
Abstract
Keywords
After decades of reductions in smoking rates there is increasing recognition within the tobacco control community that future gains in reducing tobacco use will increasingly require addressing other markers of disadvantage that are now more commonly associated with smoking, including the strong association between smoking and mental illness. The high proportion of people with mental illness who smoke, and conversely the high proportion of adult smokers who have a mental illness [1–3] has led tobacco control groups to suggest strategies for this group. One such strategy is the establishment and maintenance of smoke-free policies in mental health treatment facilities. In the UK, psychiatric inpatient facilities have been required to be smoke-free since July 2008 [4]. In the USA, some individual facilities have introduced smoke-free policies but these have been contentious [5]. Some Canadian regional health authorities and individual hospitals have implemented smoke-free policies [6,7]. In Australia, this has been recommended by the National Preventative Health Taskforce [8,9], and smoke-free policies have been, or are being, implemented in a number of states and territories [10,11].
Since the discovery in the 1950s of medications that are effective in treating the symptoms of severe mental illnesses there have been significant changes in the delivery of mental health services. By the 1970s most psychiatric hospitals had been dramatically reduced in size, and new modes of outpatient-based and community-based services were under development [12,13]. As a result of these changes, the nature of psychiatric service delivery has fundamentally altered. Patients who spend months or years in smoke-filled back wards of psychiatric hospitals are now very much in the minority. Most inpatient psychiatric admissions are now of short duration to deal with acute psychiatric crises, with follow-up care being delivered in the community, and most people with mental illness now spend most of their time living in the community with limited contact with specialist services. This suggests that smoke-free policy initiatives are only one of a number of strategies needed to address the high rates of smoking for people with mental illness, and that the bulk of our efforts should lie in providing greater support to these populations in the community.
We sought to examine the extent to which smoke-free policies in mental health facilities, as part of a broader strategy to address smoking cessation in people with mental illness, might contribute to the goal of reducing rates of smoking in people with mental illness. We aimed to quantify smoking rates in users of mental health services, and the degree to which smokers with mental illness have contact with psychiatric inpatient services. We used data from the 2007 National Survey of Mental Health and Wellbeing to estimate prevalence of smoking in people with mental illness by whether or not they have been hospitalized for mental health problems, and data from the Western Australian Mental Health Information System to determine the prevalence and average duration of inpatient psychiatric admissions.
Materials and methods
Data sources
National Survey of Mental Health and Wellbeing
This survey, which was conducted by the Australian Bureau of Statistics with funding from the Australian Government Department of Health and Ageing, comprised a random sample of 8841 participating adults aged 16 to 85 years. Fieldwork was conducted between August and December 2007. The survey included residents of private dwellings only, and did not cover people living in long-term in psychiatric facilities. Data collection was undertaken by means of computer-assisted personal interviewing. Full details of the survey methodology have been reported elsewhere [14,15].
Mental Health Information System
The Mental Health Information System (MHIS) records contacts with mental health services in Western Australia (WA). This database was commenced in 1966. It covers all inpatient admissions to private or public hospitals in WA where a diagnosis of mental disorder or self-harm is made or where contact is made with a specialist psychiatric service. The system also records outpatient-based and community-based contacts with state run mental health services [16].
Measures
The National Survey of Mental Health and Wellbeing (NSMHWB) identified mental disorders using the Composite International Diagnostic Interview (CIDI) Version 3 [17]. The CIDI is a fully structured interview questionnaire assessing six main anxiety disorders: panic disorder, agoraphobia, social phobia, generalized anxiety disorder, obsessive–compulsive disorder and post-traumatic stress disorder, three affective disorders: depressive disorder, dysthymia and bipolar affective disorder, and three substance use disorders: alcohol harmful use, alcohol dependence and drug use disorder. Low prevalence disorders such as schizophrenia were not assessed in the survey.
The MHIS identifies mental disorders using ICD-8, ICD-9 or ICD-10. ICD-9 was introduced in 1979, followed by ICD-10 in 2000. We identified hospital admissions for mental disorders if an ICD-8 or ICD-9 chapter 5 diagnosis, or ICD-10 chapter F diagnosis was made.
Smoking status was measured in the NSMHWB by asking respondents ‘Do you currently smoke every day, at least weekly, less than weekly, or not at all?’ Respondents were also asked about hospitalizations for mental health problems. Respondents were given the definition: ‘The next few questions are about problems with your mental health. This includes but is not restricted to such things as stress, anxiety, depression or dependence on alcohol or drugs.’ Respondents were then asked: ‘With this definition in mind have you ever been admitted overnight or longer in any hospital for problems with your mental health?’ and ‘In the past 12 months how many times were you admitted overnight to any hospital for problems with your mental health?’
From the MHIS data, length of stay in hospital was calculated from admission and discharge dates, minus any periods of approved leave. We focused on the median length of stay as the distribution of lengths of stay is strongly skewed, with the small proportion of stays of many years duration affecting the mean duration.
On the MHIS, where patients have had multiple admissions, it is possible that more than one principal diagnosis may have been assigned over the course of those admissions. For this study, principal psychiatric diagnosis was assigned by giving preference to later diagnoses subject to a hierarchy that would give preference to an earlier diagnosis if the later diagnosis was less informative or likely to refer to a comorbidity. Full details of this method are described elsewhere [16].
Ethics
As the NSMHWB data are publicly available confidentialized files, no institutional ethics approval was required for this analysis. Access to the MHIS was approved by the Human Research Ethics Committee of the Department of Health, Government of Western Australia.
Analysis
As the NSMHWB was a stratified multi-stage area-based survey, survey weights were applied to calculate estimates of totals and proportions. To account for the complex sampling design, standard errors and confidence intervals were calculated using the jack-knife method of replicate weighting [18,19].
We calculated the proportion of the WA adult population who had contact with mental health services from the MHIS. Numerator counts were extracted directly from the MHIS. Population denominators were taken from estimated resident population counts provided by the Australian Bureau of Statistics [20].
Results
National Survey of Mental Health and Wellbeing
Only a small proportion of smokers with mental health problems had been hospitalized for a mental health problem in the year prior to the survey. Of the estimated 3 567 000 adult smokers in Australia, an estimated 1 156 600 smokers had a mental illness in the 12 months prior to the survey, representing 32.4% of adult smokers (95%CI: 29.5–35.3). However, only 1.4% of adult smokers (95%CI: 0.5–2.4) reported being hospitalized for a mental health problem in the 12 months prior to the survey, an estimated 50,900 smokers nationwide. In terms of lifetime prevalence of mental disorders, the majority of current adult smokers had met CIDI diagnostic criteria for one or more mental disorders at some stage of their lives (66.6%; 95%CI: 63.2–70.1), but only 6.3% of adult smokers reported ever being hospitalized for a mental health problem (95%CI: 4.9–7.8) (Table 1).
Estimated number of smokers, smoking rate and proportion of all smokers, by mental health status and whether ever hospitalized for a mental health problem, Australian National Survey of Mental Health and Wellbeing
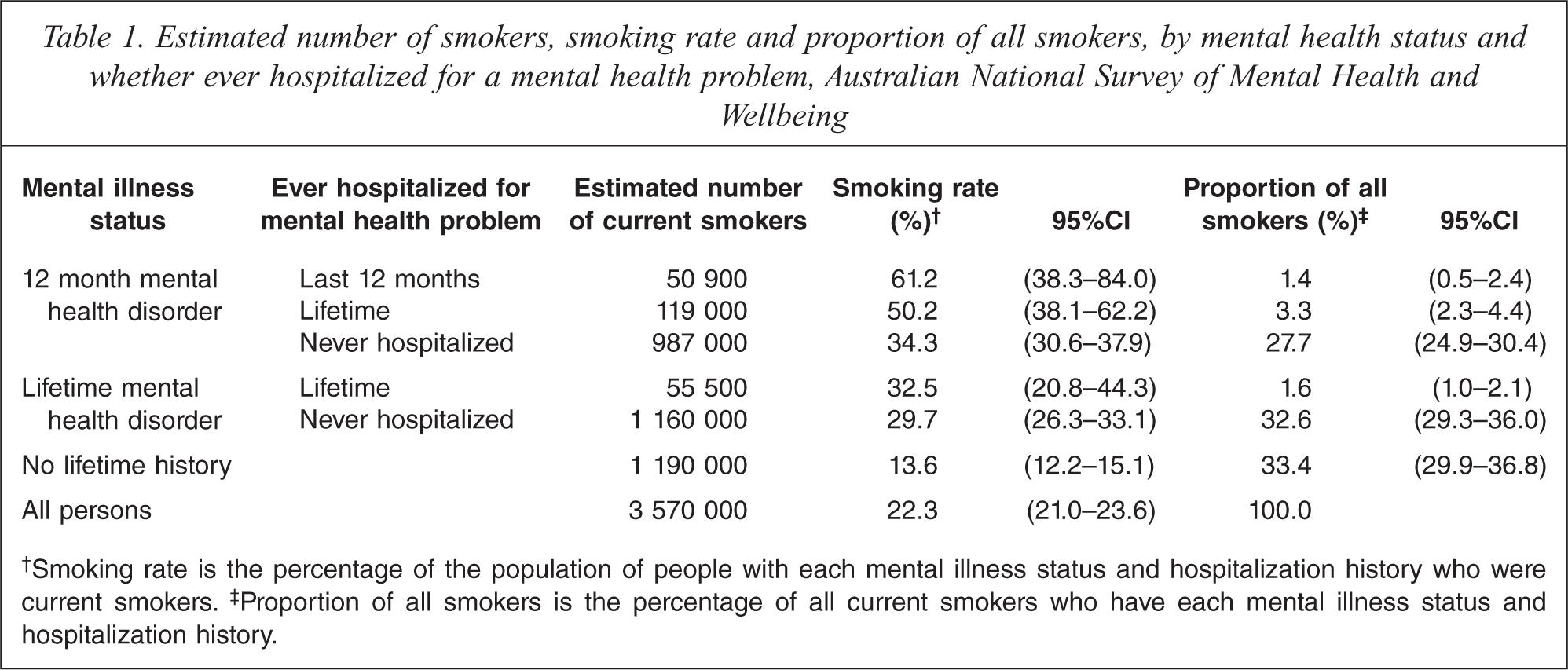
Smoking rate is the percentage of the population of people with each mental illness status and hospitalization history who were current smokers.
Proportion of all smokers is the percentage of all current smokers who have each mental illness status and hospitalization history.
Using the NSMHWB, the estimated proportion of the total adult population of 16 015 000 who had been hospitalized for a mental health problem in the last year was 0.52% (95%CI: 0.29–0.75). The proportion of this group who are current smokers was 61.2% (95%CI: 38.3–84.0).
WA Mental Health Information System
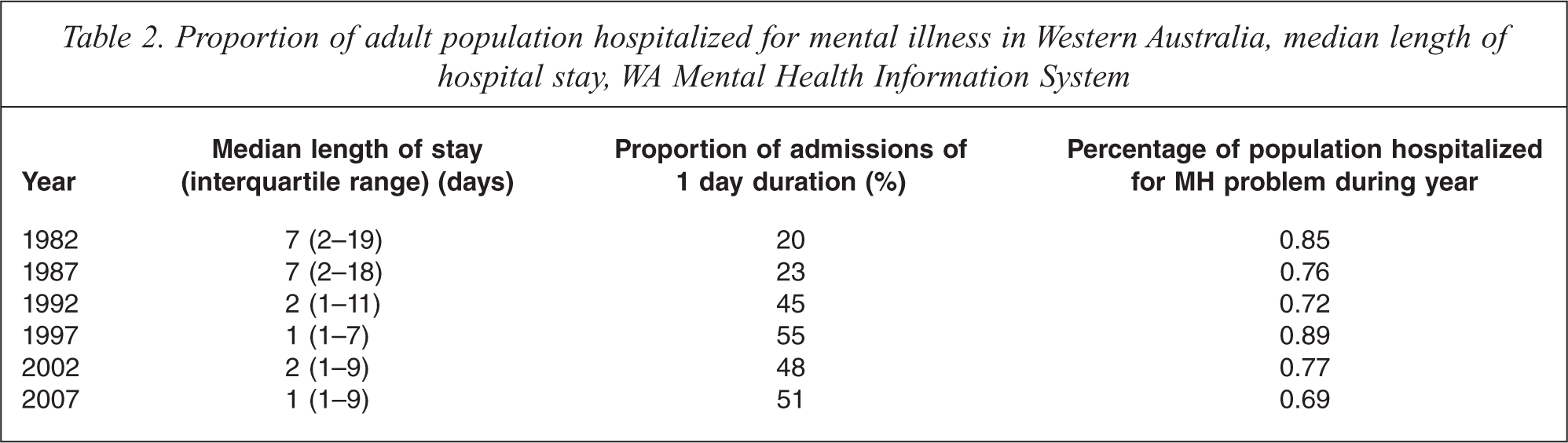
The median length of stay in hospital for people in contact with mental health inpatient services dropped from 7 days in 1982 to 1 day in 2007. The proportion of the WA population who had been hospitalized for mental health problems in 2007 was 0.69% (Table 2). Some difference in estimates between the MHIS and the NSMHWB could be expected as the NSMHWB was a household survey that did not include people living in non-private dwellings, such as long-term residents of psychiatric hospitals or hostels.
Proportion of adult population hospitalized for mental illness in Western Australia, median length of hospital stay, WA Mental Health Information System
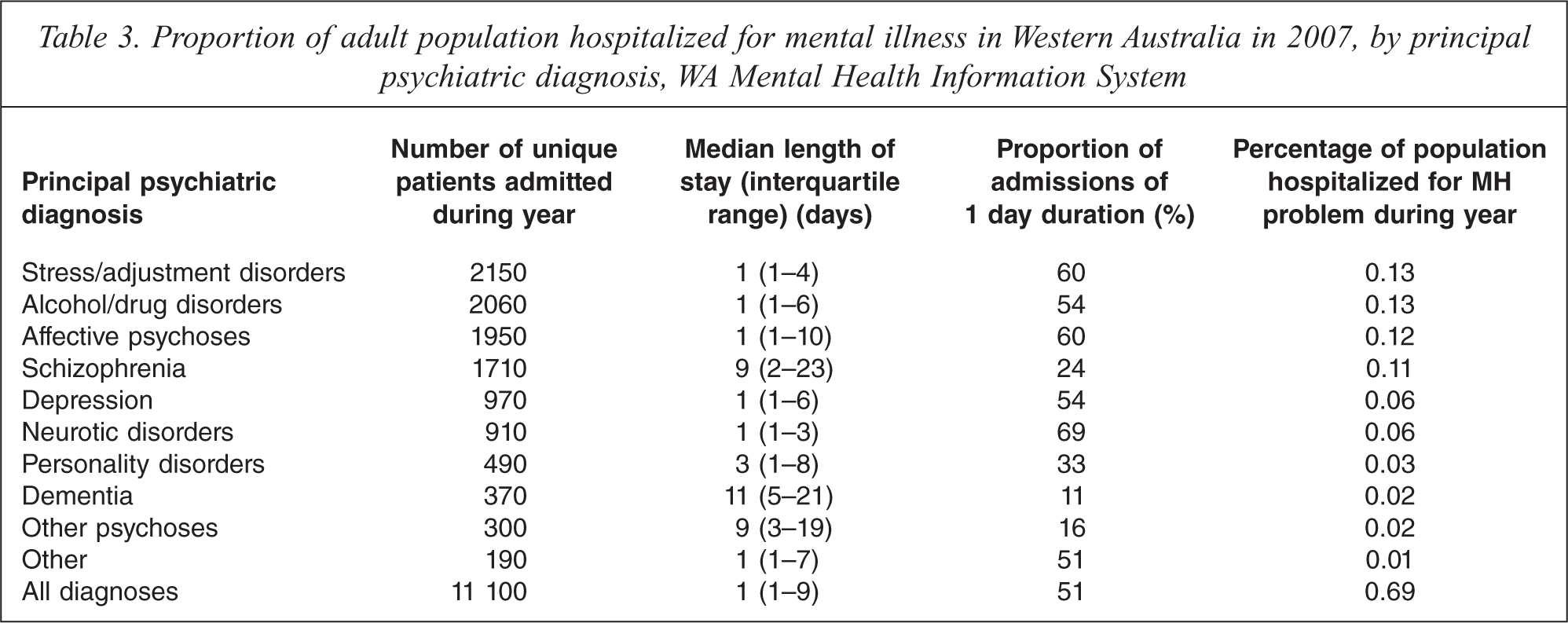
Patients with a principal psychiatric diagnosis of dementia had the longest median length of stay, followed by patients with schizophrenia and other psychoses (excluding affective psychoses). With the exception of personality disorders, all other disorders had a median length of stay of one day. Short-term admissions made up the majority of psychiatric inpatient contacts in 2007 in WA with 51% having duration of one day (overnight stay or same day discharge) and 57% of two days or less (Table 3).
Proportion of adult population hospitalized for mental illness in Western Australia in 2007, by principal psychiatric diagnosis, WA Mental Health Information System
Discussion
These data confirm that the rate of cigarette smoking is very high among people who have been hospitalized for mental health problems. These people are likely to benefit, not only in terms of their physical health, but also in terms of their mental health, as well as financially, if they quit smoking [21–24]. These data are consistent with previous studies of institutionalized patients [25,26]. They also show that while people with current mental illness comprise one third of Australia's adult smokers, the vast majority are not in contact with inpatient services. Less than 1% of the adult population in WA has an inpatient admission for a mental health condition per year. While smoke-free policy may be an important component within a coordinated continuum of smoking cessation support for people with mental illness who are in contact with inpatient services [27], it is very unlikely that the implementation of smoke-free policies in mental health inpatient facilities will have any impact on smoking rates in the large proportion of smokers with mental illness who do not have contact with inpatient facilities. Other strategies, including targeted population-based strategies, are required to address the needs of this often neglected group [28,29].
In addition to addressing smoking in psychiatric patients, smoke-free psychiatric facilities have been proposed and supported for a number of other reasons: the symbolism of showing that health care facilities do not support smoking, achieving cultural change amongst staff, providing a smoke-free working environment for staff, and a smoke-free environment for non-smoking patients [10,11,30]. While these are all important and achievable goals, the debate over whether and how to implement smoke-free mental health facility policies should not distract from the larger issue of how to reduce smoking among people with mental illness including the large group of people with mental illness who are not in routine contact with mental health services. Supporting smoking cessation is a larger responsibility of many and should involve motivation and self-efficacy of the person, and systems of support that extend beyond the inpatient setting to the community as well. This should include government and non-government community mental health services, and other agencies that have contact with people with mental illness including non-government organizations and support groups, general practitioners and supported accommodation facilities.
Implementing a smoke-free policy, in and of itself, has not been shown to have any impact on achieving smoking cessation unless it is part of a more comprehensive approach to smoking cessation [31,32]. It may contribute to the establishment of more comprehensive smoking cessation approaches if it facilitates cultural and behavioural change among staff who would otherwise explicitly reinforce smoking by smoking with patients, or implicitly reinforce smoking by doing nothing to acknowledge and manage its clinical interaction with mental disorders.
Although the proportion of smoking adults who are seen in inpatient psychiatric services is small, and the proportion in long-term psychiatric inpatient care smaller again, the rate of smoking within this group is high. Psychiatric services have long neglected the issue of smoking [33–35]. Despite the high level of nicotine dependence in this group, there is evidence that severely mentally ill patients are able to quit smoking when given appropriate opportunities and support to do so [36–39].
Some have argued that forcing people to attempt to quit smoking impinges on their human rights – the right of informed and rational adults to choose healthy or unhealthy behaviours as they wish [40]. Rather than making a free choice as adults, most adult smokers commenced smoking in adolescence and continue to smoke in adulthood because of their addictions. It has also been argued that there can be an ethical dilemma in enforcing smoking cessation on patients against their will, particularly if they are acutely unwell and have been hospitalized involuntarily, given the lack of evidence that such interventions can produce sustained smoking cessation following discharge from care [41,42]. Depending on how smoke-free policies are implemented, some patients can be advantaged while others might suffer some disadvantage while not reducing their dependence on cigarettes. While some patients may be successful in quitting smoking after being treated in a smoke-free psychiatric facility, it is also possible that some patients will be discouraged from making their own quit attempts by the failure of their enforced quit attempt during a psychiatric hospitalization. Others may be reluctant to seek inpatient treatment if they do not wish to undergo an enforced quit attempt. For instance, the introduction in Ontario of a smoking ban in all inpatient units was initially associated with a fall in visits to psychiatric emergency departments by patients with psychotic disorders [43].
Although most psychiatric inpatients would benefit from quitting smoking, there would be a small number of cases of, for example, people with terminal illnesses and suffering cognitive or memory impairment that prevent them from understanding or remembering the smoke-free status of an institution, where the benefits of enforcing smoking cessation may not outweigh the challenges involved. In tobacco addiction and recovery, as in many other areas of health care, there is no single right approach. The best way to motivate and support one person to quit smoking may not be effective for another.
The results of this study also confirm the changed nature of psychiatric service delivery, with the majority of inpatient episodes being of short duration. As such, support following discharge is a crucial aspect of successful programmes. After one or two days in inpatient care, patients who commenced a quit attempt during an inpatient episode will be discharged at a time when they are still facing significant withdrawal symptoms, and peak intensity of withdrawal symptoms may occur after discharge. The first weeks after discharge are a time of high vulnerability to return to smoking. Desire to quit is an important predictor of successful smoking cessation [44]. Motivating patients to quit smoking prior to discharge is also an important part of successful programmes [45,46]. This could include the use of techniques such as motivational interviewing [47], or smoking cessation counselling. Smoking cessation counselling within the general hospital setting has been shown to be effective when it is delivered by someone specifically employed and trained for the task [48,49], but not when it is delivered by someone trying to fit it in with their other duties [50]. Its effectiveness is yet to be evaluated in inpatient psychiatric settings.
Evaluations of the success of smoke-free services on short-term smoking cessation have found that most smokers resume smoking as soon as they are discharged. For example, a study of 100 patients admitted to a smoke-free psychiatric unit for an average stay of about a week found that all resumed smoking within about 5 weeks of discharge. The median time from discharge to the first cigarette was 5 minutes, with a range from a few seconds to 36 days [31].
It is unknown whether failure of an enforced smoking cessation attempt affects a patient's likelihood of undertaking or succeeding in a subsequent attempt, although nearly half of those in this study (48%) reported a later quit attempt. Some participants reported increased expectancy of success with quitting and decreased expectancy of difficulty with staying quit in the future [51].
Evaluations of smoke-free policies and programmes in psychiatric facilities almost always focus on whether it has been possible to achieve a smoke-free environment and sustain it [52,53]. For instance, adverse reactions, such as behavioural difficulties and violence, are rare [54]. While there are important lessons from these studies as to the programme and environment components necessary to be able to implement smoke-free policies, the success of the strategy hinges on whether sustained smoking cessation can be achieved. Evaluations rarely measure the impact of the programme on smoking rates of the patients seen by services, or whether smoking cessation attempts started during an inpatient admission are sustained for any period of time after discharge. This sort of evaluation should be an integral part of the evaluation of the effectiveness of smoke-free policies within a larger goal of smoking cessation support across the continuum of care.
Further research is needed to better understand the programme components that will facilitate the greatest level of smoking cessation in psychiatric patients. For instance, better understanding of the effects of smoking cessation efforts in acutely ill psychiatric patients with short inpatient stays is required. Also, many evaluations of smoking cessation treatments have either been evaluated in samples that explicitly exclude psychiatric patients, or when they were included, only patients in remission, not acutely ill inpatients are studied [55].
Limitations of our study include reliance on self-report data of smoking status and psychiatric admissions in the NSMHWB. However, the fact that there was good agreement concerning psychiatric admission between the NSMHWB data and information from the WA MHIS gives some assurance that the NSMHWB self-report data are reasonably reliable.
Just making facilities smoke-free will not of itself reduce smoking in people with mental illness. Smoke-free policies need to be embedded within a larger programme that motivates patients to seek to change their smoking behaviours, that provides appropriate and evidence-based supports to assist in quit attempts, and that provides an appropriate level of support following discharge from inpatient care to increase the likelihood of smoking cessation being maintained. This may include the use of techniques such as motivational interviewing, cognitive behavioural therapies, mindfulness, peer support and access to nicotine replacement therapy [55–58].
The goal of creating and sustaining smoke-free mental health services should be secondary to the goal of reducing tobacco-related morbidity and mortality in people with mental illness by reducing uptake and promoting cessation, and this goal is just one aspect of the overall goal of mental health services, to provide the most appropriate health care for people with mental illness. People with mental illness constitute a third of smokers in the USA and Australia, and consume over 40% of cigarettes smoked [1–3]. As a group, people with mental illness smoke at a higher rate, have higher levels of nicotine dependence, have more difficulty quitting, and smoke for longer than people with no mental illness [2,29,59]. This gives strong support to the need for comprehensive tobacco cessation strategies aimed at this group of smokers. The debate over smoking bans in mental health facilities should not divert attention from the needs of the much larger number of smokers with mental health problems who do not receive inpatient treatment.