
Abstract
Objective:
To describe and compare the health profiles and health service use of people hospitalised with severe mental illness, with and without psychotic symptoms.
Methods:
We conducted a historical cohort study using linked administrative datasets, including data on public hospital admissions, emergency department presentations and ambulatory mental health service contacts in New South Wales, Australia. The study cohort comprised 169,306 individuals aged 12 years and over who were hospitalised at least once with a mental health diagnosis between 1 July 2002 and 31 December 2014. Of these, 63,110 had a recorded psychotic illness and 106,196 did not. Outcome measures were rates of hospital, emergency department and mental health ambulatory service utilisation, analysed using Poisson regression.
Results:
People with psychotic illnesses had higher rates of hospital admission (adjusted incidence rate ratio (IRR) 1.26; 95% confidence interval [1.23, 1.30]), emergency department presentation (adjusted IRR 1.17; 95% confidence interval [1.13, 1.20]) and ambulatory mental health treatment days (adjusted IRR 2.90; 95% confidence interval [2.82, 2.98]) than people without psychotic illnesses. The higher rate of hospitalisation among people with psychotic illnesses was driven by mental health admissions; while people with psychosis had over twice the rate of mental health admissions, people with other severe mental illnesses without psychosis (e.g. mood/affective, anxiety and personality disorders) had higher rates of physical health admissions, including for circulatory, musculoskeletal, genitourinary and respiratory disorders. Factors that predicted greater health service utilisation included psychosis, intellectual disability, greater medical comorbidity and previous hospitalisation.
Conclusion:
Findings from this study support the need for (a) the development of processes to support the physical health of people with severe mental illness, including those without psychosis; (b) a focus in mental health policy and service provision on people with complex support needs, and (c) improved implementation and testing of integrated models of care to improve health outcomes for all people experiencing severe mental illness.
Introduction
As with jurisdictions across the globe, mental health service provision in Australia has evolved substantially over the past 40 years, with residential institutional care being replaced by a complex and only partially integrated model (National Mental Health Commission [NMHC], 2019). In Australia, services are funded by a combination of national government, state and territory governments, and the private and non-government sectors. This model comprises acute care (including emergency community-based mental health teams, emergency department [ED] and admitted patient care), community mental health care services, primary care delivered in general practices, outpatient clinics, private psychiatry and psychology clinics, and by non-government organisations (Australian Institute of Health and Welfare [AIHW], 2020). The changes in the funding and delivery of services are legacies of the Richmond Report in New South Wales (NSW) and other subsequent recommendations for accessible community-based interventions for people experiencing severe mental illness (SMI) (Australian Health Ministers, 1992; Richmond et al., 1983). Yet, debate continues over how resources and service models can facilitate access for groups with different clinical needs. For example, the funding and development of community-based health care services for people with SMI have historically prioritised people with psychotic disorders, such as schizophrenia spectrum disorders (McGorry, 2015). It is known, however, that people experiencing other forms of SMI (e.g. severe mood, anxiety and personality disorders) frequently come into contact with acute health services, at times due to a lack of availability, suitability or appropriate equipping of community-based services (Berren et al., 1999; Dark et al., 2017; Decoux, 2005; Productivity Commission, 2019). It is therefore unclear whether current models of health service provision that have evolved through a focus on psychotic disorders are appropriately geared to meet the needs of people experiencing other types of SMI.
In response to the higher rates of morbidity and mortality experienced by people with SMI (Laursen, 2011; Morgan et al., 2011, 2017), priority areas of the current Australian Fifth National Mental Health and Suicide Prevention Plan (Fifth Plan) include coordinated treatment and supports for people with severe and complex mental illness, as well as improving the physical health of people living with mental illness with a view to reducing early mortality (Department of Health, 2017). Although the Fifth Plan does not distinguish between people with and without psychotic disorders, programmes rolled out to address morbidity among those with SMI have primarily prioritised people experiencing psychosis (e.g. Curtis et al., 2016, 2018; International Physical Health in Youth [iphYs] Working Group, 2013; Watkins et al., 2020). This prioritisation in part reflects the fact that people with schizophrenia represent the largest proportion of individuals who access community mental health services in Australia (AIHW, 2020), as well as the varied definitions of SMI that may be utilised by health services, some of which require a diagnosis of psychotic illness (Ruggeri et al., 2000; Schinnar et al., 1990). Increasingly recognised is that a substantial proportion of people with other types of mental health disorders (e.g. depression, anxiety and personality disorders) experience severe illness affecting both physical and mental health (Arvidsson, 2009; Firth et al., 2019), including high rates of physical comorbidities such as cardiovascular disease (Hare et al., 2014), cancer (Evans et al., 2005), chronic pain (Bair et al., 2003; McWilliams et al., 2003), asthma and diabetes (Stubbs et al., 2017). As a result, there is now increased awareness of the need to advocate for better physical health care for all people with SMI, not just psychotic illnesses (Firth et al., 2019; NMHC, 2016).
Strategic directions of mental health reform in NSW (NSW Ministry of Health, 2014, 2018) include supporting a greater focus on community-based care and developing a more responsive system for people with complex needs, including those hospitalised with physical health problems. While there has been significant knowledge gained about the health service utilisation of people living with psychotic disorders, it is important to understand the health needs of people both with psychotic SMI and with other types of non-psychotic SMI. This understanding is required to ensure that the needs of all people with SMI are represented throughout the development and implementation of mental health policy and to facilitate the planning of health services to appropriately meet their needs. The aims of this study were to describe and compare the health profiles and rates of health service use following a mental health–related hospitalisation for people with SMI (with and without psychotic illness), using a large linked dataset of hospital admissions in NSW. For the purposes of this report, SMI is indicated by the requirement for inpatient services in the treatment of a mental health condition (i.e. people with high intensity needs; Productivity Commission, 2019).
Method
Datasets and record linkage
The linked datasets utilised in this study have been described elsewhere (Reppermund et al., 2019). The following datasets were used to obtain outcomes of interest in the current report: the Admitted Patient Data Collection (APDC); Emergency Department Data Collection (EDDC); Mental Health Ambulatory Data Collection (MH-AMB); NSW Registry of Births, Deaths and Marriages (RBDM). The APDC (1 July 2001–31 December 2015) contains information on all admissions to public and private hospitals, including psychiatric facilities, in NSW. The data contain information on dates of admission and discharge, up to 51 diagnoses, and any medical procedures relevant to each hospital episode. The EDDC (1 January 2005–31 December 2015) contains information on all ED presentations to the majority of public ED centres in NSW (90 out of 150). The data contain information about the date of, reason for, and outcome of the visit. The MH-AMB (1 January 2001–31 December 2015) contains information on patient access to NSW public ambulatory (i.e. community) mental health services. This includes mental health day programmes, psychiatric outpatients and outreach services; it does not include services provided in primary care or private services. The RBDM (1 January 1994–31 December 2015) contains information about fact of death for all people who died in NSW. Deidentified linkage of the datasets was performed by the NSW Centre for Health Record Linkage based on a statistical linkage key (SLK581) and unit record data were sent to researchers after removal of personal identifiers.
Study population
The study population comprised individuals aged between 12 and 100 years who were admitted to a public NSW hospital (to either a mental health unit or a non-mental health unit) with a mental health diagnosis in NSW from 1 July 2002 to 31 December 2014 (see below for specific ICD-10 [International Classification of Diseases] diagnosis codes). While it is acknowledged that psychotic symptoms can present outside the age limit of 12–100 years on rare occasions, the upper limit for age was used in the current study to exclude persons with implausible ages and erroneous entries in the dataset. We classified people according to the presence of psychotic illness, forming a group of people with psychotic SMI and a comparison group (non-psychotic SMI). For the psychotic SMI group, individuals required at least one hospital episode with any of the following ICD-10 AM codes recorded as the principal diagnosis relevant to the admission: schizophrenia spectrum and delusional disorders (F20, F22, F24); drug-induced and other organic psychotic disorders (F06.0, F06.2, F10–F19 subtypes .5 and .7, F53.1); schizoaffective disorder (F25); mood/affective disorders with psychotic symptoms (F30.2, F31.2, F31.5, F32.3, F33.3); acute psychotic disorders (F23); and other psychotic disorders (F28–F29).
For the non-psychotic SMI group, individuals required at least one hospital episode with a principal diagnosis of any of the following: mood/affective disorders without psychotic symptoms (F30.0, F30.1, F30.8, F30.9, F31.0, F31.1, F31.3, F31.4, F31.6, F31.7, F31.8, F31.9, F32.0, F32.1, F32.2, F32.8, F32.9, F33.0, F33.1, F33.2, F33.8, F33.9, F34, F38, F39); anxiety, neurotic, stress related and somatoform disorders (F40, F41, F42, F43, F44, F45, F48); schizotypal disorder (F21); and disorders of personality and behaviour in adulthood (F60, F61, F68, F69). To ensure absence of psychotic disorders from the diagnostic profile of people included in the non-psychotic SMI group, individuals were excluded if they had any codes denoting psychosis recorded in the MH-AMB dataset, or in secondary diagnosis fields in the APDC, but did not meet inclusion criteria for the psychotic SMI group (principal diagnosis of psychotic illness for any episode in the APDC).
The follow-up period started from the first date of discharge (index date) from hospital with a principal diagnosis of the above codes for each group and ended at the date of death for the individual or 31 December 2015, whichever occurred first. We restricted index hospital admissions to those where psychotic SMI or other non-psychotic SMI was recorded as a principal diagnosis to ensure that the follow-up period for every individual commenced following a hospital admission where a mental health disorder was the primary reason for inpatient treatment. Where an individual had separate hospital admissions for psychotic SMI and non-psychotic SMI, the follow-up period started from the first date of discharge for psychotic illness.
Outcome measures
The three outcome measures for this study were the rates of hospitalisation (mental and physical health), ED presentation and mental health ambulatory service utilisation. We calculated these rates by summing all hospital separations, ED presentations and mental health ambulatory treatment days in the follow-up period and dividing this amount by the total time in study. To calculate rates of ED presentation, we adjusted the person time by length of stay in hospital, as individuals could not have visited the ED while already admitted to hospital.
Statistical analysis
We used SAS 9.4 for data manipulation and STATA 15 for data analyses. Demographic data were summarised using descriptive statistics. Rates of health service utilisation per 1000 person-years were calculated for the whole study period after the index date. The impact of psychotic illness on rates of health service utilisation was assessed using Poisson regression after adjusting for demographic variables, comorbidity and previous health service utilisation (operationalised as the number of hospital admissions and ambulatory mental health service treatment days in the last 12 months). Variables with fixed values over the study period were sex, intellectual disability status (as per Reppermund et al., 2019), Aboriginal and/or Torres Strait Islander status, remoteness, Index of Relative Socioeconomic Disadvantage (IRSD) and length of stay for the index admission (categorised into under 7 days, between 7 and 29 days, and over 30 days). For remoteness and IRSD, we used information published by the Australian Bureau of Statistics. Charlson Comorbidity Index (CCI) was calculated from hospital episodes (Charlson et al., 1987; Quan et al., 2005, 2011) using multiple annual intervals for each individual, starting from the index date, ending at 1 year after the index admission and repeating this process annually until the end of the follow-up period. Age was included in the regression analysis as a time-dependent variable and was calculated at the beginning of each annual interval. We also included the non-linear effect of age in the model as it provided a better fit to the data.
Ethics approval
The study was approved by the NSW Population and Health Services Research Ethics Committee (HREC/13/CIPHS/7; Cancer Institute NSW reference: 2013/02/446 and Sub-study Reference number: 2019UMB0209). This approval included a waiver of informed consent.
Results
Cohort characteristics
Table 1 outlines demographic characteristics of the cohort. There were 189,790 individuals identified as having at least one mental health–related hospitalisation. Of these, 169,306 individuals met inclusion criteria for the study. Of the individuals who were excluded, 14,554 had their index admission after 31 December 2014, 2543 did not have required codes recorded, 3197 had invalid demographic information (either unspecified sex, negative age, an age listed under 12 or over 100 years, or missing remoteness or sociodemographic data) and 190 people died at the index admission. Of those in the included sample, 63,110 individuals were categorised into the psychotic SMI group (37.3%), and 106,196 were categorised into the non-psychotic SMI group (62.7%). Median age at the index admission for both groups was similar at 37.4 and 37.2 years, respectively. More than half (57.5%) of people with psychotic SMI were male, compared with 39.5% of people with non-psychotic SMI (Table 1). Notably, a greater proportion of index admissions within the psychotic SMI group were within psychiatric units (76.1% vs 44.6% for non-psychotic SMI), and median length of stay at the index admission for people with psychotic SMI was nearly three times that of those with non-psychotic SMI (11 days vs 4 days).
Cohort characteristics.
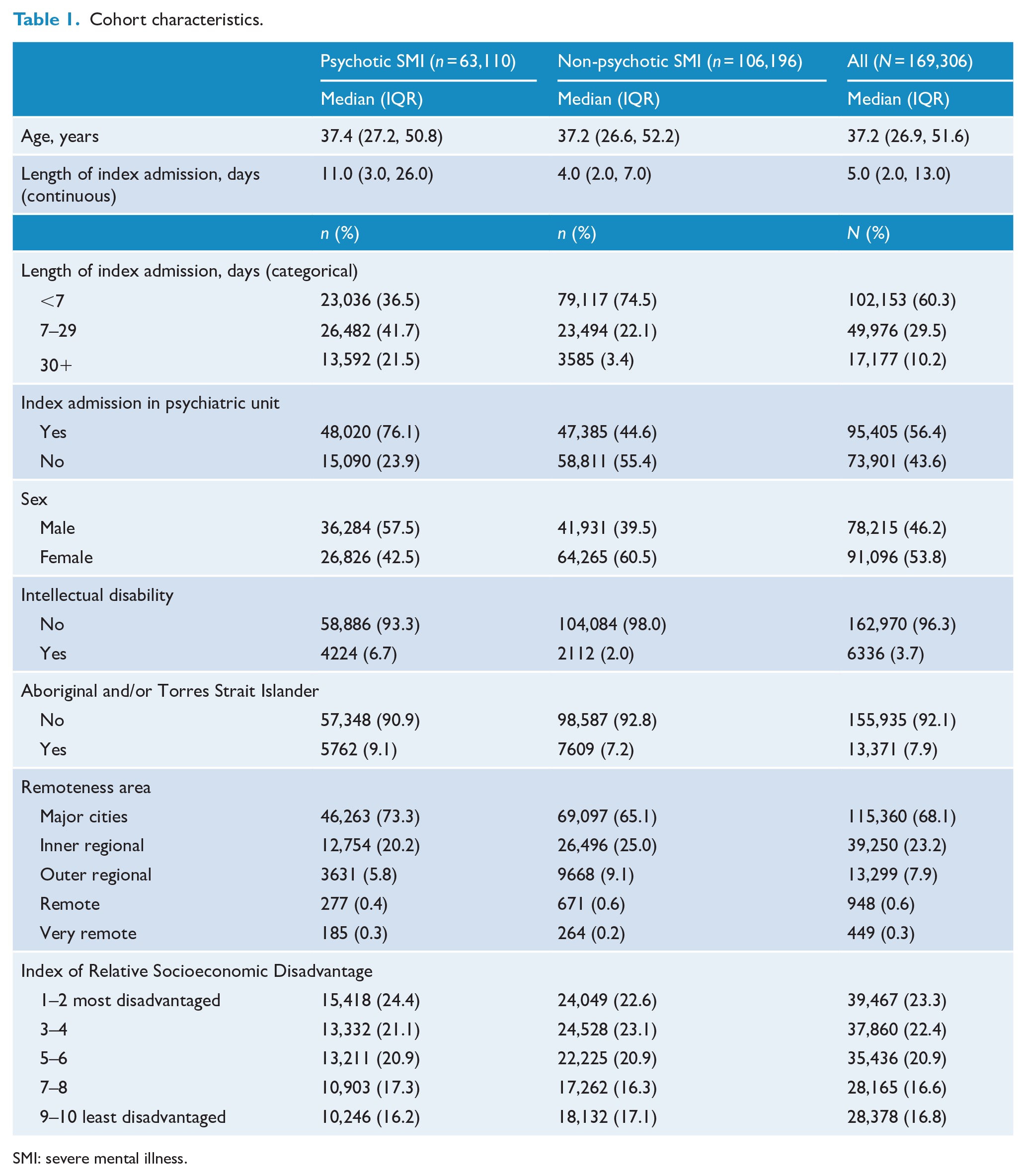
SMI: severe mental illness.
Rates of health utilisation
Following an index admission and until the end of the follow-up period, 51,015 (80.8%) people with psychotic SMI were admitted to hospital, 50,433 (79.9%) presented to an ED, and 52,682 (83.5%) accessed ambulatory mental health services. The proportions of people with non-psychotic SMI accessing services after an index admission and until the end of the follow-up period were 73,498 (69.2%), 82,256 (77.5%) and 58,834 (55.4%) for hospital, ED and ambulatory mental health services, respectively. Table 2 details rates of hospital separations, ED presentations and ambulatory mental health treatment days for each group. For people with psychotic SMI, rates of hospital separations, ED presentation and ambulatory mental health ambulatory treatment days were 920, 1204 and 12,857 per 1000 person years, respectively. Rates of hospital separations, ED presentation and ambulatory mental health treatment days for people with non-psychotic SMI were 750, 1205 and 2095 per 1000 person-years, respectively. Table 3 shows the rates of hospital separations by ICD chapters. As expected, the highest rate of hospital separations for the entire cohort was for mental disorders, followed by separations for dialysis, then injury and poisoning (Table 3).
Rates of health utilisation (per 1000 person-years).
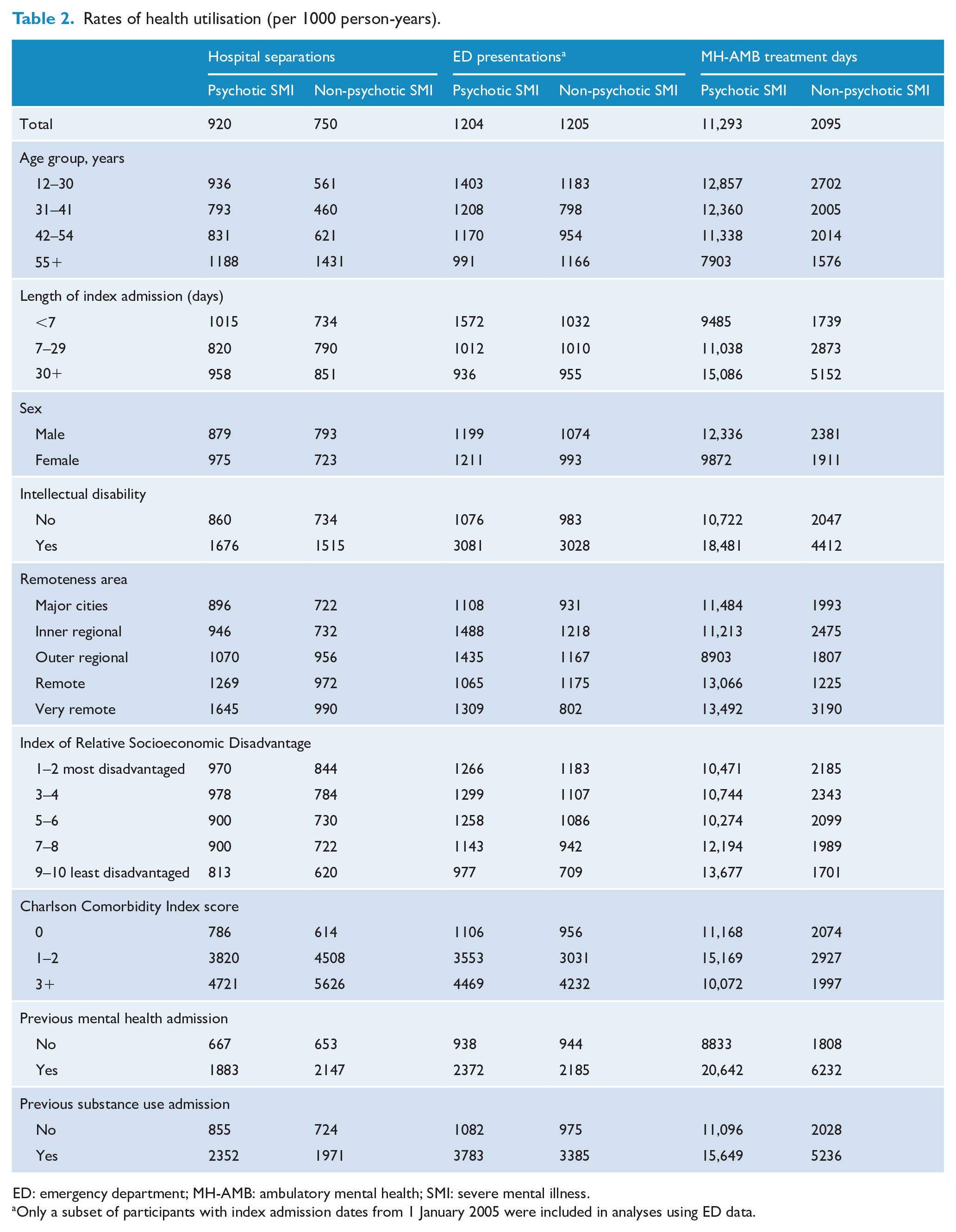
ED: emergency department; MH-AMB: ambulatory mental health; SMI: severe mental illness.
Only a subset of participants with index admission dates from 1 January 2005 were included in analyses using ED data.
Rates of hospital separations by ICD-10 chapters (per 1000 person-years).
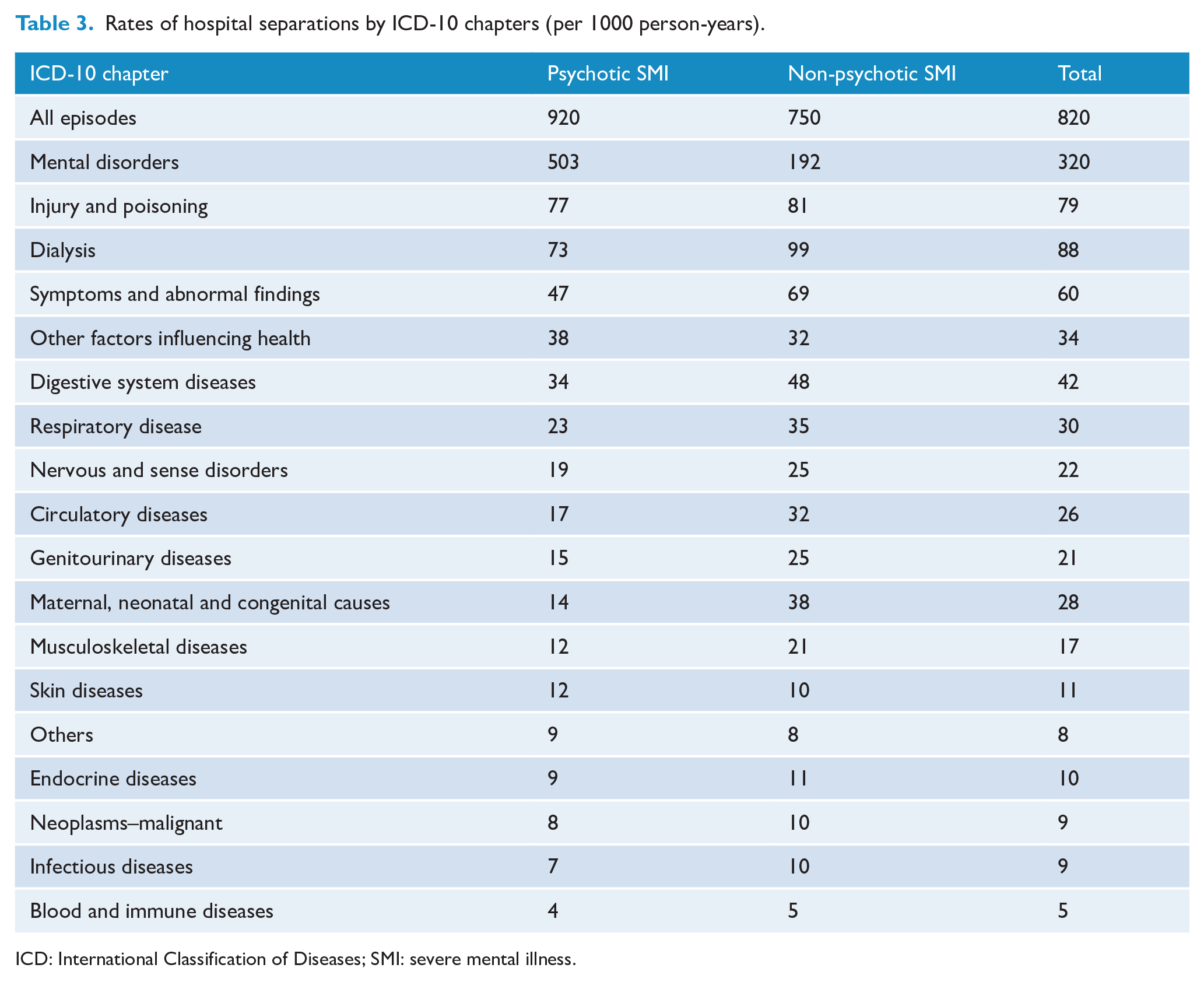
ICD: International Classification of Diseases; SMI: severe mental illness.
Factors associated with rates of health utilisation
A multivariable Poisson regression showed that people with psychotic SMI had, on average, higher rates of hospital separation (adjusted incidence rate ratio (IRR) 1.26; 95% confidence interval [CI] [1.23, 1.30]), ED presentation (adjusted IRR 1.17; 95% CI [1.13, 1.20]) and ambulatory mental health treatment days (adjusted IRR 2.90; 95% CI [2.82, 2.98]) than people with non-psychotic SMI. In addition to psychotic illness, factors that were independently associated with increased hospital separations, ED presentations and ambulatory mental health treatment days in the entire SMI cohort included intellectual disability, higher Charlson comorbidity score and previous hospitalisation within the last 12 months (Table 4).
Factors associated with health service utilisation.
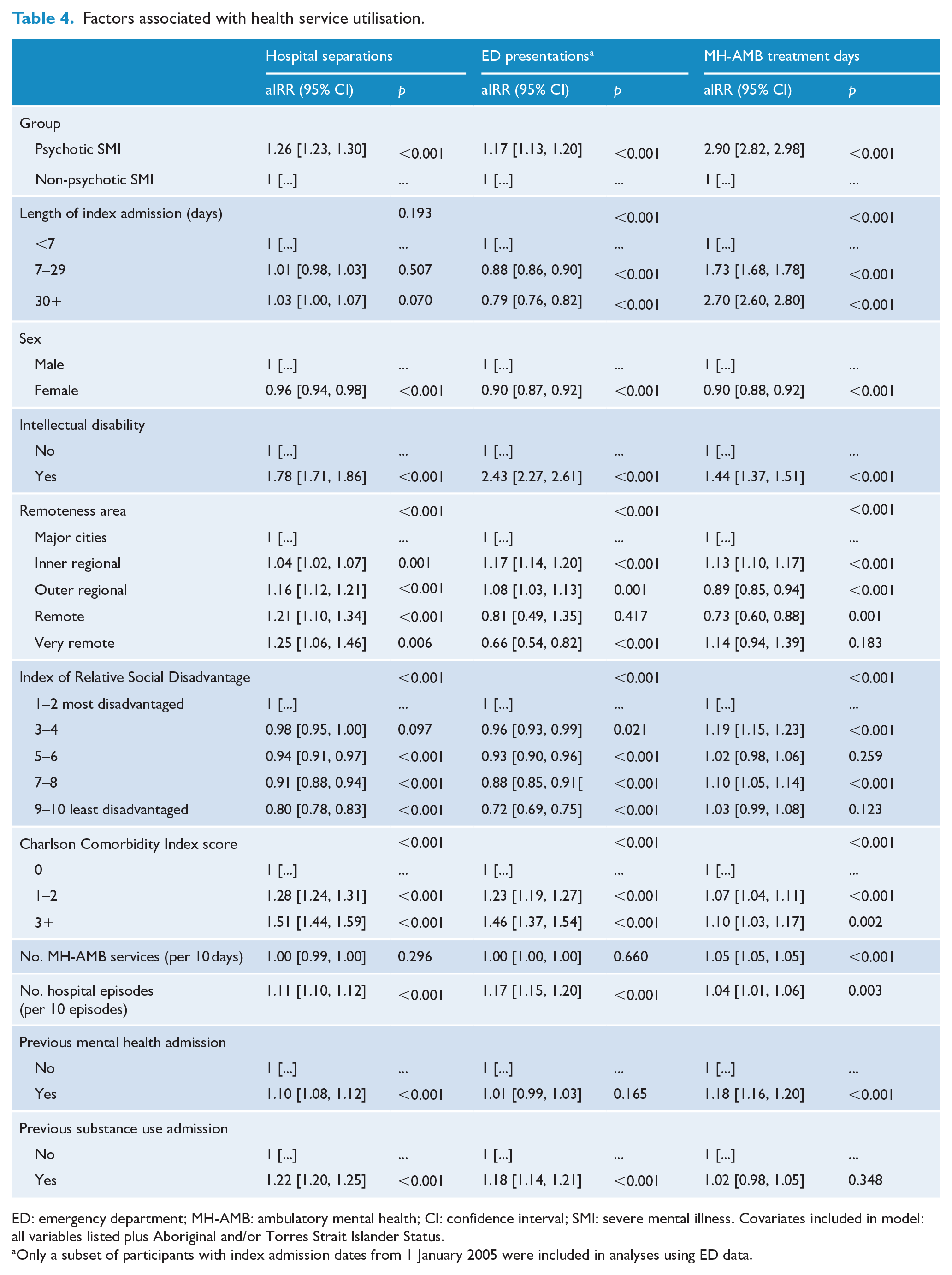
ED: emergency department; MH-AMB: ambulatory mental health; CI: confidence interval; SMI: severe mental illness. Covariates included in model: all variables listed plus Aboriginal and/or Torres Strait Islander Status.
Only a subset of participants with index admission dates from 1 January 2005 were included in analyses using ED data.
Discussion
In this study, we have used a large, population-based linked administrative dataset to describe and compare the health profiles and health service use of people with SMI, with and without psychotic illness. We found that people with psychotic SMI utilised all health services (hospital, ED and ambulatory mental health services) at higher rates than those with non-psychotic SMI. This difference was most striking for ambulatory mental health services, with individuals with psychotic SMI using this service at almost three times the rate of those with non-psychotic SMI after accounting for differences in available sociodemographic and other clinical characteristics. Despite the overall greater rate of hospitalisation among people with psychotic SMI, high rates of hospitalisation among those with non-psychotic SMI and relatively higher rates of hospitalisation for physical health problems in this group indicate that people with non-psychotic SMI also have a high need for acute health care services. The development or expansion of programmes to prevent and address physical health problems among people with SMI not limited to those with psychosis may mitigate the need for acute care and improve health outcomes in this group.
The higher rates of hospitalisation and ED use among people with psychotic SMI in the current study is consistent with previous research showing high rates of acute service use among people with psychotic disorders (AIHW, 2020; Morgan et al., 2011). Our findings build on this past research to show a higher rate of hospitalisation for people with psychotic SMI compared to non-psychotic SMI that appears to be driven by hospitalisations for the management of mental health disorders. While people with psychotic SMI had more than twice the rate of mental health admissions, people with non-psychotic SMI had higher rates of admission for the management of physical health problems such as circulatory, musculoskeletal, genitourinary and respiratory diseases. For the majority of mental disorders, it is unlikely that the findings are the result of differential health risks associated with the primary disorders, with the most obvious explanations relating instead to the nature of health care provision for these groups. Integrated care offered to people with psychotic disorders may better support physical health needs than those without, reducing the acute care presentations for chronic physical conditions. An alternative explanation is that diagnostic overshadowing contributes to poor identification and management of physical health disorders on presentation to hospital or ED (Thornicroft, 2011), or that physical health problems are managed during a mental health admission for people with psychotic disorders (this may contribute to the longer median length of the index hospital stay in this group). Finally, as index admissions of people with non-psychotic SMI were less likely to be within a psychiatric unit compared to people with psychotic SMI, it is possible that a substantial proportion of people with non-psychotic SMI in the current study were Consultation-Liaison patients with long-term medical conditions. Further research utilising primary care data including general practitioner visits and referrals is needed to determine the existence of a possible gap in access to community-based interventions for physical health problems for people with other types of SMI.
The most striking difference in health service use between groups was in ambulatory mental health treatment days. In the current study, people with psychotic SMI had almost three times the number of ambulatory mental health service treatment days compared to people with non-psychotic SMI. This is consistent with a previous report showing that schizophrenia as a principal diagnosis accounts for the largest proportion of contacts with community mental health care services in Australia (AIHW, 2020). There are multiple possible reasons for this finding. It is possible that the primary care and private sectors may be less equipped to effectively support people experiencing psychotic symptoms, increasing the need for mental health admissions and subsequent support from ambulatory mental health services. Second, our definition of SMI was based on a single hospital admission and thus did not take into account the long-term severity of the condition for the individual. It is possible that people with psychotic SMI experienced more severe illness for longer durations throughout the follow-up period and that this warranted their being more likely to be referred to or retained in ambulatory mental health services, while people with non-psychotic SMI included in the dataset may not have been referred to ambulatory mental health services if their condition was less complex and could be adequately managed by a different service, such as their general practitioner or private mental health professional. Third, it is possible that people with psychotic SMI may be more likely to be under an order of involuntary commitment and treatment and in these cases, attendance to ambulatory mental health services would have been required. Finally, people with psychotic SMI may be preferentially referred to ambulatory mental health services, and their limited availability, coupled with the historic focus on the needs of this group in public mental health services, may limit access to this resource for those with non-psychotic SMI. People with non-psychotic SMI may in fact form part of the ‘missing middle’ identified in the Victorian Royal Commission into Mental Health (State of Victoria, 2021); that is, people whose illness is considered too complex to be solely managed by primary care services, but not sufficiently severe to meet criteria for access to specialist mental health services. As health service utilisation is not a straight-forward reflection of health need, further efforts are needed to understand and address barriers to access to community mental health and early intervention services for people with all types of SMI, including those without psychosis.
Overall, the predictors of health service utilisation in the entire cohort support prior studies showing that people with complex needs (e.g. people with an intellectual disability and/or greater physical morbidity) access acute health services at a higher rate than those without (Li et al., 2018; Lunksy et al., 2012). Personal circumstances also had an impact on the rates of hospitalisation and ED visits; higher rates of hospitalisation in remote areas may reflect reduced access to non-hospital mental health services in those areas (AIHW, 2020; Meadows et al., 2015), while reduced rates of ED visits among people who were least disadvantaged (compared to most disadvantaged) may reflect the gap in access to community-based and private mental health support for people of lower socioeconomic status (Meadows et al., 2015). Longer hospital stay at the index admission, even when accounting for the presence of psychotic illness, was associated with a greater number of ambulatory mental health treatment days during the follow-up period, further supporting the notion that people with more complex support needs are prioritised for this service. It is unclear from our data whether individuals who did not access ambulatory mental health services required support from this service, received support elsewhere, or whether their need for further support remained unmet. Given the unrelenting demand on mental health services (State of Victoria, 2021), further research is needed to determine the characteristics of, and subsequent health service utilisation of high service users (including people with prolonged hospital stays) and people with complex needs to determine whether specific interventions or clinical pathways may reduce the need for acute care.
Collectively, the findings of this study have important implications for the development and implementation of mental health policy and service models to meet the health needs of people with all types of SMI. As expected, rates of all-cause hospitalisation for people with psychotic and non-psychotic SMI in the current study were more than twice that reported in the NSW general population (405 per 1000 population in 2014–2015) (AIHW, 2016). Overall, our findings reflect groups with high health care needs, and support the call for a greater focus on community-based care and development of a more responsive system with coordinated treatment and support for people with complex needs (Department of Health, 2017; NSW Ministry of Health, 2014, 2018). In particular, our findings highlight a need for greater support for people with SMI who have co-occurring intellectual disability, experience greater physical comorbidity, live in more remote areas or live in areas with greater relative socioeconomic disadvantage. Although our study did not include data from primary or private care services, our findings also highlight a possible need for the examination of ways to support physical health in people with non-psychotic SMI, which may include optimisation of primary and integrated care, as well as ensuring access to programmes designed to prevent and address physical health issues (Rosenbaum et al., 2014). One example is the Keeping the Body in Mind (Curtis et al., 2016, 2018), offered through the South Eastern Sydney Local Health District Mental Health Service in NSW. This early intervention lifestyle programme prevents weight gain and metabolic decline. A potential addition to the model of care for people with SMI is the provision of a general practice service within the ambulatory mental health service, as a proactive and early service to diminish the need for ED presentations for non-mental health issues. Finally, our findings point to a need for further research using large linked datasets (that include all components of health service use) and simulation to examine long-term health outcomes, service use and costs. This approach would enable the development and testing of new models of care to achieve better health outcomes for people with SMI which, based on our findings, would likely include an expansion of efforts and funding for community mental health services and integrated care.
Strengths of the current study include the whole of population capture of individuals admitted into hospital for the management of mental health problems in NSW, the most populous state in Australia, and the number of years available in the dataset (2001–2015). Limitations of our study include those inherent to the use of administrative datasets; these include possible erroneous and missing data (managed with strict inclusion criteria for the current study) and absence of information about a range of potential explanatory factors, including the duration of mental illness, mental health act status, risk assessment issues and impact on everyday functioning. As our definition of SMI was based on the requirement of hospitalisation for the management of a mental health disorder, our findings are not generalisable to all people with SMI, many of whom are not receiving inpatient treatment. This would impact our findings related to ambulatory mental health service utilisation, particularly if people with psychotic SMI are more likely to have been hospitalised than people with non-psychotic SMI (i.e. there may be a greater number of people with non-psychotic SMI utilising ambulatory mental health services without a previous hospital admission who did not meet inclusion criteria for the cohort). Notwithstanding this limitation, our findings do still indicate that following a mental health–related hospital admission, the rate of ambulatory mental health service use is higher among people with psychotic SMI than people with non-psychotic SMI. Another limitation relates to our findings about ED use as not all EDs participate in the EDDC. While this could potentially bias our findings, it is important to note that the larger public EDs participate in the EDDC, and so a substantial proportion of the NSW population has been covered. A final limitation of our study relates to the lack of information about utilisation of primary care and other mental health services, including general practitioners, private psychologists and private psychiatrists. Further research is needed to determine the impact of access to these services on acute and ambulatory mental health services among people with SMI.
Although people with psychotic SMI have been recognised to have high health needs, this study supports the need to also focus on people with non-psychotic SMI who also have high health needs that require acute care. Efforts to develop more coordinated treatment and supports and improve physical health for people with SMI should include a focus on non-psychotic SMI as well as on people with complex support needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Health and Medical Research Council Australia (Partnerships for Better Health APP1056128) and the UNSW Medicine Neuroscience, Mental Health and Addictions Theme and SPHERE Mindgardens Clinical Academic Group.