
Abstract
Children and adolescents with congenital limb deficiencies are visibly and physically different from their peers. They present limitations in activities, depending on the severity of deficiency. Therefore they are at risk for lower participation in social and leisure activities. This might negatively influence the perception on their quality of life. The aim of this narrative review is to describe participation and quality of life in children with congenital limb deficiencies. Participation and quality of life are relatively new concepts. Psychosocial functioning, being closely related to the concept of quality of life, is described as well. A comprehensive review of the literature was conducted on participation, quality of life and psychosocial functioning in children and adolescents with congenital limb deficiencies. The review involved a systematic search using multiple data sources. Fifteen cross-sectional studies were included in this review. The literature to date provides limited knowledge on how children and adolescents with congenital limb deficiencies participate and how they perceive their quality of life. The psychosocial functioning, although described as at risk, appears to be comparable to healthy peers. In conclusion, more research is needed on how children and adolescents with congenital limb deficiencies participate and how they perceive their quality of life. A broader perspective will not only help parents in making the right choices for their children, but can also have implications for health care providers, teachers and agencies funding rehabilitation services.
Keywords
Introduction
Limb deficiency disorders are heterogeneous, chronic physical conditions with a reported prevalence across different countries of 2–7 in 10.000 births. 1 Most limb deficiencies in children are congenital in origin; acquired limb deficiencies as a result of disease or physical trauma, are less ordinary. 2
Almost all children with lower limb deficiencies are fitted with prosthetic components to enhance their ability to participate in activities of daily living. The use of prosthetic devices in children with upper limb deficiencies is less evident, depending on the level of deficiency and functional gain. 3
Participation and Quality of Life (QoL) are two key concepts in paediatric research and can be considered essential outcomes in describing health status and effect of interventions. 4
Participation is defined by the World Health Organization as the nature and extent of a person' involvement in life situations. 5 For children and youth, involvement in life situations includes participation in recreational and leisure activities as well as school and work activities. 5 Regular participation in day-to-day activities is an important aspect of children' health, well-being, and development. 6 In general, children and adolescents with disabilities tend to be more restricted in participation than their peers. 7 The most important factors that influence participation are children' functional abilities, environment (e.g., attitudes of community members), family (e.g., parents interest in recreation and family support) and personal characteristics (e.g., gender and social competence). 8–10
QoL is an emerging concept in the psychological functioning of children with chronic disorders. QoL can refer to aspects of a person' well being (physical, psychological, social), as well as aspects of the environment and a person' standard of living. 11 Psychological well being, self-esteem, adjustment and happiness are constructs related to QoL. 12 Evidence from the literature suggests that adolescents with disabilities are at greater risk for psychosocial maladjustment than adolescents without disabilities. 13,14
The relationship between participation and QoL is currently not fully understood. From studies that focused on children with complex disabilities it is suggested that participation is associated with increased QoL and reduction of health and social problems. 8,9,15 In the children included in these studies physical limitations as well as cognitive impairments were present.
Children and adolescents with limb deficiencies have a visible abnormal appearance which might negatively influence their participation and QoL. To what extent they are involved in and enjoy life situations is unclear.
The main objective of this review is to study and describe the current knowledge on participation and QoL in children and adolescents with congenital limb deficiencies. Because participation and QoL are relatively new concepts, psychosocial functioning as an outcome was included, being closely related to the concept of QoL. 16
Methods
Studies that described participation, QoL and/or psychosocial functioning in children and adolescents with congenital limb deficiencies were considered eligible for this review of the literature.
Search strategy
A comprehensive search from 1980 to October 2009 for relevant studies was performed in medical and psychosocial databases: CINAHL, the Cochrane library, EMBASE, HaPi, PEDro, PsychINFO and MEDLINE. The literature search was limited to published studies, available in full text English articles. Mesh, thesaurus and text-based search terms included: Participation, quality of life, adolescents, children, limb deficiencies, perceived disabilities, well being, personal satisfaction, physical appearance, adjustment, self esteem, self perception, psychosocial outcome, family, sports and recreation.
Reference lists of studies included and reviews have been hand searched for relevant publications. The complete search and screening of titles and available abstracts was done by the first author (AM). Studies that met the inclusion criteria were summarized in terms of purpose, type and setting of study, study sample and outcome measures. Results of all studies on participation, QoL and psychosocial outcome were independently assessed by the first author. Two independent researchers (IvW, MK) examined the summary of all studies for definite inclusion and exclusion and checked the results. Disagreements were discussed until consensus was reached.
Selection criteria
Studies were included if they met the following inclusion criteria: (1) Children and adolescents with congenital limb deficiencies (age 0–19 years), 5 (2) outcome measures concerning participation, quality of life or psychosocial functioning, (3) publication between 1980 and October 2009. Exclusion criteria were studies that included children with limb deficiencies in combination with cognitive impairment and studies reporting on effects of specific interventions.
Results
Search results
A total of 87 possible relevant studies were selected from the search (Figure 1). After screening title and abstract, 64 articles did not match the inclusion criteria. Five reviews were found 13,14,17–19 One study 20 was excluded for not being published full text.
After screening seventeen full text studies, another two studies were excluded. Reasons for exclusion were: Population age above 20 years 21 and unclear study sample. 22 Reference tracking of eligible articles and present reviews 13,14,17–19 did not provide new studies for inclusion. The 15 included studies all were classified as cross-sectional descriptive studies and are summarized in Table I.
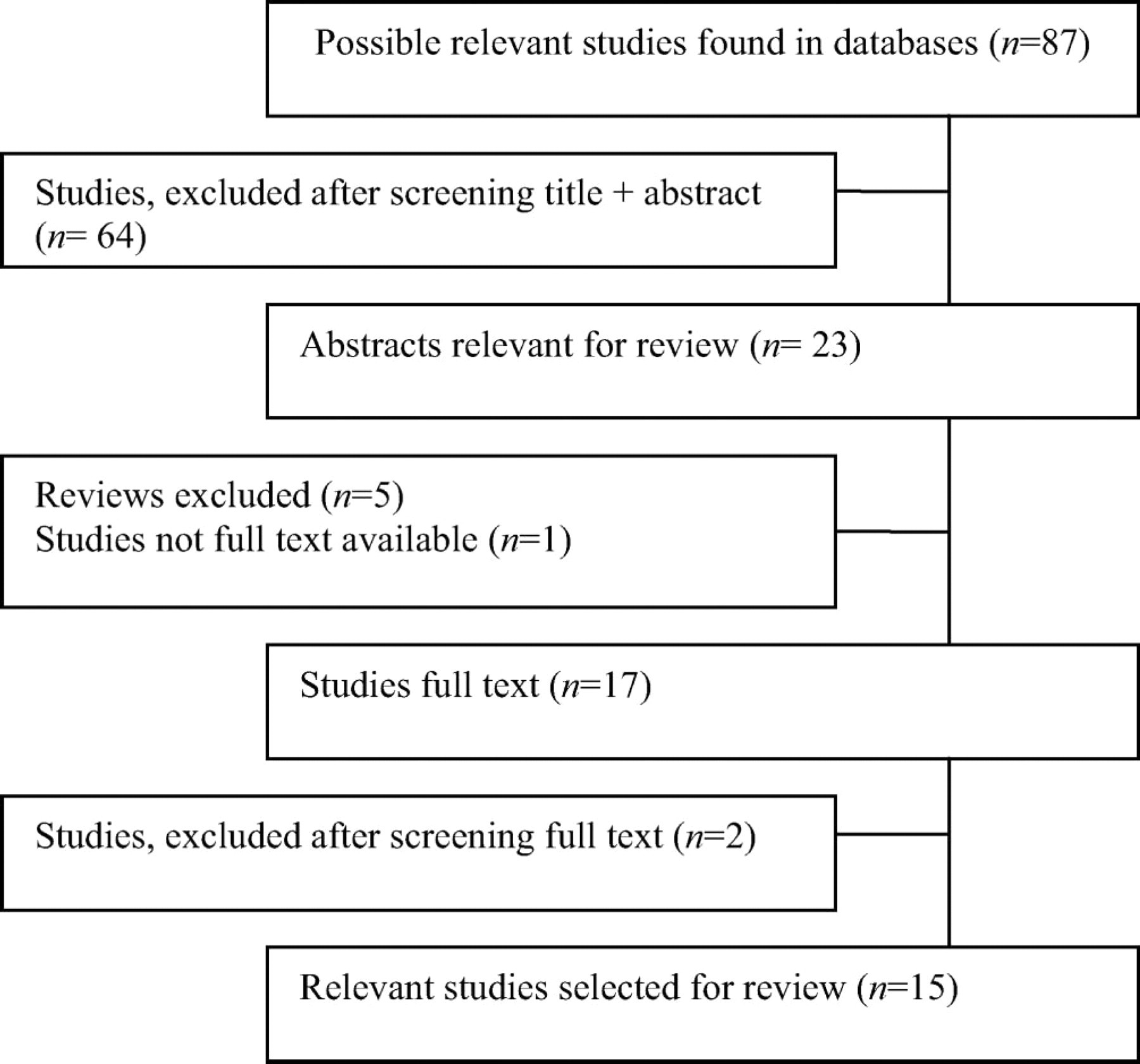
Flow chart of study selection.
Summary of studies.
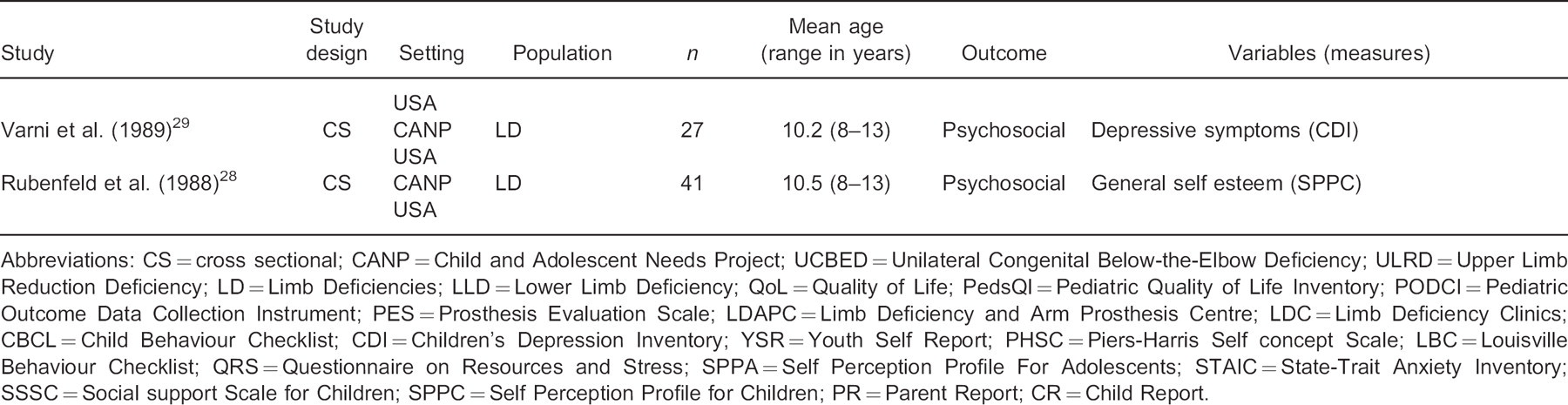
Abbreviations: CS=cross sectional; CANP=Child and Adolescent Needs Project; UCBED=Unilateral Congenital Below-the-Elbow Deficiency; ULRD=Upper Limb Reduction Deficiency; LD=Limb Deficiencies; LLD=Lower Limb Deficiency; QoL=Quality of Life; PedsQI=Pediatric Quality of Life Inventory; PODCI=Pediatric Outcome Data Collection Instrument; PES=Prosthesis Evaluation Scale; LDAPC=Limb Deficiency and Arm Prosthesis Centre; LDC=Limb Deficiency Clinics; CBCL=Child Behaviour Checklist; CDI=Children' Depression Inventory; YSR=Youth Self Report; PHSC=Piers-Harris Self concept Scale; LBC=Louisville Behaviour Checklist; QRS=Questionnaire on Resources and Stress; SPPA=Self Perception Profile For Adolescents; STAIC=State-Trait Anxiety Inventory; SSSC=Social support Scale for Children; SPPC=Self Perception Profile for Children; PR=Parent Report; CR=Child Report.
Evaluation of results
Participation
No studies specifically report on participation as outcome or used a standardized measure for participation. Aspects of participation are described in three studies. 23–25
James et al. 23 examined a large group of children and adolescents with Unilateral Congenital Below-the-Elbow Deficiency (UCBED), age range between two and 20 years. Parents and children above 11 years (n=184) reported on ‘sports/physical function’, ‘happiness’ and ‘global function’ as a part of a musculoskeletal health questionnaire addressing activity and participation components of function (PODCI). 26 No significant differences on these domains were found in children with UCBED compared with the general population and between prosthesis wearers and non wearers.
Herring et al. 24 and Vannah et al. 25 reported the frequency of recreational and sports activities in children with Lower Limb Deficiencies (LLD). In the study of Vannah et al., 25 more than half of the 258 children were participating in regular sports: Swimming 60%, indoor chores 59%, running 58%, outdoor chores 55%, bicycling 52%, basketball 42%. In Herring' study 24 43% of the children (n=21) were participating in competitive school athletics. Missing more than 10 days of school per year due to their limb deficiency was reported by Vannah et al. 25 in 7% of the children.
QoL
Assessment of health-related QoL was carried out using the Pediatric QoL Inventory (PedsQL) 27 in the study of James et al. 23 Children with UCBED were compared with the general population. Within the group of children with UCBED, prosthesis wearers were compared with non-wearers. Both parents and children (5–20 years) reported on the QoL of the child: No significant differences were found. When comparing children wearing a prosthesis with children not wearing a prosthesis also no significant differences were found, except for the QoL with regard to school functioning: significant higher QoL was reported for prosthesis wearers compared with non-wearers. Eleven to 20-year-old children with UCBED felt significantly happier than children in the general population, regardless of prosthetic use, as reported in the Happiness domain of the questionnaire addressing activity and participation (PODCI). 23
Psychosocial functioning
All, but two studies 23,25 focused on psychosocial adaptation in children and adolescents with Limb Deficiencies (LD). Eleven studies 28–38 were executed by Varni et al. within the Child and Adolescent Needs Project (CANP) in which they investigated psychological and social adjustment in order to identify risk and protective factors. The children (8–18 years) participating in the CANP project were diagnosed with deficiencies of upper and/or lower limbs of which the majority was congenital. Description of subgroups was not provided. Outcomes in the series of studies were perceived physical appearance, self-esteem, depressive symptoms, anxiety, perceived social support, behaviour and social competence.
From the CANP project it appeared that children with LD are not significantly different in how they perceive their physical appearance 34 and social support, 29,35 and in their self-esteem 31,34 compared with the general population. The children with LD are not more depressed 29,32 and they do not experience a greater number of hassles 29 than physically healthy peers.
On the other hand, in one study, Varni and Setoguchi 36 demonstrated greater behavioural and emotional problems and lower social competence in children with LD than the normative sample. Through parent report, 23% of the children in the above-mentioned study appeared to function in the clinically significant maladjustment range for behavioural and emotional problems; 14% of the children functioned in the clinically significant social maladjustment range. These percentages were compared to the proportion of maladjustment in the general population which is 10% for both behavioural and emotional problems and social competence.
This result could not be confirmed by the study of Hermansson et al., 39 in which parents and their children with ULRD who had initially been fitted with myoelectric prosthetic hands, reported on social competence, emotional or behavioural problems and depressive symptoms. No significant differences compared to normative samples were observed. All children though, irrespective of age or gender, had significant higher scores on the withdrawn behaviour subscale. Girls with ULRD (13–17 years) showed a tendency to lower social competence compared to girls in the normative sample.
Discussion
Although optimal participation and QoL are considered the main goals in paediatric rehabilitation, the literature provides limited knowledge on how children with congenital limb deficiencies participate and how their QoL is perceived. The psychosocial functioning in children and adolescents with LD appears reassuring but the studies are from earlier date and are products of especially one research group (CANP).
Participation
Participation has only been studied on different aspects like sports and going to school, but as a concept of overall functioning participation has not been measured in children with congenital LD. In one study, 23 participation was only partially questioned with the questionnaire PODCI 26 which addresses both activity (upper extremity physical function; mobility/transfers; pain/comfort) and participation (sports/physical function; happiness) aspects of function. The main purpose of the PODCI is to assess the efficacy of orthopaedic interventions. Currently, different instruments are available for measuring participation in children and adolescents with and without disabilities. 40 How appropriate those measures are in assessing participation in children and adolescents with LD needs to be studied.
More than 50% of the children and adolescents with LLD participate in sports activities. This is comparable to typically developing children and adolescents in the Dutch population: 62% of the children up to 15 years and 42% of adolescents between 15 and 25 years are participating in sports activities. 41 If and how children with LLD adapted their sports to their physical impairments and how they feel about that is valuable information which can not be found in literature. Further research is required on how children participate and how they can be encouraged to do sports and recreational activities. Due to advances in prosthetic technology and design, opportunities are available for children and adolescents with LD to be physically active in sports or recreation. 18,42,43
QoL
Remarkably, QoL is addressed in only one study, 25 reporting on children with an upper LD whose QoL is found to be similar to the general population. An adult study, 21 in which 10
patients with LLD from the study of Herring et al. 24 were evaluated on their physical and psychological functioning, showed no significant difference in QoL from the normative sample. It supported the idea that adults who have had an amputation of the forefoot in childhood perform as well as the average adult on measures related to QoL, self concept and psychological adjustment.
Research on how children and adolescents with LD perceive their QoL is important for understanding the perception of their disability. Over the last decade, research of QoL of children and adolescents with various conditions has advanced significantly. Many factors can have an influence on the individual' perception of their position in life. In Dutch adolescents, 12–19 years old with various chronic disabilities but no limb deficiencies, factors significantly related to QoL were degree of physical impairment, number of hospital visits, visibility of condition, experiences with visibility, body image, general health and self-efficacy. 44 Age was not related to QoL. 44 Girls rated their QoL lower than boys, which is confirmed in other studies. 45,46
Similar results were found in adults with amputation of the upper and lower extremities: factors related to their QoL were physical disability and pain, and men had higher QoL than women. 47 In this population, a young age at the time of amputation and an upper-limb amputation were associated with a better QoL.
In children and adolescents with limb deficiencies it is unclear how they perceive their QoL. Factors related to their QoL are unknown and therefore future research is needed.
Psychosocial functioning
Psychosocial functioning in children and adolescents with LD appears to be comparable with healthy peers. To get more insight in the psychological and social adjustment in children with LD, researchers of the CANP project examined different associations in order to identify risk and protective factors. Although not a primary focus of this review correlations of CANP' study outcomes were summarized (see appendix available online from www.informahealthcare.com/10.3109/03093646.2010.495371). Multiple perceived social support domains were found to be statistically significant predictors of psychological adjustment. Higher perceived social support was associated with lower depressive symptoms and higher self esteem. 35 In particular, classmate social support appeared to be highly predictive and was therefore represented as a risk factor for children with LD. 35
In children with ULRD more withdrawn behaviour was considered to be a possible result from societal attitudes towards visible physical differences. 39 How to deal with peer teasing and curiosity is a concern dealt with by parents of children with ULRD. 48 These findings indicate the importance of assessing social emotional functioning in children and adolescents with LD. It will help healthcare providers to identify potential needs and areas of support in the challenges children and adolescents with LD and their families face associated with the visible physical difference.
Methodological issues
All studies included in this review are descriptive and exploratory and have a cross sectional design. No causal effect can be drawn from cross sectional studies and therefore the level of evidence is limited. 49
Most studies have used well developed psychometric measurement tools with demonstrated validity and reliability. In two studies the measures used to describe physical 24,25 and psychological functioning 24 were poorly described, lacking psychometric
information and references. Except for the previously mentioned two studies, all measurements allowed comparison with population norms to control for the non-specific effects of limb deficiency.
Although the population in all studies have been described as limb deficient children and adolescents, direct comparison between the studies is difficult due to age range (2–20 years) and lack of knowledge on heterogeneity of diagnoses. While some studies 23–25,39 investigated a subgroup within the diagnosis limb deficiency, the CANP project included limb deficient children without proper description of the variety within the population. It is plausible that differences in outcome in upper and lower deficiencies or combinations of both exist. Hand function is essential in most hobbies and a deficiency of the upper limb is more visible to others than a lower LD. On the other hand, a lower LD may possibly lead to other participation or adjustment problems.
Although in the CANP studies a small number of children had acquired limb deficiency, a comparison of congenital versus acquired limb loss differences on adjustment measures is mentioned in only two studies 32,38 and proper analysis is lacking. Also gender or age subgroups were not explored due to small sample sizes.
No details are presented on interventions children received. As stated before, children with limb deficiencies present a heterogeneous condition with a variety of interventions and treatment options. The kind of treatment may influence the relationship between psychosocial factors and participation and overall QoL.
Conclusion
This review reveals a lack of knowledge on how children with congenital limb deficiencies participate and how their QoL is perceived. Their psychosocial functioning, although described as at risk, appears to be comparable to healthy peers.
Participation and QoL are relatively new concepts in rehabilitation medicine and can be considered as key outcomes. Nowadays different measurement tools are available to measure both concepts. Children and adolescents with congenital LD are a considerable diagnosis group in rehabilitation medicine and therefore further studies are required to describe how they participate and how they perceive their QoL. This is important to guide the development of interventions to promote optimal participation and QoL in this population. Furthermore, identification of factors that influence participation and the relationship with QoL in children and youth with limb deficiencies needs to be explored.
Acknowledgements
The authors would like to thank M. van Brussel, PhD, C. van der Sluis, MD PhD, and O. Verschuren, PT PhD, for their support in the preparation of this manuscript.