
Abstract
Purpose
The primary aim was to examine if there were differences in physical function and health-related quality of life (HRQoL) between young adults (18 to 35 years) with unilateral congenital lower-limb deficiency (CLLD) who had been surgically lengthened (Surg) and those using lengthening prostheses (Pros). Second, we wanted to compare their health status with an age- and gender-matched reference group (Ref) without CLLD.
Methods
Cross-sectional study including a study-specific questionnaire, clinical examination, two field tests evaluating physical function (the six-minute walk test and the Stair test) and HRQoL questionnaires (Short Form (SF)-36 and EuroQol (EQ)-5D-3L).
Results
Physical function and HRQoL did not differ between the two treatment groups. The odds for having painful or disfiguring scars were 18 times higher in the Surg group (n = 16) compared with the Pros group (n = 14). The CLLD group showed significantly reduced physical function compared with the Ref group. HRQoL, measured by the EQ-5D-3L visual rating scale, was significantly reduced in the CLLD group compared with the Ref group, as was the SF-36 physical function domain in both genders. Men with CLLD also showed increased bodily pain and reduced general health (SF-36), while we found a reduction in the emotional role domain in women compared with Ref.
Conclusion
There were no significant differences in physical function and quality of life in young adults with CLLD treated with surgical lengthening compared with those using lengthening prostheses. Compared with the general Norwegian population, young adults with CLLD had significantly lower physical function and reduced HRQoL in some domains.
Keywords
Introduction
The long-term goal when treating children born with congenital lower-limb deficiencies (CLLD), e.g. congenital fibular deficiency (CFD), is to achieve an active adult lifestyle with optimal function and as little musculoskeletal pain and complaints, including cosmetic aspects, as possible. 1 For the orthopaedic surgeon, this traditionally implies achieving approximately normal alignment with equal limb length and a normal gait pattern based on full weight-bearing. 2 Most often the goals are achieved surgically by one of two treatment modalities: foot preservation and limb salvage with lengthening procedures; or fitting of prostheses, with or without amputation. Colleagues will differ actively in the literature and at conferences on what is ‘best’. A limited number of previously published studies have compared the outcome of the two methods in patients with CFD.3–6 In a multi-centre study, Walker et al 5 followed the patients until adulthood (mean age 32.6 years), while other studies mainly reported outcomes in children. McCarthy et al 4 reported that children with CFD who underwent amputations (age about ten years) had no activity limitations, while the lengthening group showed moderate activity limitations (age range 16 to 18 years). In contrast, Walker et al 5 found that both groups were functioning at high levels. These evaluations were, however, reported based on questionnaires only, without any clinical examination of physical function. Quality of life aspects were only reported by Walker et al, 5 who found that except from the scores concerning job satisfaction, where the amputees scored better than the surgically lengthened patients, there were no significant differences between the groups.
At Oslo University Hospital, the first limb-lengthening procedure was done in 1977 with the Wagner device. However, developing this treatment modality to become a regular part of the surgical practice took another ten to 15 years. This seems to have been the case in most of the world, since studies in adults comparing lengthening surgery with permanent fitting of prostheses in patients with CLLD are still lacking in the literature. The first patients treated with callotasis surgery in our institution have now reached young adulthood and it is of interest to know how they are doing in this phase of life, compared with peers who have been treated in the traditional way, as well as compared with the general Norwegian population.
The primary aim of the present study was to evaluate whether there were any differences in physical function and health-related quality of life (HRQoL) between young adults born with unilateral CLLD who had been surgically lengthened and those walking with lengthening prostheses. The second aim was to compare their HRQoL status and physical functioning with an age- and gender-matched reference group without CLLD.
Methods
Participants were recruited after reviewing records from all patients aged 18 to 35 years registered with a diagnostic code of 755.3/755.4 in accordance with congenital reduction deformities of lower limb/unspecified limb, or with Q72.x corresponding to congenital reduction defects of lower limb in the World Health Organization International Classification of Diseases ICD-9 or ICD-10, respectively. 7 Participants were patients with functioning knee and hip joints who had been treated for unilateral deficiencies. Functioning hip joint for those with femoral deficiencies was defined as Aitken score A. 8 Of the 175 patients who had at least once been coded according to the criteria, the majority had been given this diagnosis code incorrectly and proved to have other conditions; therefore, only 39 could be included. Of these, 34 patients (13 female, 21 male) agreed to participate in the present cross-sectional study. The Regional Committee for Medical and Health Research Ethics South East approved the study. Written informed consent was obtained from the participating patients.
Demographics and clinical status
The data registered following a study-specific form (the form, in Norwegian, is available by contacting the first author) during the clinical consultation by one of two orthopaedic surgeons (TSK and HS) included: birthdate; gender; weight and height; level of education; relationship status; exact diagnoses; number and type of operations; type of lengthening device; level of amputation; age at operation; leg length discrepancy before first lengthening and at consultation; use of shoe lifts; complications to surgery; pain in lower limb, upper limb or back; current use of walking aids or wheelchair; and ankle, knee and hip mobility (full range of movement or not).
Classification
Congenital longitudinal deficiencies were classified according to those systems being most actively in use at the time of diagnosis: the Achterman and Kalamchi classification for fibular deficiency, 9 the Aitken classification for femoral deficiency 8 and the Jones classification for tibial deficiency. 10
Physical function
The six-minute walk test (6MWT) is a simple and inexpensive test used as a predictor of aerobic capacity.11,12 Participants were instructed to walk as fast as possible (without running) back and forth between two cones 15 m apart on an even, hard surface for six minutes. The results were measured in metres.
The Stair test is described as a sub-maximal cardiopulmonary exercise test. 11 The participants were instructed to ascend and descend 20 average-sized steps three consecutive times and had to use all steps. They were allowed to run and, for safety reasons, they were also allowed to use the banister if needed. The results were measured in seconds.
Results from both physical function tests were compared with a sample of age- and gender-matched Norwegian men and women without any lower-limb deficiencies. 11
HRQoL
Self-reported HRQoL was evaluated using the Short Form-36 survey (SF-36) 13 and the EuroQoL (EQ-5D-3L). 14 The SF-36 has been recommended as a method for evaluation of patient-reported outcome measures (PROMs) in lower-limb reconstruction surgery 15 and includes eight domains: physical functioning; role limitations physical; role limitations emotional; bodily pain; social functioning; mental health; vitality; and general health perception. 13 The five dimensions included in the EQ-5D-3L are: mobility; self-care; usual activities; pain/discomfort; and anxiety/depression. The questionnaire provides a simple descriptive rating scale registering general health as a vertical calibrated visual analogue scale (VAS) with marks from 0 (worst health) to 100 (best health) and a single index value for health status.14,16 Two aspects in the study-specific questionnaire were also related to quality of life: whether operative scars were painful, disfiguring or no problem; and to what extent the deficiency influenced self-image on a scale from 0 to 10 (0 means no influence and 10 total influence).
Statistical analysis
Demographic variables are presented by median (range) values or frequency and percentage. Differences between the lengthening and prostheses groups were analysed using the Mann-Whitney U test or chi-square test. Odds ratio was used to calculate the odds of reporting painful and/or disfiguring scars in the two groups.
The Stair test in the reference material 12 was performed by ascending and descending 18 average-sized steps three consecutive times, and the results of the reference material was recalculated to conform with the 20 steps used in the present study.
Norwegian normative values for the SF-36 13 were compared with the CLLD group. As these values are presented separately for the age groups ≤ 29 years and 30 to 39 years, mean values for the two groups were calculated and compared with the CLLD group using the one-sample Wilcoxon signed-rank test. A one-sample t-test was used to compare the scoring of general health (EQ-5D-3L) of the CLLD group with normative samples from Sweden 16 and Poland. 17 Values of p < 0.05 were considered statistically significant.
Results
Among the five included who did not want to participate, one had gone through lengthening procedures and felt generally negative about visiting the hospital, while the four remaining were prostheses-users who reported few problems in life. Two lived overseas and two were too busy with their work. The remaining 34 patients were evaluated and four of these were excluded after the examination: two with femoral deficiency had non-functioning hip joints according to the chosen cutoff of Aitken A 8 and two had bilateral CFD. The remaining 30 patients were included in the analysis.
The surgical lengthening group
The 16 participants in this group had undergone a lengthening procedure with external fixators (Surg). Of these, ten had CFD with an average of 4.1 (3 to 5) foot rays. The first lengthenings were done with mono-lateral fixators, the more recent with ring fixators (Table 1). The median limb length discrepancy (LLD) at first lengthening was 6 cm (4.5 to 15), while the discrepancy at follow-up was 1 cm (0 to 15). Eight were lengthened once, four twice and four three times. All but two, with a single lengthening procedure of 4.5 cm and 5 cm, respectively, needed additional surgery; from soft-tissue lengthenings via osteotomies to open reduction of dislocated hips (two) or knees (three). One had a persistent dislocation of the hip after one Orthofix-lengthening (Verona, Italy) of the femur at age five years, despite five subsequent operative procedures to relocate and stabilise the hip. Two with LLD of 2 cm and 5 cm, respectively, used shoe lifts at follow-up. Two walked with crutches, one due to the dislocated hip, the second for more diffuse reasons. As a group, they subjectively were content with the choice of treatment mode their parents had made on their behalf and were happy to still walk on their own feet, whatever size and form.
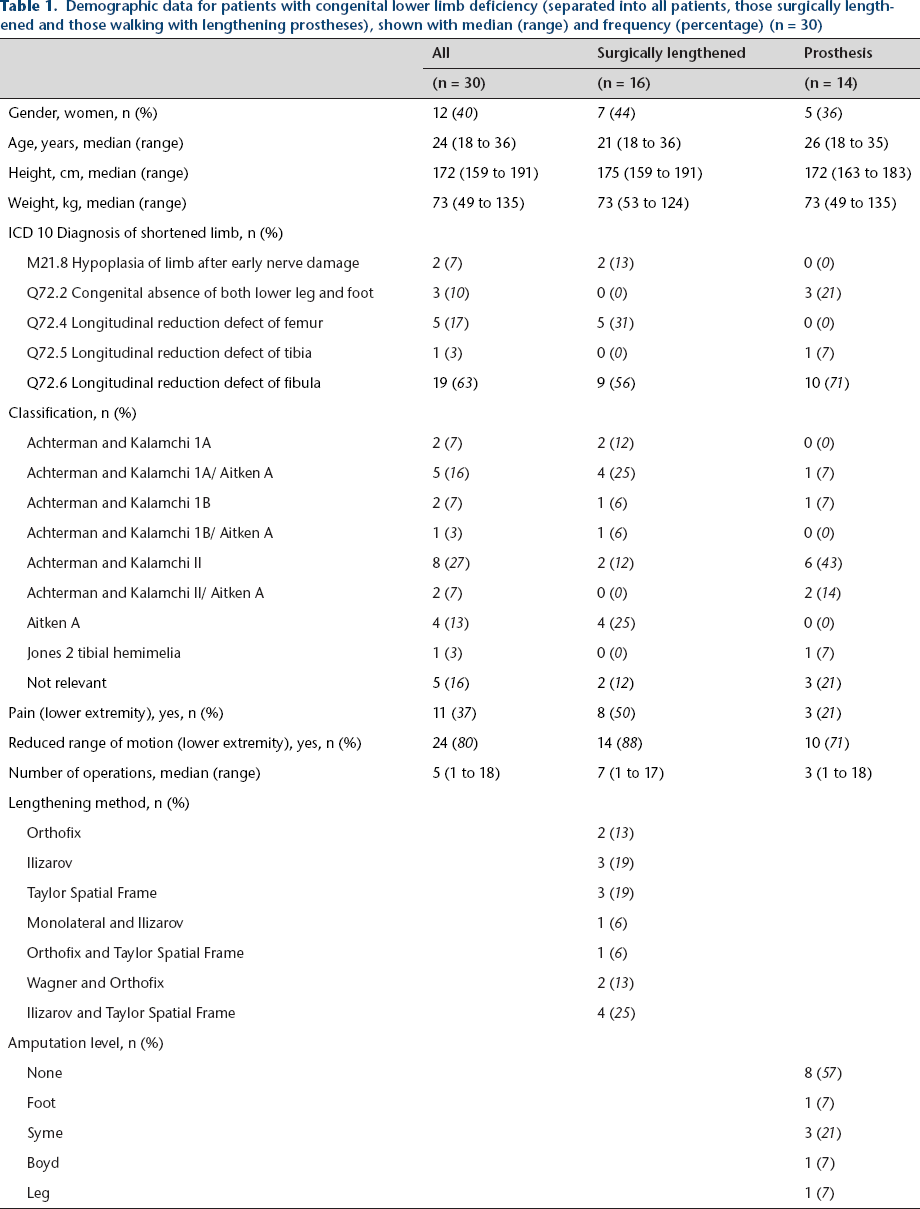
Demographic data for patients with congenital lower limb deficiency (separated into all patients, those surgically lengthened and those walking with lengthening prostheses), shown with median (range) and frequency (percentage) (n = 30)
The lengthening prostheses group
Of the 14 participants in the prostheses group (Pros), ten were born with CFD with an average of 3.1 foot rays (1 to 4). One patient had undergone lengthening procedures before amputation. Of the 14 participants, six had amputations, at an average age of 12 years (10 to 16) (Table 1). Three of these were originally planned for lengthening surgery, but the patients themselves decided they would rather go for permanent fitting of prostheses. Four had a Syme amputation, one a Boyd and one several amputations at foot level. One Syme-amputated participant had a through-leg re-amputation at age 27 years. The other amputated participants had no subsequent need for surgery. Seven used extension prostheses with intact deficient limbs and all had needed surgery for alignment or, for the two with trans-tibial congenital amputations, had needed many revisions due to tibial overgrowth. The last in the group had settled for a shoe lift of 8 cm with a LLD of 12 cm and a persistent equinus in the CFD limb. One used crutches at the follow-up due to a recent incident, but did not usually need them. As a group, they were subjectively content with the choice of treatment mode made by their parents and, for those who had amputations, themselves. Not one missed the amputated foot and some commented they wished their parents had decided on the operation already while they were babies. Others were just happy they had not needed to go through the lengthening procedures.
There were no differences between the treatment groups in demographic variables, in pain, in number of operations, nor in range of movement in the lower limbs (Table 1).
Physical function
Both treatment groups showed a wide range in performance in the physical function tests and there were no differences between the two groups (Table 2).
Functional tests shown with median (range) for patients with CLLD (divided into those surgically lengthened and those walking with lengthening prostheses) (n = 30)

Comparing our patients with CLLD with the reference material, 11 there were significant differences in both the 6MWT (558 m (405 to 787) versus 682 m (501 to 888); p < 0.001) (Fig. 1) and the Stair test (46.5 seconds (28.8 to 104.3) versus 34.8 seconds (26.3 to 50.7); p < 0.001) (Fig. 2).
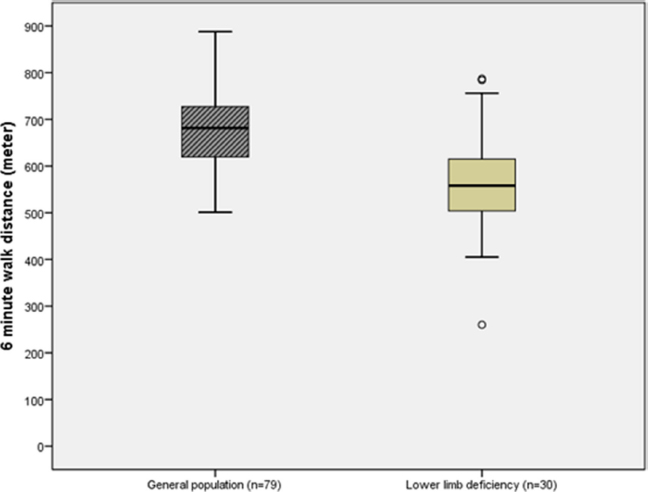
Difference in the six minute walking distance (given in metres) between a sample derived from the general population (Reference material) 12 and patients with congenital lower-limb deficiency.
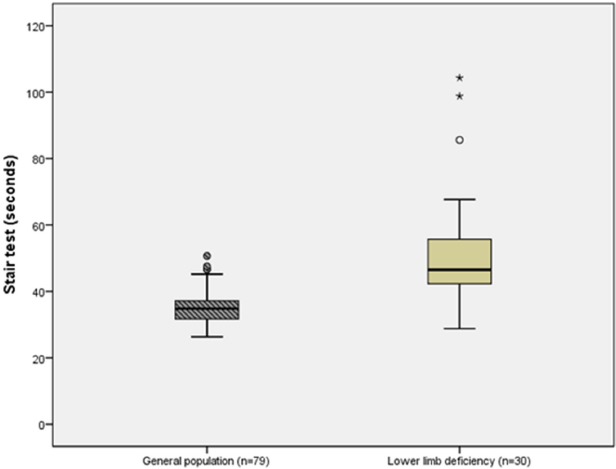
Difference between a sample derived from the general population (Reference material) 12 and patients with congenital lower limb deficiency in the Stair test (measured in seconds).
HRQoL
Self-image did not differ between treatment modalities (Table 3). However, 12 patients in the Surg group reported painful and/or disfiguring post-operative scars, compared with two patients in the Pros group, making the odds for having pain and/or disfiguring scars 18 times higher when comparing the Surg and Pros groups (95% confidence interval (CI) 3 to 117). Several patients, especially girls, reported during the examination that they had been offered scar revisions by plastic surgeons.
Health-related quality of life measures shown with median (range) or frequency (%) for patients with congenital lower limb deficiencies (divided into those surgically lengthened and those walking with lengthening prostheses) (n = 30)
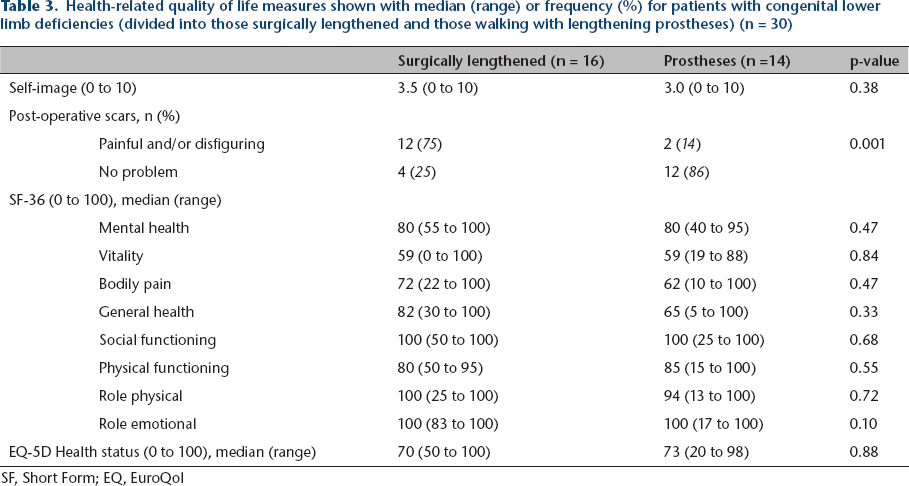
SF, Short Form; EQ, EuroQol
There were no differences between the Surg and Pros groups in any of the aspects in the SF-36 or the health status scale derived from the EQ-5D.
When comparing the HRQoL measured by SF-36, the limb-deficient men showed reduced physical functioning (p = 0.002), increased bodily pain (p = 0.011) and reduced general health (p = 0.017) compared with the Ref group. The 12 limb-deficient women showed reduced physical functioning (p = 0.040) and a reduction in emotional role compared with the Ref group (p = 0.004). 13
Self-assessed general health measured by EQ-5D-3L (VAS scale) showed an average of 74 (standard deviation 19) in the CLLD group, which gave a difference of -15 (95% CI -22 to -8) when compared with an average of 89 from a Swedish general population (p < 0.001) 16 and a difference of -11 (95% CI -18 to -4) when compared with an average of 85 from a general population in Poland (p = 0.003). 17
Discussion
In young adults with unilateral CLLD, there were no differences between the surgically lengthened and the prostheses group in physical function and HRQoL. The only difference found between the treatment groups was in painful and/or disfiguring scars, where the Surg group had significantly more pain and discomfort from post-operative scars in the lower limbs than patients in the Pros group. Compared with reference materials, our patient groups on average showed reduced levels of physical function 11 and scored significantly lower on the EQ-5D-VAS-scale of self-assessed general health,16,17 as well as in some items from the SF-36. 14 However, there was a wide range in performance in both treatment groups, underlining our observations of heterogeneity during the study period - that there were individuals in both groups with a very high level of both mental and physical function, as well as individuals with significantly reduced levels of function.
The limitations in this study are obvious, since the distribution of diagnoses and deficiencies in the two patient groups differ (Table 1), suggesting they are not fully comparable. Two patients in the Surg group did not have genuine congenital deficiencies, but had acquired an early general hypoplasia of one limb after disease during infancy. In Norway, children who acquire limb deficiencies after amputation or other causes before their second birthday, for practical purposes, are considered and treated by multidisciplinary teams along with those with congenital deficiencies. For this reason, these two patients were included in our study. Along with a third patient in the Surg group with general hypoplasia of one limb, these had normal foot and ankle anatomy. At the other end of the range of deficiencies were the three patients born without a foot at all, where the treatment mode was given. Thus, the two groups were skewed to begin with.
Patients with lower-limb deficiency, in general, constitute a heterogeneous group, both regarding different diagnoses and the extent and severity of the deficiency within the same diagnosis. The most comparable patients with regard to diagnosis included in the present study were the CFD patients (n = 19). However, they also were not quite comparable, since all feet in the deficient limbs of the Surg group had three to five rays at birth, as opposed to one to four rays in the Pros group. Due to this tendency of fewer deficient feet in the Surg group, it could be argued that this group would be expected to perform better than the Pros group, an issue also discussed in the study of patients with CFD by Walker et al. 5
Nonetheless, we decided not to divide the participants into smaller diagnostic groups, but go on with analysis for comparison with the groups as they were, in the hope of at least illuminating some trends related to one treatment modality versus the other. The number of patients included in this study was small and the dispersion in results is wide. However, as our hospital has national responsibility for treatment of patients with CLLD, we can assume that, with the exception of those few unwilling to participate, the patients included in this study are representative of young adults being treated for CLLD in the first era of reconstructive lengthening treatment in Norway. To date, corresponding studies have not been published that we are aware of, since the study of adult outcomes following amputation or lengthening for CFD by Walker et al, 5 although also dealing with physical function and quality of life issues, was done using questionnaires, without physically seeing the patients at clinical follow-ups.
Physical functioning contributes heavily to an optimal HRQoL. In the present study, we therefore wanted to include some objective tests to evaluate the patients’ functional capacity and not only base the results on PROMs. Both the 6MWT and the Stair test are simple, clinical field tests frequently used to evaluate functional and cardiorespiratory capacity,11,12 and reference values derived from healthy persons exist. 11
There were no differences between the two treatment groups for either the 6MWT or the Stair test (Table 2), indicating that functional capacity was almost the same, irrespective of treatment mode. However, as shown in Figures 1 and 2, the patients with CLLD showed a lower performance in both tests compared with the Ref group. 11 The difference between the Surg and Ref groups was more pronounced for the Stair test than the 6MWT, with a difference of 26% compared with 19%, indicating that the Stair test is an even more demanding task to perform with lower-limb deficiencies, not only being due to general lower aerobic capacity.
The SF-36 includes two items related to physical function: the ‘Physical functioning’ and ‘Role physical’ items. For both the Surg and Pros groups, there was a significant reduction in self-reported physical function compared with the Ref group, 13 which indicates that there was good agreement between physical function reported by PROMs and the clinical field tests. This expected reduction in physical function has been poorly reported in patients with CLLD, although it was clear in a long-term follow-up of a small group of patients treated with van Ness rotationplasty for proximal femoral deficiency. 18 Studies done in children have rather tended to find normal physical performance in this patient group, as in a Dutch study, 19 which included children and adolescents with CLLD, where the participation in activities and perceived HRQoL did not differ from those among typically developing children. However, the participation of adolescents (aged 12 to 18 years) with lower-limb deficiencies was characterised by less diversity and with less interaction in social and skill-based activities, 20 suggesting there is an increasing difference in physical activity level in CLLD patients compared with the general population, with age.
There were no differences between the Surg and Pros groups in any of the items in the SF-36. There were, however, significant differences in some items, beyond those related to physical function, for the CLLD patients compared with the material from the Ref group. The reference values are presented by age groups and gender, and when comparing them with the men and women included in the present study, we found some significant gender differences. Both genders showed reduced physical functioning; however, increased ‘Bodily pain’ and reduced ‘General health’ were only present among the male participants, while the female participants showed reduced ‘Role emotional’ compared with the general population. 13 These gender differences in quality of life factors have previously not been reported in CLLD patients. Walker et al 5 found no differences between treatment groups with CFD in the SF-36, and their mean score was within one standard deviation of the normal population, suggesting they had a quality of life ranging from slightly below to slightly above average. They did not report any differences in results between genders.
While more studies on function and quality of life in adults comparing treatment modules for CLLD are needed, there are some studies evaluating these aspects in adults having been through one treatment or the other. In a long-term follow-up including patients who had undergone Ilizarov lower-limb lengthening during childhood (37 patients aged 17 to 30 years, where 22 had congenital deficiencies), Moraal et al 21 found that they still had physical restraints. Compared with the normal population, the lengthened group also had more pain, reduced gross motor function and reduced vitality when testing HRQoL with the TNO-AZL Adult Quality of Life questionnaire, 21 which fits with our findings. 22 In the classic papers of Herring and Birch reviewing treatment with Syme amputation, the first included 21 children, 23 while the second paper followed up ten of the 12 CFD patients from the first study who were older than 18 years at the time of review. 24 The mean age of the ten patients at the time of the Syme amputation was seven years (2 to 12), 24 while the amputated in the current study on average were aged 12 years (10 to 16). The higher age at our institution might relate to a reluctance to do ‘no return’ surgery of this kind before the child was old enough to participate in the decision, not least since the reconstructive treatment modalities were developing in a way supporting a ‘wait and see’ attitude of the surgeons involved.
Tests of quality of life and self-esteem did not show any significant difference from the reference population in the study of Birch et al. 24 The study also included physical performance testing by measuring isokinetic knee extension and flexion muscle strength.23,24 They compared the CFD limb with the normal contralateral side in the follow-up study of patients older than 18 years, and found quadriceps power to be an average of 61% and the hamstrings power mean 71% in the affected limb. 24 In the young adults of the current study, physical function rather than muscle power was evaluated, and relevant studies in similar patients are lacking. However, walking speeds in 6MWT have been studied in individuals with lower-limb amputations and a correlation with oxygen cost was found. 25 Distances walked during the test were not given, as the focus was on walking speed. In the current study, the average distance walked was significantly reduced compared with the values in the Ref material, 11 but the range of performance was wide in both the Surg and Pros groups and not so different from that found in 167 patients with musculoskeletal conditions receiving physiotherapy in primary care. 26 The average age of the latter group was 55 (all aged more than 18 years), while the current study participant was aged 24 years on average, indicating a mean physical performance at the level of middle-aged persons with need of physiotherapy, mostly in the lower extremities. 26 The CLLD group on average walked 83% of the distance that the reference population did in six minutes, or equally as far as the average 60- to 70-year-old. The physical performance in the Stair test also showed a very large range of performance in this study and much more so than in the general population. The best performing in the CLLD group were almost as fast as the best performing in the general population of same age. On average, however, the patients needed 57% more time to do the Stair test than those in the Ref group. 11
Painful and disfiguring post-operative scars are well known sequelae after lower-limb lengthening with external fixators, although very little documentation exists on this specific problem. 27 However, Moraal et al, 21 in their follow-up of young adults having been through Ilizarov lengthening in childhood, did include the scar aspect in their review by evaluating results of plastic surgery by means of a rating for the total result on a ten-point scale (the higher the rating, the higher the satisfaction). In total, 11 out of 37 patients had been to a plastic surgeon for surgical removal of scars: seven wanted plastic surgery, while 19 were not interested. In the present study, the topic was addressed when going through the study-specific form with the patients, and problematic scars were far more present in the Surg group than in the Pros group. We did not specifically study the scars or evaluate them on a scale or with a scoring system,27,28 but several patients spontaneously mentioned that they had been referred to a plastic surgeon because of troublesome or cosmetically disfiguring scars. With modern intramedullary lengthening techniques the scar problems are expected to be reduced, but scars in the legs in particular have been found to reduce patient satisfaction. 27 For small children, the use of ring fixators will still be a main method for surgical lengthening of the tibia. The parents should be informed about this consequence of the treatment mode along with the many other known complications of lengthening surgery with external fixators.
One observation was that most patients were content with whatever treatment mode they had ended up with, although some amputated participants wished the surgery had been done when they were a baby. This leads us to conclude that in cases where it is not obvious whether to lengthen surgically or go for permanent fitting of prostheses, the orthopaedic surgeon and the multidisciplinary team, through the first year of the child's life, should help the family find out what mode fits their culture and their baby. Also, if that choice is the fitting of prostheses as a permanent solution, a final amputation should already be done at around the age when the child starts walking. 5
There were no significant differences in physical function or HRQoL between the surgically lengthened patients and those with prostheses. Since the groups differed in deficiency profile, it was not possible to conclude if one treatment mode was preferable over the other, except for post-operative scars, where the Pros group had far fewer problems than the Surg group. Both groups on average scored significantly lower than the normal population with regard to walking distances, speed at stair climbing and some quality of life domains, but the wide dispersion between the patients indicates that while some experience the lower-limb deficiencies influencing their daily life on a permanent basis, others are functioning as healthy, normal individuals.
Footnotes
Sophies Minde Ortopaedics Ltd. provided funding for this study.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.