in walking.
Conclusion
This paper provides detailed data regarding temporal-spatial, kinematic and kinetic changes at the knee joint during gait, following different stages of tuning an AFOFC. It illustrates a reduction in knee hyperextension, which had not been obtained with a non-tuned AFOFC. The current study and previous studies indicate the potential clinical utility of tuning of AFOFCs. Although tuning of AFOFCs has been recommended for clinical practice in Scotland, 4 the feasibility of tuning as part of a routine clinical service, and within gait laboratories, for patients with stroke needs to be comprehensively addressed. Research is warranted to further investigate both the short- and long-term effects of tuning AFOFC design on gait and other outcome measures, such as passive joint range of movement, pain, and ‘participation’ in life.