
Abstract
Finger and partial finger amputations are some of the most frequently encountered forms of partial hand loss. A high quality aesthetic prosthesis with passive function can be helpful to the patient since loss or congenital absence or malformation have both a social and psychological impact on the patient. Prosthetics is an art and science which provides a lifelike appearance to the lost structures of the patient. This case report presents the fabrication of a silicone finger prosthesis which had good suspension, adequate function, was comfortable to use and aesthetically acceptable to the patient.
Introduction
Finger and partial finger amputations are some of the most frequently encountered forms of partial hand loss. The most common causes of these amputations are trauma, congenital absence and malformations. 1 In India, a developing country where farming is the main occupation, most of the partial traumatic finger amputations are seen in the harvesting season. Primitive agricultural machines such as kutty and the thresher machine take a heavy toll on hands of young men and women every year. 2 Any deformity, especially with the hands which are constantly in the view of the patient and others, may adversely affect a patient' socio-economic status. 3 Advances in surgical sciences in the form of micro vascular reimplantations have helped save many severely injured and traumatically amputed digits. However, in most of the patients, micro vascular reconstruction is contraindicated, unavailable or unsuccessful. It is in this group of patients that a prosthesis can be provided and may offer great help as, besides psychosocial issues, 1 patients also face pain, contractures, reduced grip strength and hypersensitivity. 4
The fabrication of a prosthesis is as much an art as it is a science. Prosthesis form, coloration and texture must be as indiscernible as possible from the surrounding natural tissues. The ideally constructed prosthesis must duplicate the missing parts so precisely
that the casual observer notices nothing that would draw attention to the prosthetic reconstruction. Rehabilitation efforts can only be successful when the patient can appear in public without fear of attracting unwanted attention. 5 The construction of a prosthesis consists of six stages and each requires extraordinary attention to detail: (i) Impression and working cast, (ii) sculpturing and formation of the pattern, (iii) mould fabrication, (iv) stump fabrication, (v) processing of the prosthesis material with intrinsic and extrinsic coloration, 5 and (vi) proper suspension testing of the prosthesis. This paper presents the prosthetic rehabilitation of amputated fingers with a custom-made prosthesis fabricated using silicone elastomers, which had adequate suspension, function, is comfortable to use and aesthetically acceptable to the patient.
Case report
A 32-year-old male patient reported to the Department of Prosthodontics, Rural Dental College, Loni, Maharashtra, India, for the fabrication of finger prostheses. On general examination it was noticed that the patient had lost part of his index, middle finger and thumb of the dominant right arm due to trauma in a thresher machine. Amputations were carried out through the distal portion of the middle inter phalanx of the middle finger and by disarticulation through the proximal inter phalangeal joint of the index finger and the thumb. The amputated fingers showed thickened ends. The surrounding area appeared to be normal with no signs of any infection over the digits.
After taking an informed consent from the patient, to ensure his willingness and cooperation, the case was taken up for reconstruction of partially missing fingers of the right hand. The hospital occupational therapist was involved in the assessment and management of the amputee. As the patient concerned was self-motivated, the role of the psychologist was found to be minimal in this case. The rehabilitation was done in close collaboration with the physiotherapist. Approval of the Ethics Committee, Pravara Institute of Medical Sciences, Loni, was obtained.
Technique
The patient' right hand was lubricated with a thin layer of petroleum jelly to prevent adherence of impression material to the skin and hair. The area around the hand was boxed and impression material, irreversible hydrocolloid (Alginate, Zelgan 2002, Dentsply, India; batch no. Z090218) was placed over the palmar side first and then the dorsal side to prevent tearing and distortion of the material. This technique also allows the hand to be removed from the impression with the fingers in flexion. 6 The patient was instructed to keep the hand in the normal resting position without stretching.
An impression (Figure 1) was then poured in stone plaster, Type III (Gold Stone, Asian Chemicals, India; batch no. 309251/25), and a positive replica of the hand was retrieved.
A donor whose finger dimensions and contours closely mimicked the fingers of the patient was chosen to reduce time required for sculpting. A putty impression (Aquasil putty, Dentsply, Germany; batch no. 0811003044) was made. Wax was then poured into the putty index and retrieved. The wax pattern was then hollowed from the inside by sculpting. The wax patterns were then placed on the cast and modifications in sculpting were carried out to resemble the digits of the other hand.
The wax pattern was then tried on the patient' hand. The wax patterns were relined with light body impression material (Reprosil, Dentsply, Germany, DE 19963-0359) (Figure 2) to

Irreversible hydrocolloid impression made.

Relined wax patterns.
achieve better fit. This was then poured in stone plaster, Type III (Gold Stone, Asian Chemicals, India; batch no. 309251/25). An indexed base was then made.
Stump model preparation
Since the prostheses were meant to be a ‘glove’-like construction, it was essential to ensure a snug fit of the silicone to the tissue. In order to provide a snug prosthetics fit, the stump was reduced accurately by around 0.5–1 mm, so that silicone stretches and flexes over the stumps as prostheses were fit.
Investment technique
Each stump with a keyed base and wax pattern was then invested in a custom-made box. The first pour was done until the junction of dorsal and ventral surface (Figure 3). Separating medium was then applied and a second pour was done to cover the entire wax pattern. Dewaxing was carried out and the flask was allowed to cool (Figure 4). A three-piece mould was thus obtained.
The advantage of this technique is that it eliminates the unsightly voids in the prosthesis commonly seen while using silicone, as it is more viscous and does not flow easily into inaccessible areas. It also facilitates color matching so that the under surface of the fingers can be matched first with a lighter shade and packed. Next the stump is inserted in place and the color on the dorsal surface, usually a darker shade, is matched and the packing is done.
Factor II Brand medical grade silicone MDX-4210 RTV (Room Temperature Vulcanizer), better known as Dow Corning Brand silicone, was used. The base color was dispensed (Figure 5) and intrinsic colors were mixed to achieve the required shade. The shade matching was carried out in natural light between 11:00 and 13:00 h (Figure 6). The dorsal

Investing of wax patterns.

Three-piece mould.

Medical grade silicone with intrinsic stains.

Shade matching.
and palmar aspects were mixed separately and characterization was incorporated. The patient' presence was critical to gain his approval.
The mould was packed separately for dorsal and palmar surfaces. Escape vents were provided to prevent air entrapment and for escape of excess material. The material was allowed to bench cure overnight. A commercial hair dryer was used for polymerization for 6–8 h. Residual silicone was left on the external surface to check polymerization.
Once the final prosthesis was retrieved, the flash was trimmed using a sharp blade and final finishing was accomplished using a silicone burs. To complete the prosthesis, an artificial nail was fabricated with cold cure clear acrylic resin layered on a pink cold cure acrylic resin (Dentsply, Rapid recovery powder; batch no. R080610). The nail was carefully fashioned to match those of the corresponding normal hand. A cynoacrylate adhesive was then applied on the under surface of the nail for bonding with silicone surface to achieve a realistic appearance.
The final step was placement of the prosthesis on the patient' hand in lieu of the missing finger. Since the prosthesis was extended up to the metacarpal-phalangeal joint, the patient was asked to wear a finger ring to mask the junction (Figure 7). The patient was instructed and demonstrated about the use (Figure 8) and maintenance of the prosthesis. The following suspension tests were carried out: (i) Tensile stress with static increasing load with gravity plus position, (ii) impact stress, and (iii) static proximal loading in gravity nil position.
Results
Adequate suspension was found with the prosthesis. The patient was satisfied with the aesthetics and was also able to resume functioning by holding light objects.
Discussion
The loss of even one finger produces significant deficiencies. The more dexterous individuals suffer the greatest degree of impairment. A prosthesis can often restore near normal function in distal phalange amputations. When part of the hand and two or more fingers have been amputated, requests are often made for a complete glove covering. Although this may be supplied, it must be appreciated that the surviving digits are unlikely to

Prosthesis in-lieu of missing fingers.
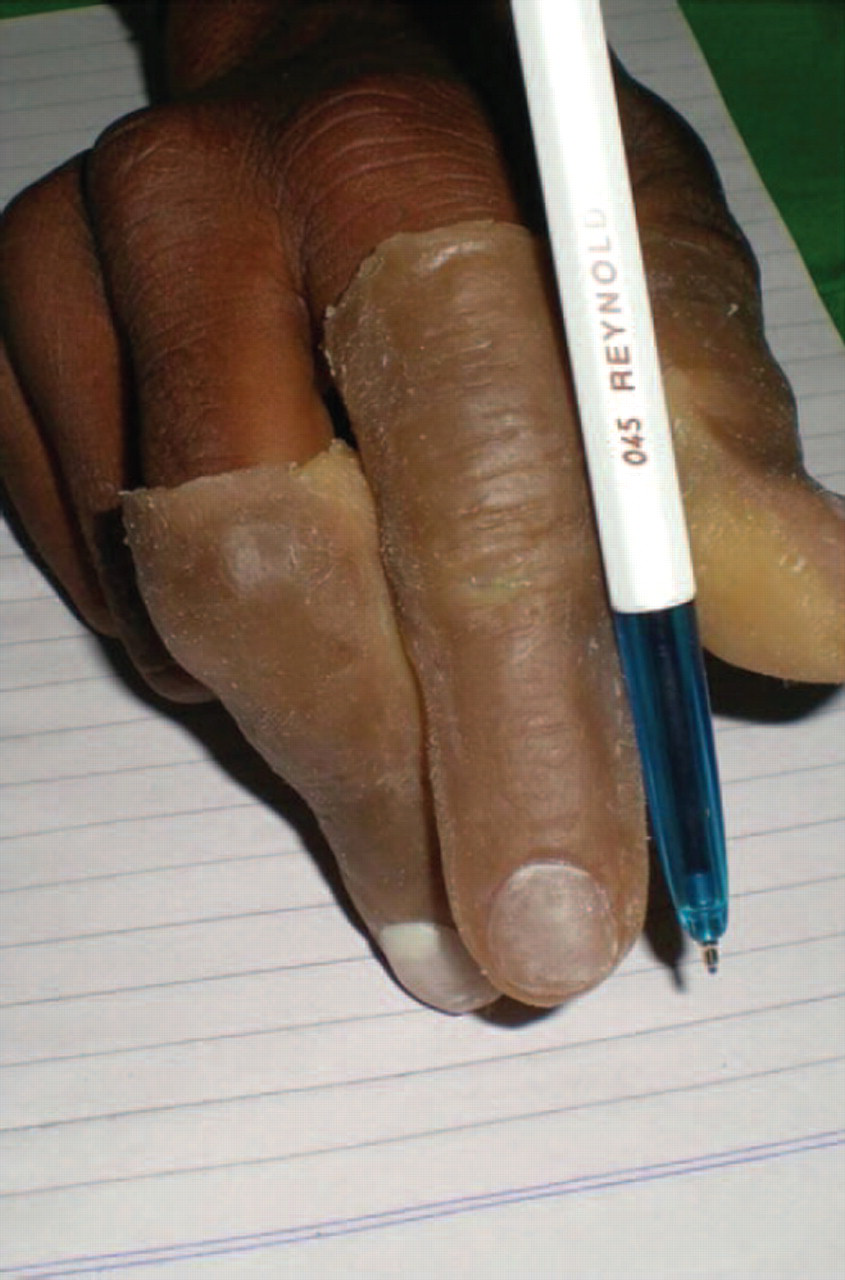
Prosthesis in function.
be comfortable. Function of the intact portion of hand will inevitably suffer while it is encased. Sweating is also a troublesome feature. 4 If at least one centimetre of mobile phalanx remains, some restoration of active grasp is feasible. The longer the residual finger the more secure the grip. 7 Silicone finger restorations may have additional functional benefits. Silicones unlike polyvinyl chloride prosthesis allow copying of the natural hand in every detail, the material is supple and not subject to ordinary thermal damage or ink stains. Thinness of the silicone prosthesis allows good sensibility through it. 8 Many traumatic amputees experience painful hypersensitivity at the termination of finger remnants. The gentle constant pressure of an elastomeric prosthesis can help desensitize and protect the injured tip. They also improve the hydration of stratum corneum of immature hypertrophic scars. 9 Prosthetic rehabilitation is quick, reversible, medically uncompromised and allows the surgical site to be closely monitored. 10 Creating a prosthesis that appears to have a realistic skin surface while achieving seamless visual integration with the surrounding tissue requires both artistic and technical expertise. The skin of the hand also changes color, not only by exposure to sunlight but also in response to elevation or dependency. 11 Placing a decorative ring over the margin of a finger prosthesis ending at metacarpal-phalangeal joint will make changing color of the hand less noticeable although the distal joint functions will be slightly restricted. 12 The ability to match skin tones requires a keen eye, good understanding of color therapy, and application and meticulous attention to detail.
Intrinsic coloration is a color applied within the mould during the casting procedure. It increases the service life of the prosthesis since color is less vulnerable to environmental conditions and handling and it does not interfere with sculpted surface texture or planned translucencies which are often compromised by application of extrinsic color. 13 Proper lighting is essential for an effective color match, so wherever possible, full spectrum color corrected lights are recommended. Medical grade Silicone was used for the fabrication of the prosthesis. The MDX-4210 is a RTV (Room Temperature Vulcanizer) and does not shrink on curing. This translucent silicone is compatible with all the intrinsic and extrinsic coloring systems available. 14 Significant advances in the field of material science have led to the production of new silicones with improved characteristics and improved methods of prosthesis coloration. 15
Conclusion
Experts in fields of prosthodontics, somato prosthesis and anaplastology have been playing an epicentric role in restoring anatomical contours. A psychological profile of the patient with proper counselling is also suggested to improve patient compliance. 3 The custom-made finger prosthesis is aesthetically acceptable, partially restores some degree of functionality and comfortable for patient use resulting in psychological improvement with personality development.