
Abstract
Background and aim:
Finger amputation is one of the most common types of amputation. Prosthesis with adequate suspension, user-friendly design, and an aesthetic appearance can be effective in the rehabilitation of these patients. The aim of this technical note was to propose a technique for fabrication of finger prosthesis with a new suspension approach for such patients.
Technique:
To design and accurately fabricate the socket of finger prosthesis, the socket was reduced by 2 mm less than the original value, and a central tunnel with 4 mm width and depth with length matching the distance between the end of the stump and the nail section was provided, so that the silicone material extended to the stump to provide appreciable suspension.
Discussion:
This study demonstrated the design and fabrication of a silicone finger prosthesis. It also showed silicone finger prosthesis with acceptable suspension, a user-friendly and light design, and a cosmetic appearance constructed for a patient with finger amputation.
Clinical relevance
Patients with finger amputation usually use prostheses with a simple suspension technique, but evidence suggests that the residuum of these patients experience atrophy and subsequently loss of appropriate suspension. Therefore, this study was required to provide an alternative suspension method in patients with finger amputations.
Background and aim
Finger and partial finger amputations are the most common types of partial hand amputation. Trauma is the most common cause of these amputations, 1 although congenital absence and deformities also have a role. 2 Hand deformity and amputation can affect a patient’s socioeconomic relationship because hand movement forms an important role in the activities of daily living. 3 Despite the fact that many advancements have occurred in surgical reconstruction techniques, 4 this type of surgery is not practical nor is it successful or indicated in many patients with partial finger amputations. Prosthetic rehabilitation of these patients has, however, been shown to help psychosocial aspects by providing increased grip strength and reduced hypersensitivity and pain.3,5
The design and fabrication of finger prosthesis, which is a combination of art and science, is an effective approach in the rehabilitation of patients with finger or partial finger amputation. 6 Suspension via the residual limb or stump is currently the main approach for attaching a finger prosthesis. 7 Suspension is one of the important concepts in finger prosthesis function to reduce displacement and increase performance of the amputated finger. In a suction type of suspension socket, due to the smaller internal dimensions of the socket compared to that of the stump and the elastic and nonporous structure of silicon, a vacuum state exists, which is formed by the cupping that provides appreciable suspension. 8 Adhesives, mechanical approaches, and anatomical methods have all previously been used as suspension methods to maintain the prosthesis position on the residuum, but wearing a prosthesis on the residuum has been shown to cause soft tissue atrophy after prolonged use, 8 and therefore, the suspension of such prostheses is challenging.
Although many suspension approaches have been developed in prosthetic finger suspension, there is still a requirement for a suspension method that has less drawbacks for patients with finger amputation who have atrophy of the stump when using suction suspension techniques for a finger prosthesis. Development of a simple approach of suspension in cosmetic finger prostheses when compared to conventional suspension is therefore important for these patients.
The aim of this technical note was to introduce a new technique in suspension of finger prostheses by fabricating silicone prostheses in people with partial finger amputation.
Technique
A 37-year-old male patient with partial finger amputation of the fourth finger was referred to the Natel Prosthetics Center, Tehran, Iran, for provision of a finger prosthesis (Figure 1). Examination of this patient showed the finger had been traumatically amputated at the proximal interphalangeal joint. The amputated finger demonstrated a thickened end and no signs of any infection in amputated finger. The rehabilitation team included contributions from an occupational therapist and physiotherapist to manage psychological and physiological issues associated with the traumatic amputation. A statement acknowledging informed consent was obtained from the patient before his participation in this study. The Ethics Committee of University of Social Welfare and Rehabilitation Science approved this study.
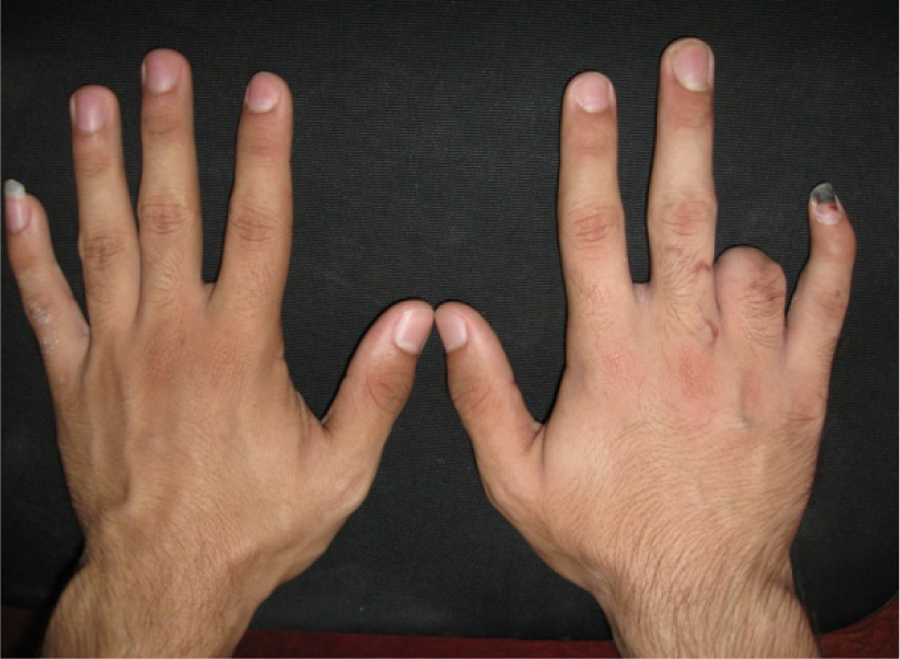
Partial finger amputation in right hand.
To obtain a good negative model and to prevent adhesion of the hand to the casting material, the amputated hand of the patient (right hand) was lubricated with Vaseline. Negative casting was performed with alginate (Tropicalgin; Zhermack, Italy) over the palmar and dorsal aspects of the patient’s hand. Using flexible material for casting allowed the fingers and hand to be removed easily from the cast, 6 which was performed in the neutral resting position of the hand. Plaster of Paris was then poured to provide a positive cast. To prepare and introduce the new method of suspension, the overall circular shape of the positive cast was reduced by removing 2 mm in depth, and a plastic dummy 4 mm in diameter, with a length that matched the distance between the end of the residuum and the nail region (as measured from the contralateral side), was added to the end of the stump (Figure 2).

Positive model of stump associated with dummy.
An adequate prosthetic fit is obtained by suitable fitting of prosthesis on residual limb by a suction method and by reduction of the circumference of the stump. To obtain a suitable suction suspension, the socket of the prosthesis was made smaller than the residual limb size by reducing the cast circumferentially (by 2 mm depth). To provide more suction suspension in finger prosthesis, we made a central tunnel with 4 mm width and depth with its length between ends of stump until nail section by adding a central tube (Figure 3). This tunnel provided suction when it was pushed on. The mechanical action involved exclusion of air within the tube, which provided additional suction between the inner circumference of the prosthesis and the circumference of the residuum model.
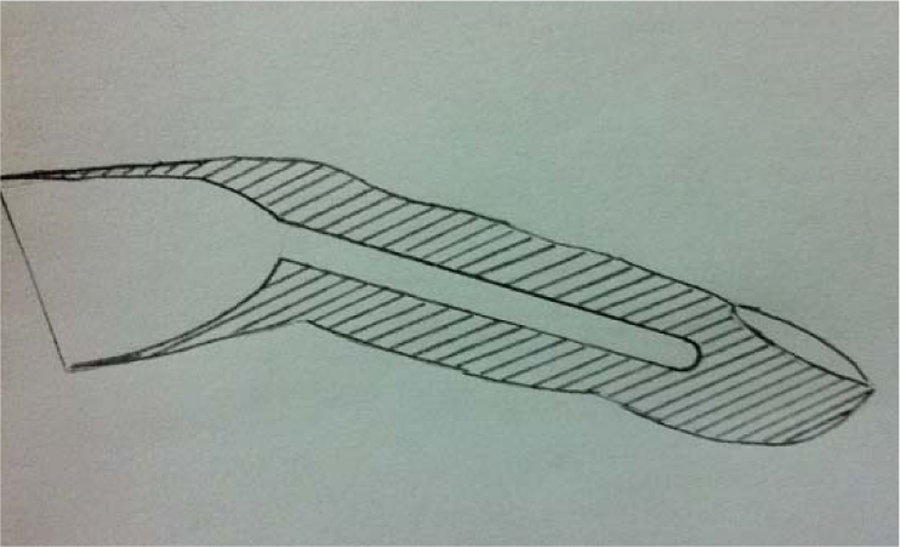
Schematic view of central tunnel in new method.
To reconstruct the lost parts of the finger, a negative cast was taken from the left ring finger (healthy side) by alginate. Melting wax (Covex Company, modeling wax, Netherlands) was then poured into the negative cast to construct a positive cast of healthy ring finger (Figure 4).

The wax pattern on the positive cast of the amputated finger.
The wax pattern was put on the positive cast of the amputated finger. Modifications in sculpting were performed to reconstruct the digit of the amputated hand to appear like the ring digit of the other hand, and then a negative cast was prepared using putty impression material (Aquasil putty, Dentsply, Germany) from the reconstructed finger that was provided by the wax (Figure 5).

Negative casts from putty impression material from the reconstructed finger.
In readiness for silicon injection, the reconstructed wax finger and putty impression cast were placed in boiling water for 10 min to melt the wax that was used in the reconstructed format. After this stage, based on a patient’s skin color, silicone biomaterial was mixed with coloring and then poured into the putty impression cast, and the positive cast of the stump associated with plastic dummy was put on silicon material. After 24 h, the positive cast of the stump and dummy was removed and the silicone finger prosthesis was brought from the putty impression cast. After preparation of the silicone finger with the new method of suspension, an artificial nail was constructed with pink cold cure acrylic resin (Dentsply, Rapid recovery powder, Acropars, Marlik Company, Iran). The nail was carefully polished to resemble the nails of a normal hand. A cynoacrylate adhesive was used to bond nail to the silicone surface. The final stage of the prosthesis manufacture was to put the silicone finger prosthesis with the new suspension method on the amputated finger (Figure 6). The patient was advised about the appropriate use and maintenance of the prosthesis.
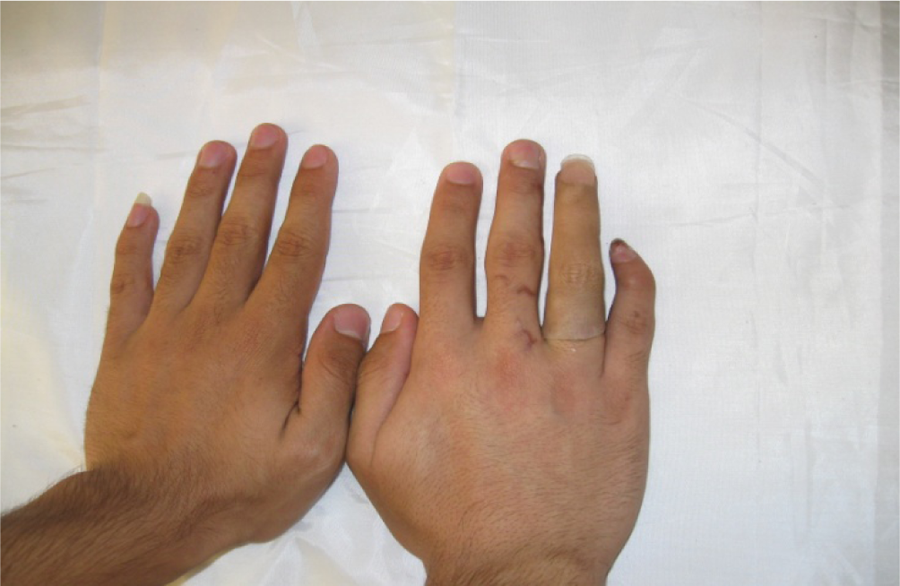
Silicone finger prosthesis with new suspension method on the amputated finger.
Results
Through this technique, good suspension was obtained with the finger prosthesis. Satisfactory and acceptable aesthetics and functional performance were demonstrated in this study.
Discussion
Providing good suspension using an appropriate suspension method is important in aesthetic prostheses. 9 Adhesives and other approaches have historically been used to provide suspension in finger prostheses.2,6,7 Our study introduced the use of new method of suspension by providing a suction tunnel on the socket of the stump. Based on previous studies performed in this field, which showed the disadvantages of stump atrophy, skin motion and lessening, 7 using this new method could potentially provide a more effective solution to hold the finger prostheses in place.
The amputation of a finger or partial amputation has been shown to have a significant impact on the physiological and psychological aspects of daily living.1,3 According to the level of amputation in the finger and the number of fingers that have been amputated, a patient may be faced with either simple or complex dysfunction as compared to normal hand activity. Finger prostheses can restore the function of an amputated finger close to that of a normally functioning hand, especially in distal phalange amputations.
After 6 months of use, this new design of prosthesis utilizing a new approach of suspension provided safe and reliable use with no problems with suspension. The user-friendly and light design of the prosthesis decreased skin sensitivity risk, increased the useful time of prosthesis use, and provided a low cost method of suspending a finger prosthesis. The advantage of this technique was that suspension was achieved via snug fitting on the stump even when it was atrophied. This method of suspension eliminated the use of additional suspension approaches such as using adhesives. To remove the finger prosthesis in this new method, negative pressure in tunnel region of the prosthesis would need to be removed, meaning a high force would need to be applied to remove the prosthesis. Providing suction inside the socket caused a negative pressure to be applied to the stump, which prevented dislocation of the finger prosthesis.
Using silicone as a biomaterial in fabrication of finger prosthesis allowed a high-quality and natural finger design, and the thin-layered socket that covered the stump of the finger prevented obtrusion. We did not evaluate the efficacy of the suspension afforded in this method compared to that provided by a traditional suspension method. Comparison between this method and a simple sleeve suspension with an appreciative measurement instrument would be beneficial for inclusion in a future study.
Prosthetists have formed an important role in the design and fabrication of finger prostheses as a viable rehabilitation approach for these patients. To prepare compliance, psychological counseling can be a useful approach in such patients. 8 The results of this study indicated that a custom mold finger prosthesis with acceptable suspension, a good aesthetic appearance, and adequate functionality may be developed for the benefit of patients with traumatic finger amputation.
Key points
Finger and partial finger amputations are the most common types of partial hand amputation.
Providing good suspension using an appropriate suspension method is important in aesthetic prostheses.
To provide more suction suspension in finger pros-thesis, we made a central tunnel with 4 mm width and depth with its with its length matching the distance between the ends of the stump and the nail. This tunnel provided suction when the prosthesis was pushed into position. In mechanical terms, the air within the groove was excluded and provided additional suction between the inner circumference of the prosthesis and the circumference of the residuum model.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.