
Abstract
Background:
The use of knee–ankle–foot orthoses with drop locked knee joints produces some limitations for walking in subjects with quadriceps muscle weakness. The development of stance control orthoses can potentially improve their functionality.
Objectives:
The aim of this review was to compare the evidence of the effect of stance control orthoses to knee–ankle–foot orthoses with drop locked knee joints in improving kinematic variables and energy efficiency of walking by subjects with quadriceps muscle weakness caused by different pathologies.
Study design:
Literature review.
Methods:
Based on selected keywords and their composition, a search was performed in Google Scholar, PubMed, ScienceDirect, and ISI Web of Knowledge databases. In total, 18 articles were finally chosen for review.
Results:
The results of this study demonstrated that this type of orthosis can improve the walking parameters of subjects with quadriceps muscle weakness and spinal cord injury patients when compared to a locked knee–ankle–foot orthosis.
Conclusion:
There is evidence to show that stance control orthosis designs improve the gait kinematics but not energetic of knee–ankle–foot orthosis users. Development of new designs of stance control orthoses to provide a more normal pattern of walking is still required.
Clinical relevance
Stance control orthoses are a new generation of orthotic intervention that could potentially be significant in assisting to improve the gait kinematics by knee–ankle–foot orthosis users.
Background
Knee–ankle–foot orthoses (KAFOs) are lower extremity devices which extend over the knee, ankle, and foot. KAFOs are prescribed for people with lower limb muscle weakness; particularly in quadriceps muscles.1–3 KAFOs are prescribed for varying muscular weakness of the lower limb including poliomyelitis, post-polio syndrome, cerebrovascular accident (CVA), cerebral palsy (CP), spinal cord injury (SCI), and multiple sclerosis (MS) to provide stability of the lower limb during locomotion. 2 Lower limb weakness, especially knee extensor weakness, is a condition that alters normal gait patterns, 4 and this condition may result in decreased stability during daily tasks. 5
Conventional KAFOs provide stability during walking by locking the knee joint in a fully extended position during both stance and swing phases. This requires excessive energy consumption and induces abnormal gait events such as circumduction, hip hiking, and vaulting during gait.6,7 Walking with conventional KAFOs can also lead to premature exhaustion during ambulation, as well as limited mobility, pain, and a decreased range of motion (ROM) in lower limb joints.3,8 It has been reported that using a conventional KAFO reduces gait efficiency by 24%, increases vertical displacement of the center of mass (COM) by up to 65%, and also increases energy expenditure. 9 Due to these factors, the rejection rate of using KAFOs in patients with muscular weakness of the lower limb due to conditions such as poliomyelitis, post-polio syndrome, CVA, CP, SCI, and MS has been reported as being between 60% and 100%. 9
Stance control KAFOs (SCKAFOs) are a new generation of KAFO which have been developed to prevent knee flexion during stance phase and permit free knee motion during swing phase of gait. 10 Mechanical SCKAFOs are usually activated by ankle ROM mechanisms or limb inclination. The UTX, stance control orthosis (SCO) knee joint, swing phase lock (SPL), Horton, Otto Bock Free Walk, and the Otto Bock Sensor Walk are all examples of SCKAFOs.8,11
Using a SCKAFO produces an increased acceptance rate for wearing orthoses by patients with poliomyelitis, CP, CVA, and leg muscle weakness because of the ability to control knee flexion in stance and the provision of free knee flexion during swing phase of gait.3,8,12 Studies have demonstrated that velocity, cadence, stride length, and step length can increase when walking with a SCKAFO versus a locked knee KAFO.2,3,8,12 Irby et al. 11 reported that KAFO users showed improvements in velocity, cadence, and stride length after 6 months of walking with the dynamic knee brace system (DKBS). SCKAFOs improve gait by encouraging more normal gait patterns, improving mobility, reducing the energy cost of walking, and reducing compensatory strategies that may lead to chronic pain and loss of motion.2,12–14
Unfortunately, current commercial SCKAFOs are often noisy, bulky, heavy, and expensive and in some cases are not effective in improving kinematic variables and energy expenditure. Davis et al. 12 reported that there was no difference in the energy cost of walking or physiological cost index (PCI) between a SCO and walking with the locked knee joint orthosis. Bernhardt et al. 1 reported that it was slightly more difficult to sit down and stand up with the new SCKAFO. Zissimopoulos et al. 8 showed that differences in oxygen cost could not be detected between the auto and locked modes of a SCKAFO. Only one study analyzed the engineering structure of this type of orthosis. 15 The effects on all walking parameters while using this type of orthosis in comparison to a conventional KAFO are not clear. Therefore, the aim of this literature review was to summarize the research on walking parameters while using these orthoses in various patient groups.
Research questions
Energy expenditure and kinematic variables were used as a framework to define the following research questions:
With regard to energy expenditure: do subjects with quadriceps muscle weakness caused by different pathologies achieve reduced energy expenditure immediately and over time when using SCKAFOs compared with conventional KAFOs?
With regard to kinematic variables: do persons with quadriceps muscle weakness caused by different pathologies achieve a higher speed of walking, cadence, step length, knee ROM, reduced pelvic obliquity, and vertical and lateral displacement immediately and over time when using SCKAFOs compared with conventional KAFOs?
Method
Search strategy
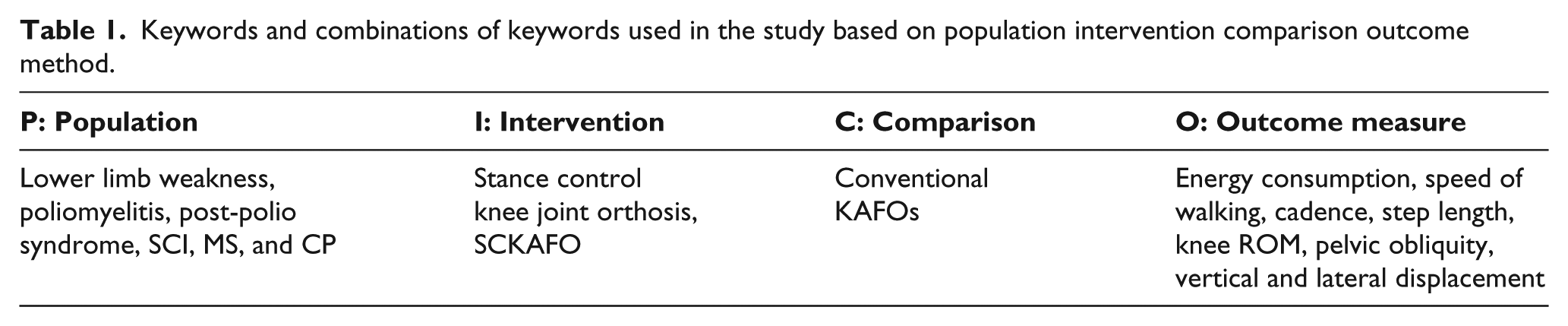
An extensive electronic search was carried out through internationally published scholarly articles in Google Scholar, PubMed, ScienceDirect, and ISI Web of Knowledge (from 1950 to 2013) with the selected keywords (Table 1): stance control knee joint orthosis, stance control knee ankle foot orthosis, energy consumption, and temporal spatial parameters. The aforementioned keywords were also searched in combination with lower limb weakness, poliomyelitis, post-polio syndrome, spinal cord injury, multiple sclerosis, and cerebral palsy. Search by selected keywords was organized following the population intervention comparison outcome (PICO) model. In order to provide a specific selection of previous studies, different combinations of the topics can be made with the use of AND, OR, and NOT. To prepare a more accurate and comprehensive search, the references of primary resultant articles were also included to find more suitable articles. The strategy includes medical subject headings (MeSH) and text words.
Keywords and combinations of keywords used in the study based on population intervention comparison outcome method.
The title and abstract of each individual study were screened by authors. The first criterion to select appropriate articles was whether the title has addressed the research questions of interest. The second step in acquiring proportional articles was performed based on the following criteria:
Studies which were considered for inclusion were randomized controlled trials (RCTs), case–control trials, cohort studies, case series studies, and single-case studies.
The article was written in English.
The study evaluated motorized (powered) or mechanical SCO using over training time in poliomyelitis subjects.
The study investigated individuals with a lower limb weakness (poliomyelitis, post-polio, and SCI) and able-bodied subjects.
The main outcome measures of the article were balance, gait, energy consumption, kinetics, kinematics, and tempo-spatial parameters.
The PICO was used to define the included studies. Figure 1 depicts the article selection procedure utilized. Ultimately, 18 studies were included in the review. All the subjects in these studies were persons with polio, post-polio, SCI patients, and able-bodied subjects.
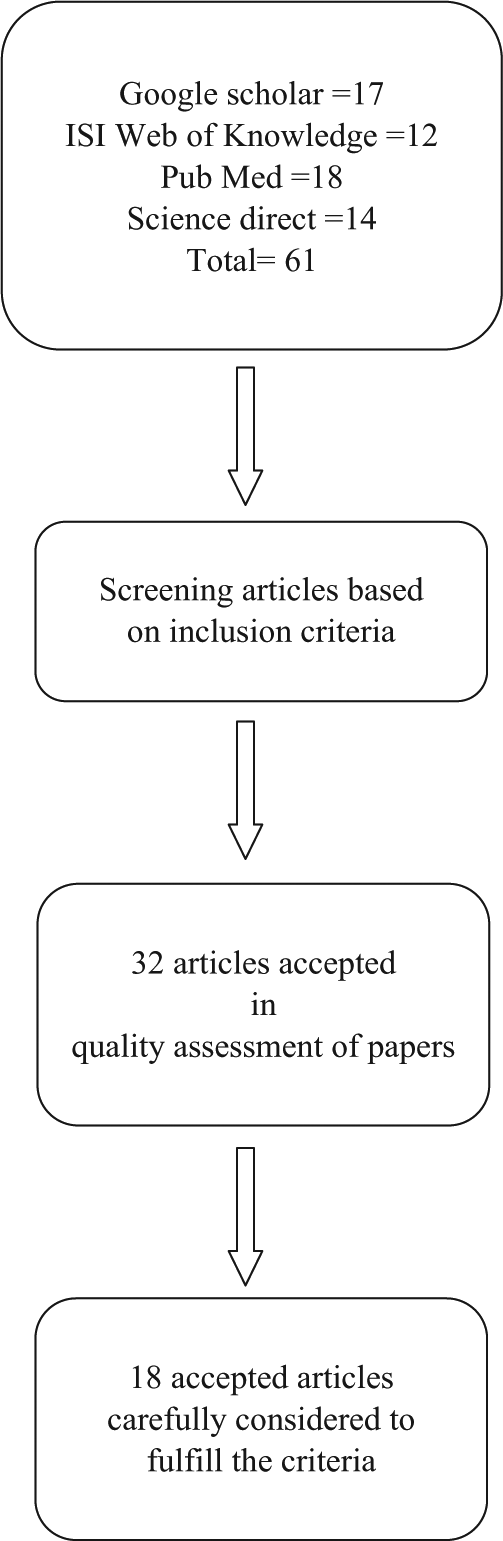
The article selection procedure utilized in this study.
Results
Table 2 summarizes the characteristics (participants, parameters, procedure, and results) of studies which evaluated SCOs compared to KAFO when worn during ambulation.
The characteristics (participants, parameters, procedure, and results) of studies that evaluated the stance control orthosis on knee–ankle–foot orthosis users.

SCKM: stance control knee mechanism; FNS: functional neuromuscular stimulation; HNP: hybrid neuroprosthesis; IRGO: isocentric reciprocating gait orthosis.
Research question 1: the energy efficiency of SCKAFOs
Interestingly, only three studies evaluated energy consumption in non-disabled subjects, subjects with lower limb pathology, and a patient with post-poliomyelitis when using a SCO.8,11,13 A trend to improved energy efficiency has been demonstrated in two studies (0.447 beats/min in using a SCO compared to 0.554 beats/min in locked KAFO, and 0.21 beats/min in using SCO compared to 0.25 beats/min in locked KAFO).8,13 However, one study reported an increased PCI when using a SCO compared to a locked KAFO (0.70 beats/min compared to 0.65 beats/min, respectively). 11
Research question 2: the kinematic efficiency of SCKAFOs
Speed of walking
Typical walking speed has been reported as being 1.3 m/s during normal walking in healthy subjects. 16 When using a powered SCO, this can reduce to only 0.57 m/s. 16 The mean of this variable has been shown to be 1.18, 8 0.82, 2 0.8, 13 0.59, 11 0.63, 20 1.04, 3 and 0.61 17 in various subjects when using a non-powered SCO for ambulation. Only three studies demonstrated an increase in walking speed compared to walking with a locked KAFO,8,11,12 while five studies reported a reduction in this parameter when wearing a SCO.3,16,17,19,20 An improvement in walking velocity has also been reported when using a stance control knee joint compared to drop locked knee joint in wearing an RGO in SCI patients (0.12 and 0.23 m/s).10,18
Cadence
Six studies noted an increase in cadence during walking with a SCO compared to walking with locked KAFO.2,3,8,11,12,21 However, Hebert et al. when using an automatic SCO and Arazpour et al. when using a powered KAFO both detected a reduction in this parameter compared to walking with locked KAFOs.13,16 Using a SCO associated with an RGO caused a reduction in this parameter in SCI patients. 10 The mean cadence in these studies was between 53 and 102 steps/min.
Step length
Nine studies analyzed step length in various subjects (poliomyelitis subjects, SCI patients, other pathologies, and able bodied) while walking with a SCO. An increase in this parameter was reported in three studies.2,3,12 However, three studies reported reduction in this parameter when using a SCO compared to a locked KAFO.16,17,20 One study reported similar results when ‘using a joint that can be switched between locked knee and stance control modes’ (mean: 0.6 m), 8 but a second study demonstrated a reduction in step length compared to a locked KAFO. 13 The mean of step length reported in these studies was between 50 and 70 cm. Two studies using a SCO in combination with an RGO by SCI patients demonstrated the mean of this parameter to be 0.46 and 0.36 m.10,18
Knee ROM
The knee joint needs 67° of flexion during swing phase in healthy subjects during normal walking. 16 Using a SCO reduces this mean to 40° in healthy subjects. 16 The reported mean of this parameter was 62.9°, 1 47°, 24 50°, 61°, 21 and 43° 25 when SCOs are used compared to KAFO with drop locked knee joints (2°–5°). The mean knee joint ROM during swing phase was 50° when walking with a SCO associated with an RGO in SCI subjects compared to RGO with drop locked knee joints. 10
Pelvic obliquity
Pelvic obliquity was analyzed in three studies when SCO was compared to KAFO with drop locked knee joint in able-bodied, poliomyelitis, and various subjects.2,8,14 Irby et al. 2 in gait evaluation of SCOs by 14 SCO users during a 6-month clinical field trial announced that all subjects had significantly lower pelvic obliquity, 2.8 mm (p = 0.04) compared to baseline. Zissimopoulos et al. 8 studied the biomechanical and energetic effects of a SCO knee joint on the gait of nine non-disabled persons and reported significant differences between the locked mode and unlocked mode (p = 0.003) and auto mode and locked mode (p = 0.01). Yakimovich et al. evaluated the kinematics of a new SCKAFO on three male KAFO users with knee extensor weakness. The new SCKAFO improved pelvic obliquity and provided a more natural gait for orthosis users compared to conventional KAFOs. 14
Vertical and lateral displacement
Reduction in the mean of lateral displacement has been reported when using SCO compared to locked KAFO. Arazpour et al., 16 in using a SCO in healthy subjects, demonstrated the decreased rate of this parameter from 8.2 to 5.8 mm. In other study, Arazpour et al. 17 in evaluation of powered SCO on one poliomyelitis subject reported a reduction in lateral displacement from 8.6 to 5.8 mm. Hwang et al. 21 in an evaluation of electromechanical SCOs worn by four poliomyelitis subjects demonstrated a reduction in this parameter from 292.8 to 196.7 mm.
Similar to lateral displacement, reduction in vertical displacement has been demonstrated when walking with a SCO compared to a locked KAFO in poliomyelitis subjects. Both Arazpour et al. 17 and Hwang et al. 21 reported a reduction in this parameter from 64.7 to 54.2 and from 9.8 to 7.2 mm, respectively. This reduction, in another study by Arazpour et al., 16 was confirmed on healthy subjects when using a SCO compared to locked KAFO (from 9.8 to 7.1 mm). The optimal level of this parameter was reported as being 4.7° for lateral displacement and 5° for vertical displacement. 16
Discussion
The aim of this study was to evaluate the effect of SCO use on walking efficacy in users of this type of orthosis. Recommended indications are different for SCKAFOs compared to KAFOs. Subjects with lower limb weakness can use a KAFO with drop locked knee joints. Users who have sufficient hip strength can benefit from a SCKAFO, and the criterion for using a SCKAFO is the presence of hip strength of at least Grade 3. Impaired cognition, knee-flexion contracture >10°, moderate to severe spasticity of the hamstrings, lack of hip abductors in bilateral patients, uncorrectable genu varum/valgum >10°, lack of motivation or inappropriate expectations, and body weight >300 lbs are all contraindications for using SCKAFOs. 25
The provision of reduced energy consumption has been quoted as one of the main aims and reasons for subjects with lower limb weakness to walk with a SCO. Due to paralysis of the lower limb muscles, KAFO users are forced to walk with the knee in a locked position, hip hiking strategy, leg circumduction, or a vaulting gait.6,7 This can cause soft tissue injury, an increased effort to walk, and a high rate of energy consumption in KAFO users.3,8 Only three studies evaluated this parameter in poliomyelitis subjects when wearing SCO compared to a locked KAFO.8,12,13 Despite the advantages of walking with a SCO, this type of orthosis has not demonstrated a significant improvement by producing decreased energy consumption.8,13 It would be expected that based on the free swing in the knee joint during swing phase made available by this device, the users effort would be decreased and therefore this would cause less energy consumption during ambulation. However, the number of participants was small, as few subjects participated in these studies, so the results cannot be generalized for the larger population. More studies are therefore needed to further analyze this effect.
Increased knee joint flexion and extension during swing when walking with a SCO compared to a KAFO in subjects with lower limb paralysis is a positive function for such individuals. In using SCO, walking with the knee locked provides stance phase stability, but provides free flexion in swing phase during ambulation, and the development of the SCO was based on this concept. The knee joint must have approximately 70° of flexion available in normal walking, but SCOs have not demonstrated that they can provide this amount of flexion. Future designs of SCOs must consider this limitation by providing more knee joint flexion. In addition, stance phase flexion must be developed in new designs of SCO to provide flexion during loading response and late stance. This is because flexion of the knee joint in stance phase plays a shock-absorbing role and smoothes the COM trajectory during normal walking. SCOs therefore also need to provide a near-normal walking pattern for subjects with less lower limb muscle strength than healthy subjects. Using a powered SCO may provide this, but the slow walking speed provided by these orthoses needs to be improved,16,17 and therefore, more research is needed in this field to provide more advanced powered SCO designs.
Using SCOs has been shown to provide improvement in frontal plane pelvic motions. Pelvic obliquity and vertical and lateral displacement have all improved with less abnormal gait deviations being noted (such as circumduction, hip hiking, and vaulting gait) during walking, but the number of participants in these studies has been low. Improvements in hip and pelvic motions were small and did not occur consistently among all studies, making it difficult to generalize this point of using SCOs compared to a locked KAFO. Future longitudinal studies involving more subjects and with longer training times with this type of orthosis may demonstrate whether the SCOs improve hip and pelvic kinematics.
The mean speed of walking when using SCOs has demonstrated lower walking speeds compared to a locked KAFO. Gait training with SCOs is also needed to produce a successful outcome in improving temporal spatial and kinematics during walking in KAFO users. Using a SCO needs a small knee extension moment to disengage knee joint locking in late stance. Experience of users during walking with the SCOs must be increased over time to provide more ability in controlling the orthosis. The concentration required for SCKAFO control may be the cause of the shorter stride lengths demonstrated, associated with longer stride times, and therefore slower walking speeds compared to walking with a locked KAFO. Another reason why SCO use does not improve walking speed is that studies have compared experienced KAFOs users with subjects who only had a short time to acclimatize to walking with the SCOs. Consequently, gait training with SCOs should be performed for several days or weeks to become experienced in walking to increase ability and confidence of users to control the SCOs and improve gait function before being compared to other devices.
Production of SCKAFOs started in the early 1970s, and since then there have been continuous improvements and modifications in their design, including the use of hydraulic 24 friction, 26 elastic 27 or impingement28,29 clutches,30,31 and brake mechanisms 23 to provide the stance control concept. In commercially available SCKAFOs such as the E-Knee from Becker Orthopedics, the Horton stance control knee joint, and the Sensor Walk from Otto Bock, weight-activated control is used. In the E-MAG Active from Otto Bock and SPL, the control of knee joint is position sensor activated. The Free Walk, UTX, and Full Stride/Safety Stride are ankle activated. According to cost, size, weight, or poor functionality, some of these designs have not led to clinical and commercial production, and development was based on mechanical and electromechanical mechanisms. New technologies can, however, be used to improve function of SCKAFOs; for instance, the use of actuators and sensors in lower limb orthoses have introduced new capabilities for adaptive control in SCOs.22,32,33
The selected studies are not analyzed according to the PEDro scale. This point was the main limitation of this study. The studies’ flaws included lack of randomization procedures, lack of control group, no masking of examiners and patients, and also there was lack of similarity among groups. These more recent studies have not substantially improved the quality of the research. There is a continuing need for high-quality experimental studies in this area.
Future studies should therefore include the following:
A study includes meta-analyses to produce improved and more reliable conclusions according to speed, cadence, pelvic obliquity, and step length;
A comparison between the different types of SCKAFOs;
A comparison of SCOs and locked KAFOs in their effect on energy consumption and endurance of walking in KAFO users to add more clarification on the effect of this type of orthosis in the rehabilitation of walking;
The design and construction of more advanced SCOs to further improve structural characteristics of orthosis in KAFO users is recommended;
The design and construction of more advanced powered SCOs as future designs of orthosis for use in rehabilitation of walking in KAFO users;
An investigation into the effect of gait training with SCOs on walking parameters in future designs of studies;
An investigation into the effect of SCOs on COM displacement and stability in quiet standing;
Although cosmesis was not evaluated in using SCOs on KAFO users, consideration should be given to improve cosmesis of walking when KAFO users wear this type of orthoses;
The effect of SCOs on quality-of-life measures and social participation compared to KAFOs.
Conclusion
SCKAFOs have been shown to support the knee joint during stance phase and provide free knee movement during swing phase successfully in all the walking studies analyzed. 15 SCKAFO designs have provided improved gait kinematics for KAFO users. Using SCOs has been shown to provide improvement in pelvic obliquity and vertical and lateral displacement during walking. Despite the advantages of wearing a SCO, this type of orthosis has not demonstrated a significant improvement in producing decreased energy consumption.8,13 Lower walking speeds have been reported when using SCOs compared to a locked KAFO. Development of new design of SCO that provides more normal patterns of walking is required in this field. To improve walking, additional gait training and accommodation periods are needed before walking with SCOs by KAFO users.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors did not have any conflicts of interest with regard to the study presented in this article.
Funding
We thank the Iran National Science Foundation for financial support (grant number 92001422) for this research.