
Abstract
Background:
Different types of ankle-foot orthoses are commonly used following lower limb surgery in children with bilateral spastic cerebral palsy. After three-dimensional gait analysis 1 year postoperatively, many children are recommended continued use of ankle-foot orthoses.
Objectives:
Our aims were to quantify the impact of ankle-foot orthoses on gait 1 year postoperatively and evaluate predictors for clinically important improvement.
Study design:
Prospective cohort study.
Methods:
A total of 34 ambulating children with bilateral cerebral palsy, with mean age 11 years (range 6–17), comprising 12 girls and 22 boys, were measured with three-dimensional gait analysis preoperatively (barefoot) and 1 year postoperatively (barefoot and with ankle-foot orthoses). Outcome was evaluated using gait profile score, key kinematic, kinetic and temporal–spatial variables in paired sample comparisons. Logistic regression was used to evaluate predictors for clinically important improvement with orthoses (⩾1.6° change in gait profile score).
Results:
Walking barefoot 1 year postoperatively, major improvements were seen in gait profile score and key variables. With ankle-foot orthoses, there were significantly improved step length and velocity, additional moderate reduction/improvement in gait profile score and knee moments and decreased stance ankle dorsiflexion compared to barefoot. Children using ground reaction ankle-foot orthoses (n = 14) decreased stance knee flexion from 13.9° walking barefoot to 8.2° with orthoses. High gait profile score and more gait dysfunction preoperatively were significant predictors of clinically important improvement walking with orthoses.
Conclusion:
The results indicate improved gait function walking with ankle-foot orthoses versus barefoot 1 year after lower limb surgery. Stronger impact of ankle-foot orthoses was found in children with more pronounced gait dysfunction preoperatively.
Clinical relevance
The 1-year postoperative three-dimensional gait analysis is a useful method to assess treatment outcome after lower limb surgery in children with bilateral cerebral palsy and could also guide clinicians whether further treatment with ankle-foot orthoses is indicated, using clinically important differences as thresholds to evaluate their impact on gait.
Keywords
Background
Ambulating children with bilateral spastic cerebral palsy (CP) often experience a decline in gait function as they grow older, mainly seen as ankle equinus or energy-demanding crouched gait.1–3 Severity of the gait impairment and the occurrence of contractures may necessitate lower limb surgery.2,4 Ankle-foot orthoses (AFOs) are routinely used as part of the postoperative rehabilitation regimen with the objective to maintain the surgical corrections, prevent the recurrence of preoperative deformities and improve gait by providing adequate mechanical support.4–6
A survey including families where the children underwent multilevel surgery revealed that the use of AFOs was a major challenge during the rehabilitation period. 7 Many children have expectations that the orthoses could be discontinued following the 1-year postoperative evaluation with three-dimensional gait analysis (3DGA). Nevertheless, the postoperative 3DGA frequently leads to recommendations for continued use of orthoses.8,9 Due to the risk of developing pes calcaneus and crouch gait in children with bilateral CP, particularly after tendo-achilles lengthening and with low age at surgery, 10 it has been suggested that discontinuation of AFOs should be advised only when gait data confirm satisfactory plantar flexion and knee extension coupling.5,11
Valuable information has previously been provided regarding the effect of orthoses on gait function in children with bilateral CP.12–18 However, we are not aware of any studies that have investigated the impact of AFOs and the indication for continued use by comparing walking with orthoses versus walking barefoot 1 year postoperatively.
The main aim of this study was to quantify the impact of AFOs 1 year after lower limb surgery in children with bilateral spastic CP. A secondary purpose was to identify predictors for clinically important improvement when walking with AFOs. We hypothesised that the use of AFOs provides improvement compared to barefoot.
Methods
Participants
We included children with bilateral spastic CP and level I–III of the Gross Motor Function Classification System (GMFCS). 19 All children underwent lower limb surgery and used AFOs at the 1-year postoperative 3DGA. Consecutive sampling during a 4-year inclusion period resulted in 55 patients who received written information about the study. In total, 34 children (62%), including 12 girls and 22 boys, gave written consent to participate. Of them, 7 children had motor function categorised as GMFCS level I, 19 level II and 8 level III. Their mean age at surgery was 11 years (range 6–17). In total, 146 surgical procedures were performed, 97 in the limbs that were analysed (Table 1). The most common procedures were hamstring lengthening (n = 19), rectus femoris transfer (n = 16), tendo-achilles lengthening (n = 15) and gastrocnemius recession (n = 11). All children were analysed with gait analysis preoperatively (barefoot) and 1 year postoperatively (barefoot and with orthoses). Kinetics from four children who used ambulatory devices that obstructed the force plate data were removed. The study was approved by the South-East Regional Ethics Committee (REC; 2013/1242).
General table with participant characteristics, type of surgery and type of AFO in the analysed limbs, and recommendations regarding AFO use.
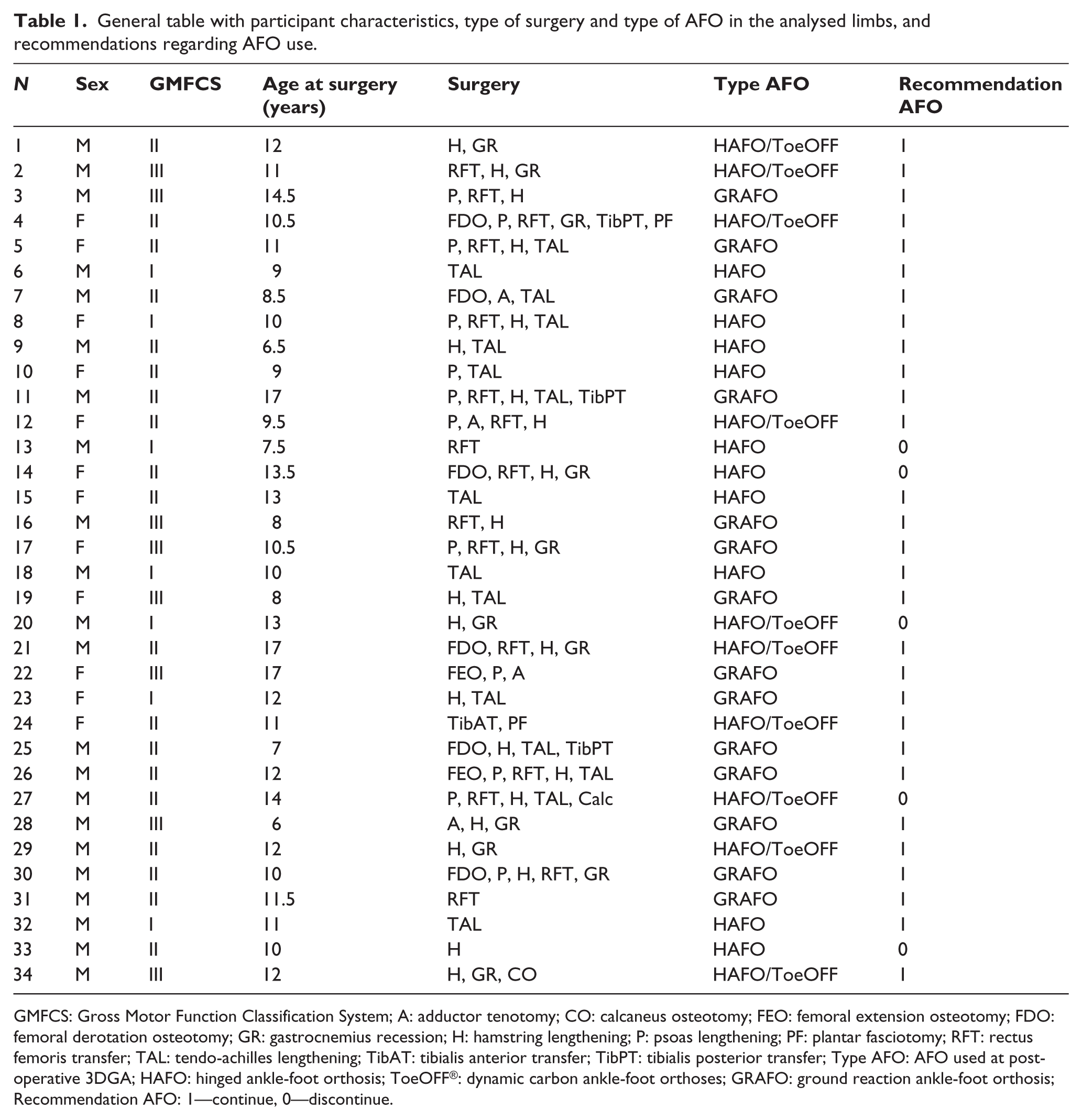
GMFCS: Gross Motor Function Classification System; A: adductor tenotomy; CO: calcaneus osteotomy; FEO: femoral extension osteotomy; FDO: femoral derotation osteotomy; GR: gastrocnemius recession; H: hamstring lengthening; P: psoas lengthening; PF: plantar fasciotomy; RFT: rectus femoris transfer; TAL: tendo-achilles lengthening; TibAT: tibialis anterior transfer; TibPT: tibialis posterior transfer; Type AFO: AFO used at postoperative 3DGA; HAFO: hinged ankle-foot orthosis; ToeOFF®: dynamic carbon ankle-foot orthoses; GRAFO: ground reaction ankle-foot orthosis; Recommendation AFO: 1—continue, 0—discontinue.
Orthoses and rehabilitation
Casting for postoperative AFOs was routinely made peroperatively by certified prosthetist orthotists (CPOs) at the hospital. Physiotherapy commenced 1 day postoperatively and was continued during the whole rehabilitation period. Fitting and tuning of the orthoses took place during 1 week of in-house rehabilitation after protective splints had been removed. Subsequently, the children spent 4 weeks in a rehabilitation centre with intensive stretching, strength and gait training, before receiving community-based follow-up.
Types of AFOs were guided by each participant’s preoperative 3DGA and the treatment algorithms suggested by Rodda and Graham. 5 In children with crouch patterns, AFOs restricted dorsal and plantar flexion and were designed to apply an external knee extension moment during stance, categorised as ground reaction ankle-foot orthosis (GRAFO). In the cases of equinus, the AFOs were constructed to allow dorsiflexion, restrict plantar flexion and lift the foot in swing, categorised as hinged ankle-foot orthosis (HAFO). Pre-fabricated carbon orthoses (ToeOFF®; Allard, USA) were also categorised as HAFO since flexibility in the sole allowed stance ankle dorsiflexion (Figure 1). With shoes, AFOs were aligned using 0°–10° anterior shank-to-vertical inclination. The children were advised to use the AFOs all day until the 3DGA 1 year postoperatively, with control of the orthosis function using video-vector analysis 6 months postoperatively.
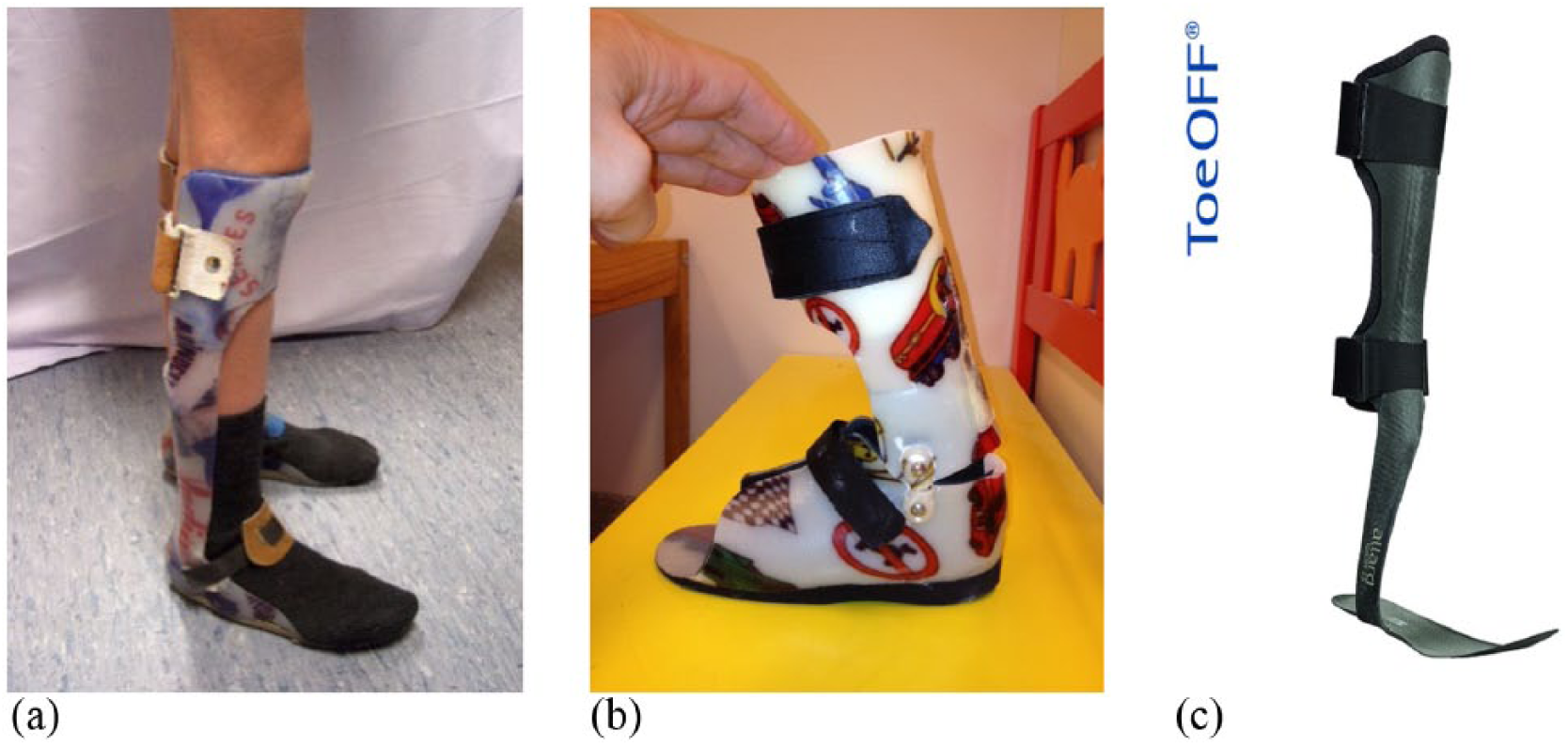
Types of AFOs used at postoperative gait analysis: (a) GRAFOs were fabricated in 5–6 mm polypropylene, fixing the ankle in neutral position and with a ventral shell extending to mid-patella and stiff sole past the toes; (b) HAFOs were made in 2.5 mm polypropylene, dorsal shell and circular, total contact foot part, integrated joints (Tamarack, Blaine, USA) and trimlines to block plantar flexion and allow free dorsiflexion; (c) dynamic carbon composite orthoses (ToeOFF®; Allard, USA) with arch-supporting insoles provided flexible resist to plantar flexion, allowed dorsiflexion over flexible sole, and were also categorised as HAFO.
Gait analysis
Data were collected with participants walking at self-selected speed, using a six-camera MXF40 Vicon system (Oxford, UK) and three force platforms (AMTI OR6-7; Watertown, USA). Markers were placed on anatomical landmarks according to the Plug-in-Gait model. 20 Using standardised protocols, two testers reached agreement about marker placement, forefoot markers were placed proximal to minimise effect of foot deformities, and knee varus/valgus curves were used as quality control of thigh coordinate system alignment. 21
Postoperatively, participants were first measured barefoot, and then with AFOs. With AFOs, markers were placed on the orthoses and shoes, in best possible agreement with the segment and motion axes. To account for differences in heel height, we measured the heel-to-toe drop of the shoe sole. Heel markers were placed accordingly higher from the ground than the forefoot marker using a calliper, and not assumed horizontal with the ground during static processing. Standardised physical examination including joint range of movement, muscle strength and tone took place prior to the walking trials.
As part of routine procedure, a multidisciplinary team consisting of orthopaedic surgeons, child neurologists, CPOs and physiotherapists interpreted the 3DGA data.6,22 Their clinical advice regarding further care and interventions was specified in the patients’ gait reports. We reviewed the postoperative gait reports to assess how many children were recommended continued AFO use and the clinical cause for prescription.
The gait profile score (GPS) 23 was used as a summary measure of gait quality. GPS for the right and left legs were derived from nine kinematic gait variable scores (GVS), using root mean square differences between the patient’s gait curves and averaged gait curves from our reference database of 24 typically developing children. 22 Reduced GPS score indicates gait closer to normal and improvement. GPS reduction ⩾ 1.6° has been defined as a minimal clinically important difference (MCID). 24 Furthermore, we investigated three kinematic, two kinetic and three temporal–spatial outcome variables considered especially relevant to evaluate the impact of AFOs on gait in bilateral CP. This included ankle angle at initial contact, stance maximum ankle dorsiflexion, stance minimum knee flexion, stance maximum external dorsiflexion moment, late stance maximum external knee moment, gait velocity, cadence and step length. Temporal–spatial outcome variables were normalised by body height to account for growth between pre- and postoperative measurements. 25
Statistics
Three gait trials in each condition were averaged, using data from one limb per participant in the statistical analyses (SPSS 21 for Windows; IBM corp., USA). This implied the most affected side when AFOs were used on one side only (n = 9) and the side which underwent most surgery when bilateral orthoses were used. Normal distributions in each outcome variable were tested using Kolmogorov–Smirnov test.
Paired sample t-tests were used to assess changes in outcome variables between the baseline preoperative and 1-year postoperative barefoot conditions, and between AFO and barefoot conditions 1 year postoperatively. Since GRAFOs were thought to differ significantly in mechanical properties from HAFOs, paired t-tests were also used to compare kinematic variables in the subgroups (GRAFOs and HAFOs).
Children who had GPS reduction ⩾ 1.6° walking with AFOs versus barefoot postoperatively were categorised as ‘Improved’ and children with GPS reduction < 1.6° categorised as ‘Not Improved’. Logistic regression was used to evaluate relevant predictors (GMFCS level, sex, age at surgery, preoperative GPS, postoperative GPS) of clinically important improvement walking with AFOs. Factors that were significant in univariable regression analysis were subsequently tested in multivariable analysis. The significance level was set at p < 0.05.
Results
Median time from surgery to postoperative 3DGA was 14 months (range 12–24). At 1 year postoperatively, 14 children used GRAFOs and 20 used HAFOs (10 ToeOFF).
The mean GPS was 17.3° (standard deviation (SD) 4.6°) preoperatively and 12.3° (SD 2.8°) walking barefoot postoperatively. GVS components of the GPS are displayed in the motion analysis profile (MAP; Figure 2). When comparing postoperative barefoot walking with preoperative baseline data, the GPS, key kinematic and kinetic variables were significantly improved, whereas non-dimensional velocity and step length decreased following surgery (Table 2).
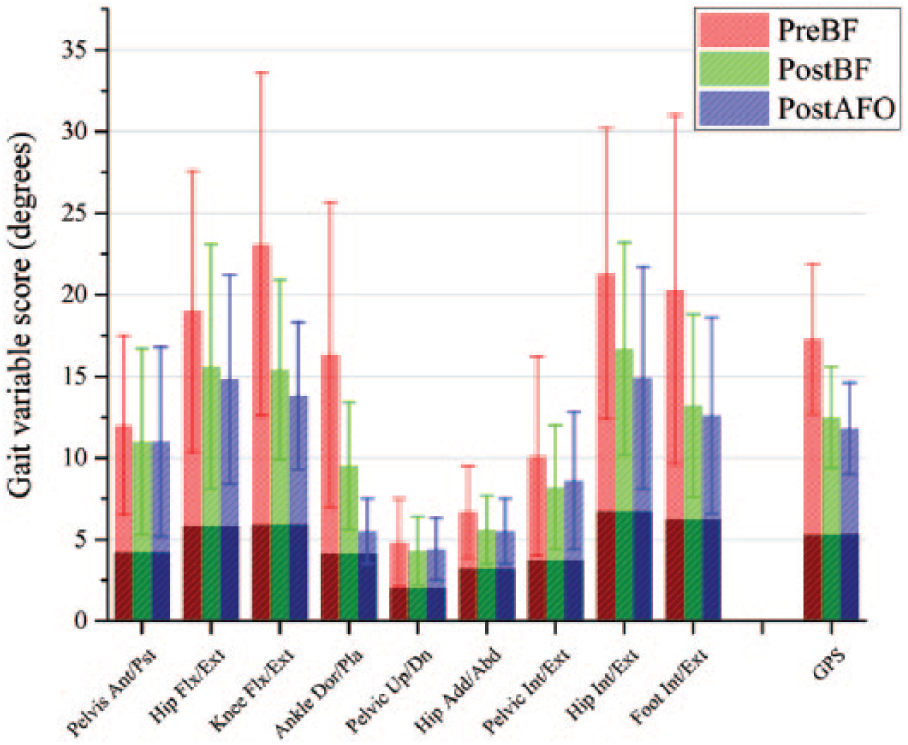
Movement analysis profile with gait variable scores and gait profile scores in three conditions: preoperatively walking barefoot (PreBF), postoperatively walking barefoot (PostBF) and postoperatively walking with AFOs (PostAFO). Each column represents the root mean square difference across the gait cycle averaged for all participants (n = 34), with averaged scores from normal reference data (n = 24) seen as the darker area in the base of each column.
Comparison of gait kinematic, kinetic and temporal–spatial variables.
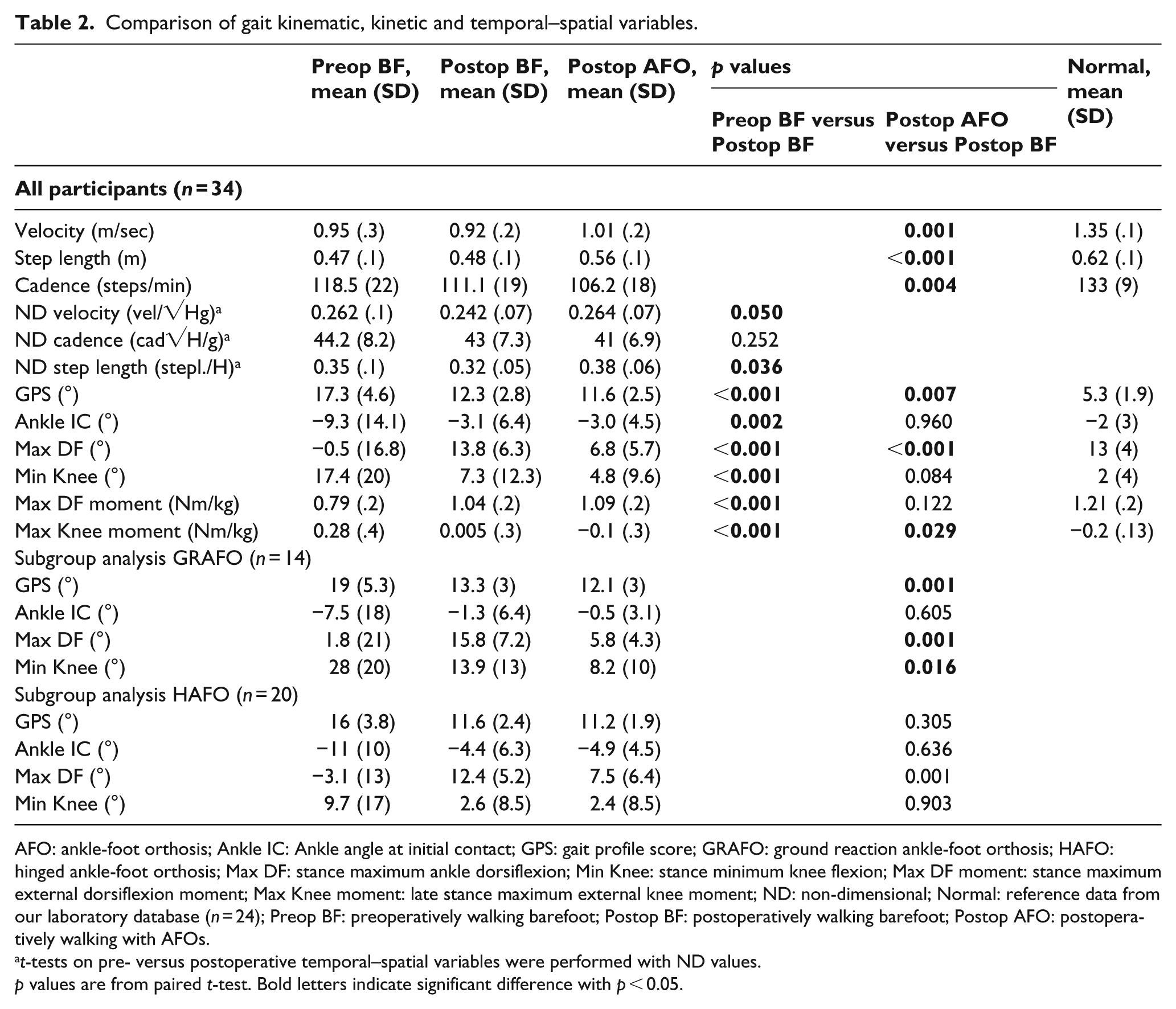
AFO: ankle-foot orthosis; Ankle IC: Ankle angle at initial contact; GPS: gait profile score; GRAFO: ground reaction ankle-foot orthosis; HAFO: hinged ankle-foot orthosis; Max DF: stance maximum ankle dorsiflexion; Min Knee: stance minimum knee flexion; Max DF moment: stance maximum external dorsiflexion moment; Max Knee moment: late stance maximum external knee moment; ND: non-dimensional; Normal: reference data from our laboratory database (n = 24); Preop BF: preoperatively walking barefoot; Postop BF: postoperatively walking barefoot; Postop AFO: postoperatively walking with AFOs.
t-tests on pre- versus postoperative temporal–spatial variables were performed with ND values.
p values are from paired t-test. Bold letters indicate significant difference with p < 0.05.
At 1 year postoperatively, the mean GPS was significantly reduced by an average of 0.7° walking with AFOs compared to barefoot (Table 2). Of the 34 participants, 12 (35%) had a reduction in GPS ⩾ 1.6° with AFOs, indicating clinically important improvement. The remaining 22 patients had change in GPS < 1.6° with AFOs and were categorised as not improved.
In univariable logistic regression, sex and preoperative and postoperative barefoot GPS values were significantly associated with clinically important improvement walking with AFOs (Table 3). In multivariable logistic regression, a high preoperative GPS value was the only significant independent predictor of clinically important improvement (p = 0.026). This indicated that children with more severe gait dysfunction preoperatively had better effect of orthoses 1 year postoperatively.
Group characteristics and results of logistic regression analysis for predictors of clinically important improvement walking with AFOs 1 year postoperatively.
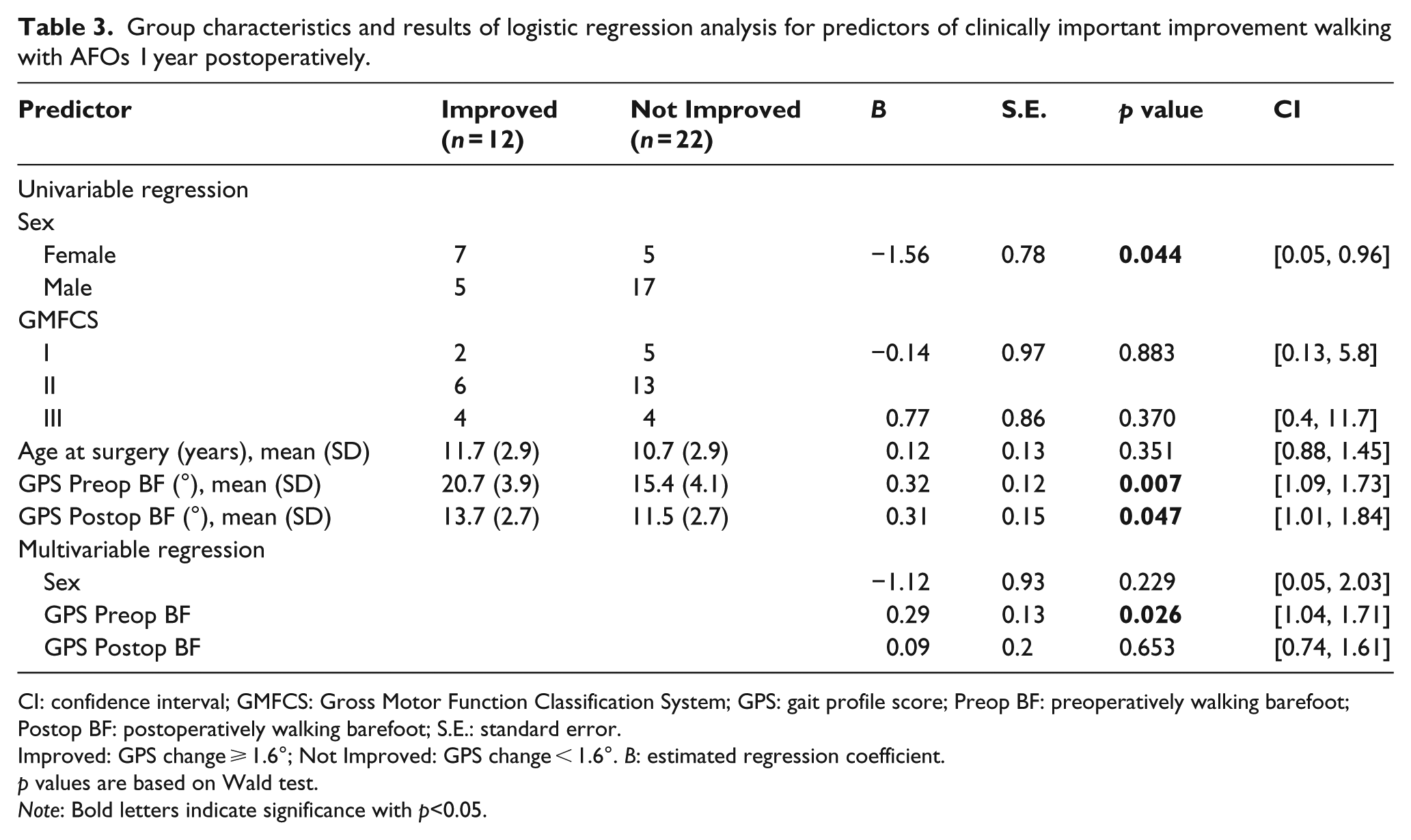
CI: confidence interval; GMFCS: Gross Motor Function Classification System; GPS: gait profile score; Preop BF: preoperatively walking barefoot; Postop BF: postoperatively walking barefoot; S.E.: standard error.
Improved: GPS change ⩾ 1.6°; Not Improved: GPS change < 1.6°. B: estimated regression coefficient.
p values are based on Wald test.
Note: Bold letters indicate significance with p<0.05.
Maximum ankle dorsiflexion was on average reduced by 7° walking with AFOs compared to barefoot (Table 2). Despite increased external knee extension moment with AFOs (p = 0.029), minimum knee flexion in stance was only moderately reduced (from 7.3° to 4.8°, p = 0.084). However, separate subgroup analysis of the 14 participants who used GRAFOs revealed significant improvement in minimum knee flexion (from 13.9° to 8.2°, p = 0.016).
Analysis of temporal–spatial variables revealed significantly increased velocity and step length when the children walked with AFOs, whereas cadence was lower, indicating a more energy-efficient gait compared to the postoperative barefoot condition (Table 2).
In total, 29 children were recommended continued use of AFOs (the same type in 14 and altered AFO type in 15). The most frequent cause for prescription was to reduce stance knee flexion and prevent recurrence of crouch and/or to improve pre-positioning of the foot before initial contact. Only 10 of the 29 children who were recommended continued use had clinically important improvement (GPS change ⩾ 1.6°) walking with AFOs versus barefoot 1 year postoperatively.
Discussion
At 1 year postoperatively, walking with AFOs compared to barefoot caused improved GPS, increased step length and velocity, decreased maximum ankle dorsiflexion and improved knee extension moment with AFOs, and in children using GRAFOs decreased minimum knee flexion. It is difficult to directly relate our findings to similar research because, to our knowledge, no studies exist that have compared walking with orthoses versus barefoot in a defined postoperative period. Previous studies included an unknown proportion of children who underwent lower limb surgery.12,13,16,17
With AFOs, the GPS was reduced with an average 0.7° (SD 1.3°), indicating an improvement of moderate degree. Previous studies using summary measures to evaluate gait with AFOs versus barefoot reported differing conclusions. Ries et al. 16 found significant improvement in the gait deviation index, whereas no difference was found in Gillette gait index 12 or GPS. 15
A clinically important GPS improvement with AFOs versus barefoot was found in 35% of the children. The main predictor for such improvement was high GPS preoperatively, which indicated that patients with more severe gait function had better effect of orthoses. This is in accordance with recent studies where patients with low functional level benefit most from AFOs.14,16 GMFCS level was not a predictor of improvement with AFOs in our study, possibly due to the limited number of patients in each group.
A well-documented effect of AFOs in bilateral CP is reduced dynamic equinus with improved pre-positioning in terminal swing and ankle angles at initial contact.13,15,18 We did not find a difference in this variable (Table 2), most likely because 26 of our participants underwent triceps surae lengthening with ankle angles at initial contact within normal ranges (mean, 2SD) in both postoperative conditions.
The reduction of stance maximum ankle dorsiflexion was significant in the total cohort and in both AFO subgroups. However, the decrease was greater in children who used GRAFOs. This group had severe crouch preoperatively, which was the initial reason why GRAFOs were prescribed. Many children had residual crouch postoperatively, seen as excessive ankle dorsiflexion (mean 15.8°) and knee flexion (mean 13.9°) in stance. The higher prevalence of excessive dorsiflexion postoperatively may have been caused by surgical overlengthening of the triceps surae. Also, immobilisation in rigid GRAFOs could have reduced triceps surae strength and contributed to the plantar flexion, knee extension deficit in this group. Although orthoses effectuated a moderate decrease in stance minimum knee flexion, the difference was not statistically significant. This was not unexpected, since the mean barefoot value was 7° postoperatively and within normal ranges. Children using GRAFOs had more severe gait dysfunction and thus more potential for improvement.14,16 Stance knee flexion decreased significantly, possibly due to ankle dorsiflexion constraint and more efficient force transfer through longer and stiffer lever arms in this AFO type. Our results are in accordance with Rogozinski et al. 17 and Böhm et al. 14 who found that GRAFOs, by restricting stance sagittal plane ankle motion, are effective to diminish crouched gait patterns in children with CP.
Improved temporal–spatial variables walking with AFOs compared to barefoot confirmed the results from previous research with respect to increased step or stride length13,15,16,18 and velocity15,16,18 and reduced cadence.13,15,18 The increase in step length by 7.6 cm was above the threshold for a clinically important difference, whereas changes in velocity and cadence were of medium and small clinical importance, respectively. 26 It should be considered whether temporal–spatial changes with orthoses may be partially due to the addition of shoes. Best practice guidelines, published after data collection for this study, recommended shoes to be used as the control condition when evaluating AFOs. 27 We prioritised barefoot data since these were needed for comparison with preoperative data. In able-bodied children, stride length increased significantly with shoes, 28 whereas in children with unilateral CP 29 no unanimous benefit was found with shoes versus barefoot. Recently, Böhm et al. 14 found no significant differences between barefoot and shoed conditions and concluded that barefoot walking is sufficient as control condition when evaluating the impact of orthoses.
Indications for continued use of AFOs after the 1-year postoperative 3DGA evaluation depend on how well gait is corrected by the surgery and postoperative rehabilitation, and whether residual gait deficits are still present. Comparing pre- and postoperative barefoot values, the average GPS was reduced by 5° postoperatively, indicating gait patterns closer to normal. Nevertheless, the mean postoperative GPS of 12.3° exceeded the normal range, suggesting that the gait problems had not been completely resolved. This may explain why many children (85%) were recommended continued use of AFOs. If a clinically important improvement in GPS had been used as a criterion, some of these children would probably have been advised to discontinue using orthoses. However, GPS was calculated for this study and was not available when the team evaluated the postoperative 3DGA. Recommendations were based on gait data and clinical evaluation. This may have caused prescription of AFOs even where they seemed of minor benefit, possibly to prevent relapse of gait problems or for support in the cases of foot deformities, which could not be determined by the simplified 3DGA model employed.
A recent study questioned whether gait indices such as the GPS are sensitive enough to measure AFO efficiency. 15 We believe that GPS is an appropriate measure of overall gait quality and it has been found reliable and sensitive to detect clinically important differences.24,30 Still, because it is a summary score calculated across several kinematic components, important changes in single components may have been concealed. Therefore, key kinematic variables should also be reported, such as stance maximum ankle dorsiflexion and minimum knee flexion, which are particularly relevant to evaluate crouch gait in children with bilateral CP.
According to the study by Capjon and Bjørk, 7 the use of AFOs was a major challenge during the rehabilitation period. Many children hoped that the orthoses could be discontinued after the 1-year postoperative evaluation, due to discomfort, pain and an overall challenging postoperative regimen. Their findings are consistent with our clinical experience. Therefore, recommendations should be well founded, preferably based on improved gait function. This could help motivate children and parents and clarify why continued use of AFOs is necessary. In future practice, we suggest that the functional purpose of AFOs is specified in each child, using clinically important differences in relevant 3DGA variables as thresholds of efficacy. Special caution should be executed in younger children who could deteriorate when they enter the pubertal growth spurt,1,10 and in children with severe gait dysfunction preoperatively. Children with bilateral CP and previous surgery have higher incidence of crouch, 3 particularly after tendo-achilles lengthening,10,11 which also could indicate prolonged use of orthoses.
There were some limitations in this study. As reported, we did not include a shoes-only control condition. Inclusion of ToeOFF orthoses may have biased analyses in the HAFO group. The number of children was rather small, making statistical analyses of subgroups and predictors of improvement less reliable. There was heterogeneity with regard to motor function, type of surgery and type of orthoses. However, repeated measures using each child as his or her own control eliminated some of the variability. Variance in postoperative follow-up time added heterogeneity to the sample and future studies should control for this factor to diminish bias. Since this study mainly included sagittal plane variables, the differences between the compared conditions were less influenced by known limitations of 3DGA, such as marker placement error 31 and soft tissue artefacts.32,33
Further research should include patient-reported outcomes to evaluate function and satisfaction with the orthoses. Furthermore, the role of AFOs in reducing the risk of relapse after surgery might be relevant to investigate in a longitudinal follow-up study.
Conclusion
Our findings indicate moderately improved gait function walking with AFOs compared to barefoot 1 year after lower limb surgery. Stronger impact of AFOs was found in children with severe gait dysfunction.
Footnotes
Acknowledgements
We thank all participants in the project and acknowledge the contribution of Merete Aarsland Fosdahl, Ann Britt Huse and Kristin Kvalheim Beyer for taking part in data collection.
Author contribution
All authors contributed to the drafting and editing of this article and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported through the PhD grant from Sophies Minde Ortopedi AS. The funding organisation was not involved in the study.