
Abstract
The aim of this study was to assess the functional effects and mechanical contribution of Ankle Foot Orthoses (AFO) prescribed to overcome drop-foot gait. We hypothesized that poor functional effects of the AFO relate to insufficient mechanical contribution of the AFO during the swing phase, or unwanted constraining of the ankle during the stance phase. In seven patients with Stroke or Multiple Sclerosis, we determined changes in energy cost of walking resulting from wearing an AFO, as a measure of the functional effects. In addition, an instrumented gait analysis was performed, and the mechanical AFO properties were measured, to calculate the mechanical contribution of the AFO. The AFO was sufficiently stiff to effectively support the foot in swing, without hampering the ankle during stance. For the whole group, there was a significant improvement in walking speed and energy cost (12%). However, the AFO had no functional benefit in terms of a reduced energy cost of walking for three patients, who coherently demonstrated no pathological plantar flexion during swing without their AFO. We conclude that functional benefit from the AFO was only found when the mechanical AFO characteristics met the need to support the patients‘ mechanical deficiencies.
Introduction
Ankle Foot Orthoses (AFOs) are frequently prescribed to treat gait-related problems in patients with central neurological disorders, such as Stroke and Multiple Sclerosis (MS). The observed problems include limited foot clearance in the swing phase, poor foot placement at initial contact, and a reduced stability in the stance phase. 1–3 Several studies have demonstrated that AFOs can be an effective way to improve the gait of patients with central neurological disorders, 1–3 although the observed changes in walking speed are not always clinically relevant. 2 However, in some studies no functional effect of the AFO was found. 4 From clinical observations it is known that the AFO is effective for some patients, whereas for others an AFO can have poor or even adverse effects.
The attuning between the mechanical properties of the AFO and the patient's specific gait related problems might explain the variation in effectiveness of the AFO. Sumiya et al. reported that the mechanical properties of an AFO, and specifically its stiffness, should be tailored to the patient's gait related problem for it to be effective. 5 In the case of “drop-foot” gait (i.e., paresis of the dorsal flexors with no spasticity of the calf muscles), an AFO is prescribed to assist dorsal flexion during the swing phase. However, if the mechanical properties of the AFO are not specifically tailored to this problem, this could lead to suboptimal effects. For example, if the AFO is not stiff enough, the moment provided by the AFO is not sufficient to keep the foot in dorsal flexion during swing. On the other hand, if the AFO is too stiff, it may hamper the function of the ankle during stance, resulting in an obstruction of dorsal flexion during mid-stance and terminal stance, and a reduced ability to perform work during pre-swing. In concordance, Lehmann et al. 6 suggested that (too) stiff AFOs may hamper ankle plantar flexion at heel strike, resulting in an increased knee flexion moment.
There is little information in the literature about the mechanical contribution of the AFO to the wearer's gait, because the mechanical properties of AFOs have rarely been quantified. We recently developed a device to measure the mechanical properties of AFOs, 7 with which the stiffness and the neutral angle of AFOs can be measured with good reliability. This makes it possible to calculate the ankle joint moments and powers that can be attributed to the AFO throughout the gait cycle.
The aim of this study is to determine the functional effect of the AFO, and the fraction of ankle joint moments and powers that can be attributed to the AFO, in gait of patients for whom an AFO was prescribed to assist the foot during the swing phase. We hypothesise that poor functional effects of the AFO relate to either insufficient contribution of the AFO during the swing phase, or unwanted constraining of the ankle during the stance phase.
Methods
Subjects
Seven subjects participated in this study, which was restricted to chronic Stroke patients and Multiple Sclerosis (MS) patients. Only patients to whom an AFO of the type Dynafo (Maramed Orthopaedic Systems, Hialeah, FL, USA) or Orteam (Livit Orthopaedics, Haarlem, The Netherlands) had been prescribed to assist the foot during the swing phase were included in the study (i.e., the Dynafo AFO is of the “Posterior Leaf Spring” type, and the Orteam is an AFO trimmed posterior to the malleolli with dorsal notches for flexibility). Patients were randomly recruited from a local supplier's database. Patients had to be able to walk faster than 0.5 ms−1, and had to have received their AFO during the previous three years. All patients signed informed consent forms prior to the start of the study, and the study protocol was approved by the Medical Ethical Committee of the VU University Medical Center. The subject characteristics of the seven patients are presented in Table I.
Measurement procedures
For each subject, the experimental session started with a measurement of energy consumption, both walking with shoes only, and walking with both shoes and AFO. During a short break, the investigators determined the mechanical characteristics of the AFO. In the
Subject characteristics.

Spasticity was measured using the SPAT. 9 (0 = normal or increased muscle resistance over the whole Range of Motion (ROM); 1 = Increase in muscle resistance somewhere in ROM without catch; 2 = catch and release; 3 = clear catch, blocking further movement.
catch at 0 degrees dorsal flexion. Berg Balance Scale: (0–20 = balance impairment; 21–40 = acceptable balance; 41–56 = good balance). 8
second half of the experimental session, the balance without AFO was assessed using the Berg Balance scale, 8 and the spasticity of the m. gastrocnemius and m. soleus was assessed with the SPAsticity Test (SPAT). 9 Both measures were taken to give a general impression of the patients included in the study. Finally, a 3-D gait analysis including force plate measurements was performed, again with the patients walking with shoes only, and walking on both shoes and AFO.
Energy Cost of walking
The Energy Cost (EC) of walking was measured with the portable VmaxST measurement system (Sensormedics, Bilthoven, The Netherlands). The procedure started with a measurement of energy consumption at rest, during which the subject was seated in a chair for 10 min. Subsequently, the subject was asked to walk at a comfortable, self-selected speed on a 50-m oval for 6 min, both with and without the AFO. Between the two 6-min walking trials there was a 10-min rest period. The order of the walking trials was randomised. During the two walking trials, the distance travelled was registered to calculate walking speed.
AFO mechanical characteristics
The BRUCE device 7 was used to determine the stiffness and neutral angle of the AFO around the ankle joint, whereby the neutral angle is defined as the angle at which no forces are exerted onto the AFO. The BRUCE device was specifically designed to measure AFO characteristics reliably. As schematically shown in Figure 1, its design is based on a replicated human leg that is manually driven and continuously registers joint configuration and force exerted onto the device by the AFO. 7 Measurements were made for the ankle part of the AFO, according to a protocol in which data are acquired within an interval ranging from 10 degrees plantar flexion to 20 degrees dorsal flexion. 7
Kinematics and kinetics
3-D Kinematics were recorded with the Optotrak system (Northern Digital, Waterloo, Canada) while the subject walked on a 10-m walkway. Clusters of three markers were firmly attached to the subjects’ trunk and pelvis, and to the thigh, shank and foot of the affected leg. Anatomical landmarks were indicated to define anatomical co-ordinate systems. 10 Circumferences and lengths of the leg segments were measured to calculate the inertial parameters of the leg segments. 4,11
Synchronously with the 3-D kinematic data, ground reaction forces were recorded on a built-in force plate (AMTI, Watertown, USA). Recordings of the subject were made walking with shoes only, and walking with shoes and AFO. Subjects walked at a comfortable, self selected speed. For both conditions three trials with the subject stepping on the force plate were used for further analysis.
Analysis
Energy Cost of walking
For each walking trial, the energy consumption was calculated from oxygen uptake and RER, using the data acquired within the last 2 min of the walking trial. 12 The energy
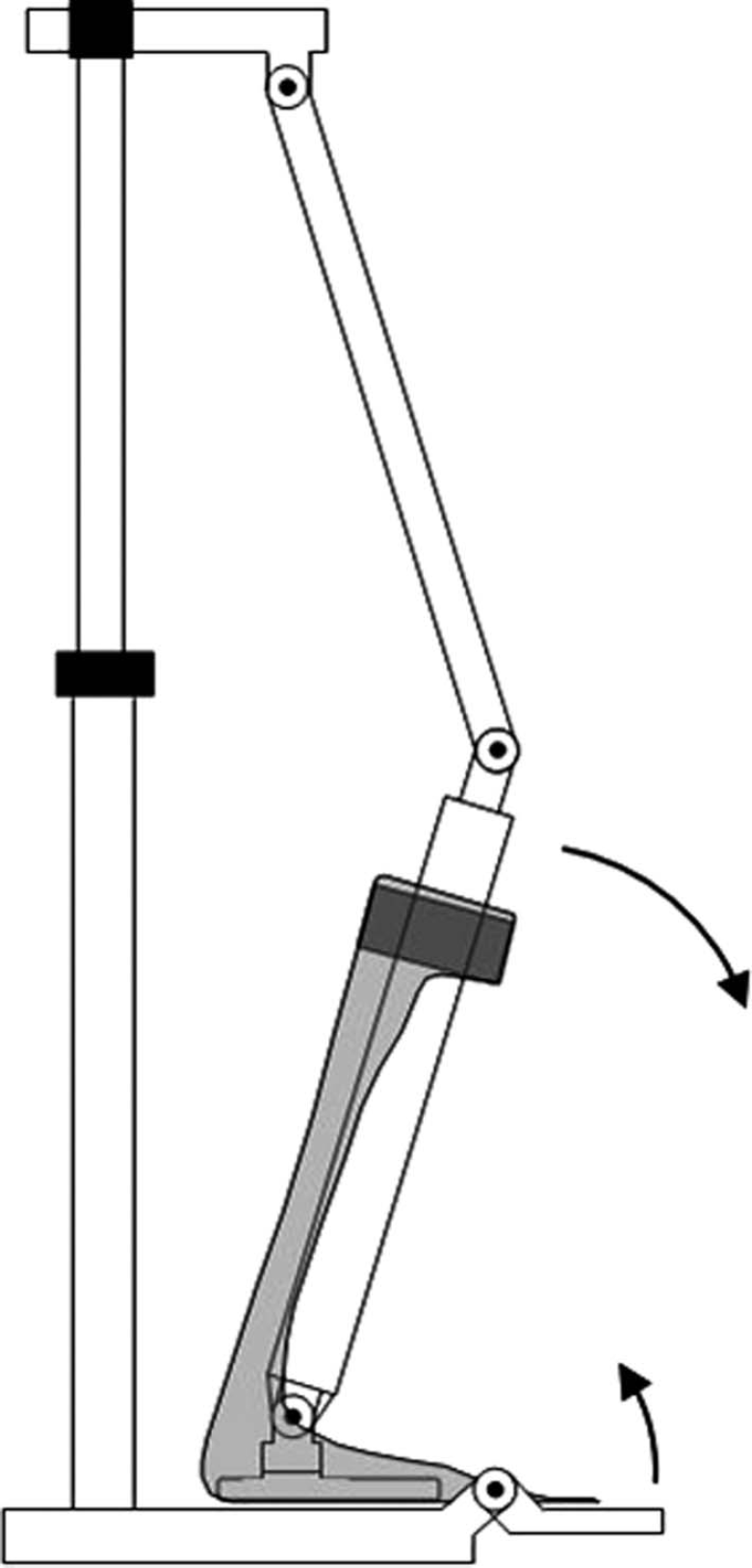
A schematic representation of the BRUCE device, 7 which was used to test the mechanical AFO characteristics around the ankle joint.
consumption at rest was subtracted from the energy consumption during walking to calculate the net energy consumption during walking, which was then divided by the walking speed to calculate the net energy cost of walking in J m−1. Finally, data were normalized for body mass, to calculate the net Energy Cost of walking in J m−1 kg−1. We defined a decrease in energy cost of more than 10% to be clinically relevant. 12
AFO characteristics
The stiffness and neutral angle of the AFO around the ankle joint were determined with a least-squares linear fit in the interval ranging from 10 degrees plantar flexion to 20 degrees dorsal flexion. 7 Prior to determining the ankle stiffness and neutral angle, all data were checked for non-linearity that may have been caused by buckling of the lateral sides of the AFO. 7 If necessary, the interval was adapted to exclude the non-linear data. To be able to compare the ankle angle obtained from instrumented gait analysis and the neutral angle of the AFO, we measured the inclination of the shoe using a custom-made inclinometer.
Kinematics and kinetics
The 3-D kinematic data were analyzed in a Matlab-based (The Mathworks, Natick, USA) open-source software package (www.bodymech.nl). For each walking trial, initial contacts were determined, based on the force plate data and the minimum horizontal acceleration of the virtual heel marker. 13 Subsequently, the instances of initial contact were used to normalise data from 0–100% stride-time, using a spline interpolation. Inertial and mass properties were calculated with the regression equations by Zatsiorski. 11 Net joint moments were calculated for the ankle with the method provided by Hof. 14 The ankle joint power was calculated from the dot product of the joint angular velocity and the ankle joint moment. The ankle joint work was calculated as the integral of the net ankle moment and the angular displacement. The positive ankle joint work was defined as all positive ankle work performed throughout the gait cycle. The moment around the ankle joint provided by the AFO (the AFO moment) was calculated by multiplying the AFO stiffness by the difference between the ankle joint angle and the AFO neutral angle. To do so, the neutral angle of the AFO was corrected for the inclination angle of the shoe, and for the difference between the definition of the anatomical axis and the definition used in the AFO tester. The subject's ankle moment was calculated by subtracting the AFO moment from the net ankle joint moment. The relative contribution of the AFO was calculated by dividing the absolute AFO moment by the sum of the absolute AFO moment and the moment provided by the subject. Next, the AFO moment and the subject's moment were used to calculate the ankle joint power provided by the AFO, and the ankle joint power provided by the subject, respectively.
Statistical analysis
Because of the small group size, we used non-parametric statistics. We used the Wilcoxon Signed-Rank test to assess whether there were differences in the functional parameters for walking with and without the AFO. The level of significance was set at p < 0.05.
Results
Energy cost of walking and walking speed
At the group level, we found a significant decrease of 12.1% (± 10.6) in EC of walking when patients walked with the AFO (Table II). One patient did not complete the 6-min walking test, so the decrease in EC was calculated from the data of six patients only. Data on walking speed was obtained for all seven patients. The mean walking speed was significantly higher (0.10 ± 0.12 ms−1) when patients walked with the AFO.
According to our predefined criterion three patients benefitted from the AFO in terms of a reduced energy cost of walking. The patient for whom there was no data available on the EC of walking was considered to benefit from the AFO, based on an increase in walking speed from 0.48 to 0.75 ms−1. The results for the EC of walking and the walking speed were also separately averaged for the subjects that benefited (benefit group) and subjects who did not (non-benefit group), which can be seen in Table II.
AFO properties
All prescribed AFOs were made out of polypropylene. Three AFOs were of the type Dynafo (Maramed Orthopaedic Systems, Hialeah, FL, USA), and four AFOs were of the type
Orteam (Livit Orthopaedics, Haarlem, The Netherlands). In the benefit group, three AFOs were Orteams, and one AFO was a Dynafo. In the non-benefit group, two AFOs were Dynafos, and one AFO was an Orteam. The prescribed AFOs were characterised by a mean stiffness of 0.19 (± 0.04) Nm deg−1. As can be seen in Table III, the AFOs were positioned in 1.0 (± 7.2) degrees dorsal flexion.
Kinematics
Walking with the AFO resulted in changes in the ankle kinematics in the benefit group, whereas in the non-benefit group the ankle kinematics remained constant (Figure 2). In the benefit group, two clear changes in ankle kinematics were observed. First, the ankle during swing shifted from a mean plantar flexed position of 8.2 (± 6.3) degrees to a mean plantar flexed position of 0.1 (± 5.6) degrees (Figure 2, Table IV). Second, the ankle angle at initial contact shifted from a plantar flexed position of 14.0 (± 6.6) degrees to a plantar flexed position of 1.8 (± 4.9) degrees. In the non-benefit group, a dorsal flexed position during swing and a dorsal-flexed position at initial contact were observed when walking with shoes only (Table IV). In the non-benefit group, the peak ankle dorsal flexion was timed slightly earlier in the stance phase when walking with the AFO (Figure 2). In both groups there was no difference between kinematics of the knee and hip joint when walking with and without the AFO. However, the knee and hip kinematics did differ between the benefit group and the non-benefit group when walking with and without the AFO. At the knee, more flexion during
Functional effects of the AFO.

Statistical difference between walking on shoes and with the AFO.
AFO characteristics.
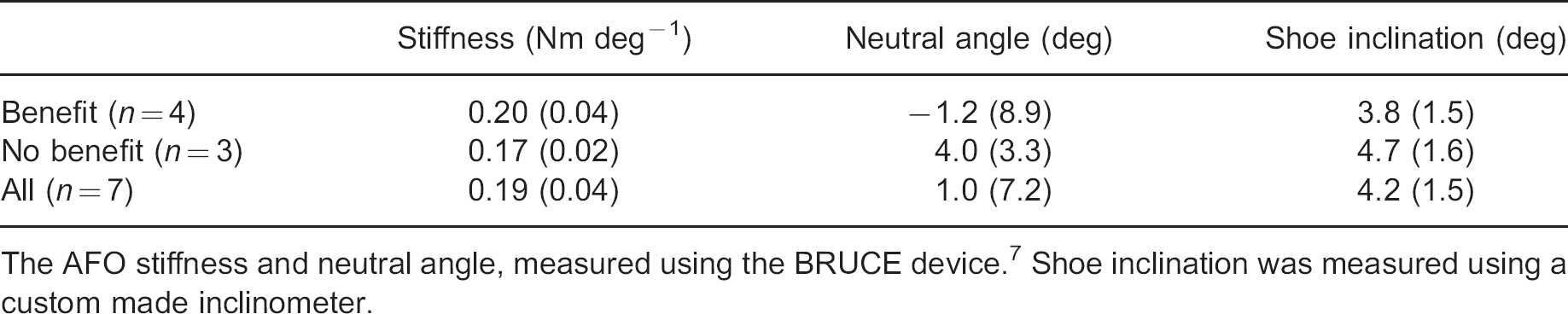
The AFO stiffness and neutral angle, measured using the BRUCE device. 7 Shoe inclination was measured using a custom made inclinometer.

Walking without AFO benefit group: dark solid line; walking with AFO benefit group: light solid line; walking without AFO non-benefit group: dark dashed line; walking with AFO non-benefit group: light dashed line. Shading represents normal gait. 17
swing was observed in the non-benefit group. At the hip, more flexion was observed in the non-benefit group.
Kinetics
Ankle joint moment
The AFO did not evoke any pertinent changes in the ankle joint moment in the benefit group or the non-benefit group. In both groups the major part of the ankle moment during stance was provided by the subject, rather than the AFO (Figure 3). In the benefit group, the AFO accounted for 13.7 (± 1.9) percent of the total ankle joint moment. In the non-benefit group the AFO contributed 7.2 (± 1.5) percent to the total ankle joint moment (Figure 3, Table IV). The moments provided by the AFO during swing were small for both the benefit group and the non-benefit group, but the relative contribution of the AFO was of greater influence as moment provided by the subjects was small.
Ankle joint power and ankle joint work
In both the benefit group and the non-benefit group no major changes in the ankle joint power were found as a result of wearing the AFO. In the benefit group, the peak ankle powers were lower than in the non-benefit group. For both groups, the contribution of the AFO to the total power around the ankle joint was marginal, as can be seen from Figure 4 and Table IV. No major changes in the positive ankle joint work were found in either group as a result of wearing the AFO.
Discussion
The aim of this study was to determine the functional effects and the mechanical contribution of AFOs that were prescribed to assist the foot during the swing phase in patients with a central neurological disorder. We hypothesized that poor functional effects of the AFO relate to either insufficient contribution of the AFO during the swing phase, or unwanted constraining of the ankle during the stance phase.
The prescribed AFOs were characterized by a mean ankle stiffness of 0.19 Nm deg−1. During swing, this stiffness was sufficient to keep the foot in neutral position. Obviously, for
Mechanical contribution of the AFO.

Statistical difference between walking with and without AFO, at group level.

Walking without AFO: light solid line; walking with AFO: dark solid line; contribution of the subject: dashed line; contribution of the AFO: dotted line. Shading represents normal gait. 17

Walking without AFO: light solid line; walking with AFO: dark solid line; contribution of the subject: dashed line; contribution of the AFO: dotted line. Shading represents normal gait. 17
three patients who already walked with their ankle in neutral position without an AFO, the AFO did not contribute to a neutral ankle position in swing. Consequently, these three patients did not functionally benefit from their AFO in terms of a reduced energy cost of walking, and these three patients might have received their AFO in vain. This questions the effectiveness of current clinical decision making, and stresses the need for careful indication. However, a larger, more representative group of patients is required to demonstrate whether current clinical decision making is adequate or not. Nonetheless, the corresponding lack of a functional benefit from using an AFO in just those three patients
reinforces a clear link between the mechanical contribution and functional effect of the AFO at the level of the individual patient.
Our second hypothesis was that the AFO should not induce any undesirable constraints around the ankle during the stance phase. More specifically, if the AFO is too stiff, the function of the ankle during stance may be hampered, resulting in a restricted allowance for dorsal flexion, and a reduced ability to perform work around the ankle joint. From our kinematics analysis it appeared that dorsal flexion around the ankle during mid-stance and terminal stance was unaffected by the AFO. It also seems unlikely that, as suggested by Lehmann et al., 6 the AFO caused an increased knee flexion moment at foot strike in our study, given the low AFO stiffness in use and the fact that no differences in knee kinematics were found when walking with or without the AFO. In concordance, the mechanical analysis revealed that during the stance phase the contribution of the AFO was negligible, compared to the ankle joint moment provided by the patient. Likewise, the powers attributable to the AFO were small. Also, the positive work performed around the ankle was not affected by the AFO. Taking all this into consideration, it seems unlikely that the functioning of the ankle throughout the stance phase was hampered by the AFO.
The contribution of the AFO to the ankle joint moment found in our study was small, compared to the contribution of the AFO found in the double case-study carried out by Stanhope et al. 15 This is not surprising, given the low average AFO stiffness of 0.19 Nm deg−1 in our study, compared to the carbon-composite AFO stiffnesses of 2.52 Nm deg−1 and 4.60 Nm deg−1 reported by Stanhope et al. 15 Our findings that the baseline characteristics of the patient (e.g., Berg Balance Scale differences between benefit (53.0) and non-benefit group (43.8)) and the correct indication for the AFO largely determine whether beneficial effects of the AFO obtained are in line with the findings reported by de Wit et al. 2 In their study, 14 out of 20 patients reported beneficial effects of their AFO, with patients who had better motor functioning of the leg reporting less beneficial effects of the AFO.
This study is limited by the small number of patients we included. Moreover, the patients formed a fairly heterogeneous group, differing both in disorder and walking ability. To avoid the suggestion of a group conclusion, we reported the data for each patient individually. Despite the heterogeneity at group level, we still found an effect, and two groups could be distinguished, presumably because energy cost of walking is a responsive outcome parameter, that even allows usage at individual level. 12 A further limitation of this study is that the walking speed differed between walking conditions with and without the AFO, thereby introducing possible speed-dependent changes in kinematics and kinetics and maybe even energy cost of walking. For example, an increased walking speed when walking with the AFO might introduce slightly more plantar flexion in late stance. 16 However, keeping walking speed fixed with and without AFO interacts with the fact that the change in walking speed is also an important outcome measure, indicating the functional benefit of an AFO. Furthermore, we did not measure any functional outcomes such as stability or the ability to walk up stairs, which may be alternative reasons for wearing an AFO in daily life, and consequently, alternative outcome parameters. In addition, some patients might only benefit from an AFO over the time course of a complete day, which was not accounted for in our study design.
In future research, attention should be paid to the match between patient-specific gait-related problems, and the mechanical properties characterising the prescribed AFO. Greater insight into the match between the AFO and patient is expected to improve the specific prescription of the AFO, and thus provide more functional benefit from the AFO. In this study we analyzed the mechanical contribution of AFOs with a fairly low stiffness.
Future research should focus on the mechanical contribution of AFOs with various stiffnesses, for example by analysing variations in the AFO stiffness within individual patients.
In summary, we found that the mechanical contribution of AFOs with a low (± 0.19) stiffness that were prescribed to overcome drop-foot gait is very low, but yet enough to keep the foot in neutral position during swing. We found that these AFOs with low stiffness did not hamper the ankle throughout the stance phase. We found a clear link between the mechanical effect and the energetic functional effects of the AFO, which demonstrates the clinical importance of using an AFO, provided that it is properly prescribed. Furthermore, this study demonstrates that research on the relationship between AFO characteristics, the mechanical functioning of the AFO, and the resulting functional effects is needed to gain insight into the effectiveness of the orthoses and the appropriateness of orthotic prescription at the individual level.