
Abstract
Objective:
People experiencing severe mental illness report higher rates of tobacco smoking than the general population, while rates of quitting and sustaining abstinence are considerably lower. This systematic review aimed to identify factors associated with sustained abstinence in people experiencing severe mental illness following a smoking intervention.
Method:
Searches were conducted in PubMed, PsycInfo, Scopus, Embase, Emcare, CINAHL and Cochrane Library from the inception of the e-databases until June 2022. Selection criteria included randomised and non-randomised studies of smoking cessation interventions in which most of the participants were experiencing severe mental illness, and reported a follow-up of 3 months or longer. From an initial 1498 unique retrieved records, 26 references were included detailing 17 smoking cessation intervention studies and 3 relapse prevention intervention studies. Risk of bias was assessed using the RoB2 tool for randomised study designs and the ROBINS-I tool for non-randomised designs.
Results:
Participation in smoking interventions was associated with higher odds of abstinence in the medium-term, but not long-term follow-ups. There was insufficient evidence that any other factors impact sustained abstinence. Most studies were considered to have some risk of bias, largely due to insufficient availability of analysis plans.
Conclusion:
Despite an abundance of studies investigating smoking cessation in smokers experiencing severe mental illness, there is limited knowledge on the factors associated with staying quit. The inclusion of people experiencing severe mental illness in large-scale randomised control trials, in which predictors of sustained abstinence are measured in the medium and long term are needed to address this important question.
Introduction
People experiencing severe mental illness (SMI), such as schizophrenia or bipolar disorder, face a reduced life expectancy of approximately 10–15 years compared to the general population (Hjorthøj et al., 2017). This is largely explained by cardiometabolic and respiratory diseases to which smoking is a significant contributor (Brown et al., 2010). Around two-thirds of people experiencing SMI in high-income countries smoke tobacco, a rate much higher than the general population (Dickerson et al., 2018; Lawrence et al., 2009). While smoking rates in high-income countries internationally have declined over recent years in the general population, the reduction in smoking rates has been much slower in people experiencing SMI (Greenhalgh et al., 2022). People experiencing SMI smoke more heavily, consume more nicotine from each cigarette and report greater nicotine dependence (Bowden et al., 2011; McClave et al., 2010; Williams et al., 2005).
Many people experiencing SMI who smoke are motivated to quit and willing to seek quit support (Aschbrenner et al., 2015; Lappin et al., 2018). Cessation attempts are less likely to be successful, however, and relapse rates are higher for people experiencing SMI (Evins et al., 2014; McClave et al., 2010). Why this is the case is not well understood. It may in part be due to the greater barriers in accessing appropriate interventions faced by people experiencing SMI (Lum et al., 2018). Some of these barriers arise from the design and effectiveness of smoking interventions, which may not adequately meet the specific needs of people experiencing SMI who are making a cessation attempt. Moreover, the exclusion of people experiencing SMI from many large randomised control trials (RCTs) investigating the safety and efficacy of pharmacological smoking treatments means that the evidence for their use in this population is limited (Talukder et al., 2021).
Barriers due to personal circumstances (e.g. low socioeconomic status, lack of family and peer support, co-morbid physical health problems) are more prevalent in people experiencing SMI (Sweeney et al., 2015). Additional barriers include commonly held misconceptions around the benefits of smoking in managing symptoms associated with mental illness, such as smoking reduces stress (Morisano et al., 2013; Strand and Nybäck, 2005), and that smoking cessation may worsen mental health symptoms, despite good evidence for the converse being true (Taylor et al., 2021).
Tailored cessation interventions for people experiencing SMI include the Smoking Cessation Intervention for Severe Mental Illness (SCIMITAR+) study (Gilbody et al., 2019). This large RCT, conducted in the United Kingdom, found that people with SMI who received the bespoke intervention had 2.4 times greater odds of quitting smoking and remaining abstinent at 6 months follow-up compared to the treatment as usual group. Some caveats should be noted, however, including first, that intention-to-treat analysis was not used as typically reported in smoking trials, and second, at 12 months the effect was not significant. This suggests that more research is needed to identify how sustained abstinence and longer-term abstinence can be supported in people experiencing SMI.
Prior studies have measured the effectiveness of different pharmacological aids on both cessation and relapse prevention in people experiencing SMI. Varenicline and bupropion have each been found to increase the likelihood of cessation in people experiencing SMI, with neither having a detrimental effect on psychiatric symptoms (Tidey and Miller, 2015; Tsoi et al., 2013). EAGLES, a large RCT comparing individuals experiencing mental illness to a sample without mental illness provided further support for the efficacy and safety of these pharmacological aids, though the sample predominantly consisted of individuals experiencing affective disorders and the proportion of participants included with a psychotic disorder was limited (Anthenelli et al., 2016).
Despite the numerous studies trialling cessation treatments for people experiencing SMI, to date, little is known about the specific factors that contribute to sustained abstinence in people experiencing SMI. Given the additional challenges that people with SMI experience in quitting smoking, maintaining abstinence is of high importance. This review seeks to address this gap by assessing the current evidence for associations of sustained abstinence in people experiencing SMI. Elucidating the factors that aid in successful abstinence may help in both the development and planning of appropriate interventions and in identifying individuals who may need targeted support to prevent relapse.
Aim
To identify factors that are associated with sustained smoking abstinence in people experiencing SMI after participation in a smoking intervention.
Methods
Design
The systematic review examined all original research studies that measured sustained abstinence in people experiencing SMI after participation in a smoking intervention. The review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement and was pre-registered on PROSPERO (CRD42020168279).
Criteria for inclusion in the review
Studies
Original peer-reviewed randomised and non-randomised studies, including single-arm studies, that examined factors associated with successful smoking abstinence in people experiencing SMI after participation in a smoking intervention were included. Grey literature, editorials, theses, conference abstracts and articles not published in English were not included. Reviews were not included but were checked for additional references. Secondary references that reported on the same dataset as a primary reference (for instance, an additional follow-up time point) were included and acknowledged in the data tables.
Intervention
Studies were included that described an intervention to assist participants to cease tobacco smoking, and that had a minimum follow-up period of 3 months following the completion of the intervention. These included both behavioural and pharmacological interventions, or a combination. Studies that included enforced smoking cessation (e.g. upon hospital admission) were not included if (1) the intervention was not optional or (2) no pharmacological or behavioural support was provided upon discharge. Observational studies of individuals completing interventions not delivered by the research team (e.g. national smoking helplines and quit programmes) could be included. Studies investigating the use of e-cigarettes were not included, as globally there is currently limited evidence on effectiveness and safety, and they are currently only licenced for smoking cessation in a limited number of countries.
Relapse prevention trials were included if the preceding smoking intervention was described in sufficient detail to allow the relevant outcomes to be extracted from the data.
Participants
Eligible studies included those with participants aged 18 years or older who had experienced SMI. SMI was defined as meeting the criteria for a clinical diagnosis of schizophrenia, schizoaffective disorder, bipolar disorder or other psychotic disorder. Studies were also included if participants were recorded as experiencing an SMI without further detail on the diagnosis being provided. If so, this was recorded in the data extraction.
Studies with mixed-diagnosis samples (e.g. people experiencing different mental illnesses, or in which people experiencing mental illness were a subgroup of the general population) were included if 75% of the sample or greater reported SMI, or if the relevant outcomes could be extracted from the data for the SMI sample separately.
Outcomes
Primary outcomes
Primary outcomes were any factors associated with sustained smoking abstinence in people experiencing SMI. All factors identified were documented and grouped as characteristics of the cessation programme (e.g. type of treatment, attendance), socio-demographic characteristics, clinical characteristics (e.g. symptoms related to mental illness or psychiatric medication) and smoking history.
The measure of abstinence at the latest follow-up was used as the time point to identify factors associated. Where more than one measure of abstinence was provided (i.e. point-prevalence and continuous abstinence), the association with each was reported. All available abstinence outcomes were recorded when describing the characteristics of studies.
Secondary outcome
A secondary outcome was the identification of factors associated with smoking relapse. Relapse was defined as a return to regular smoking. The measures used by each study to establish relapse were recorded.
Search strategy and study selection
Searches were conducted using PubMed, PsycInfo, Scopus, Embase, Emcare, CINAHL and Cochrane Library from the inception of the e-databases until June 2022. Search terms included ‘smoking cessation’, ‘severe mental illnesses’, ‘smoking relapse’ and their synonyms. The full search strategy is included in Appendix 1 of Supplemental material. Two authors (K.D. and M.S-M.) undertook screening of titles and abstracts independently. The full-text screening was completed by the same two authors and disagreements were discussed and settled with a third (J.M.L.) and fourth (R.J.C.) author.
Data extraction
Two authors (K.D. and M.S-M.) independently extracted the data into a standardised data extraction table. Any discrepancies were settled by a third reviewer (J.M.L.). Variables extracted are shown in Table 1.
Variables extracted from included studies.
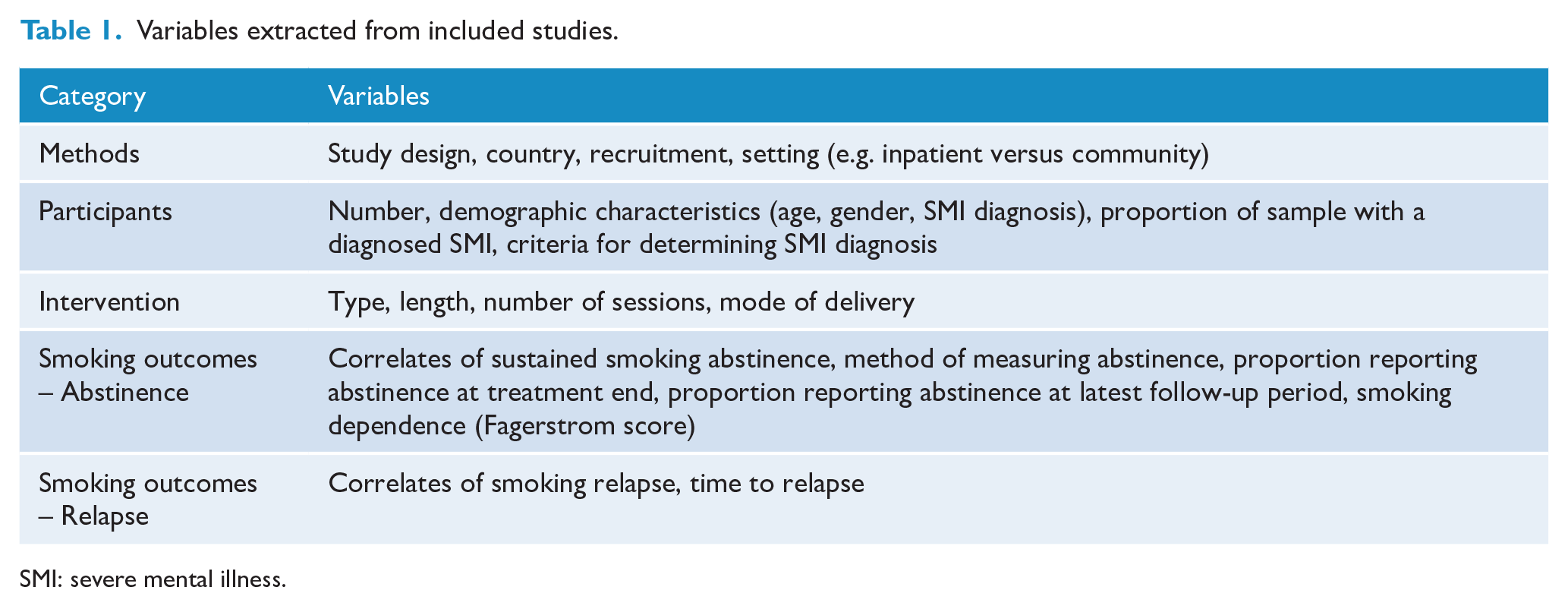
SMI: severe mental illness.
Assessment of risk of bias
For references that reported on the same study but contributed data for different time points, risk of bias assessments were conducted, and reported, per reference. This approach was used to account for the potential difference in methods of data collection and measurement of abstinence at each time point. Where more than one reference referred to the same study and provided data for the same time point (i.e. different analyses of associations), risk of bias assessments were conducted for the primary reference for that study and encompassed all available information from the combined references.
References in which the studies utilised a randomised study design were assessed for risk of bias using version 2 of the Cochrane ‘Risk of Bias’ tool (RoB2; Bucklin, 2021). Each study was assessed on the following five domains: (1) risk of bias arising from the randomisation process, (2) risk of bias due to deviations from the intended interventions (effect of assignment to intervention), (3) risk of bias due to missing outcome data, (4) risk of bias in measurement of the outcome, and (5) risk of bias in selection of the reported result. Where no data analysis plan was publicly available, neither via publication nor via trial registration, domain 5 was coded as ‘no information’ resulting in a ‘some concerns’ outcome.
References of non-randomised study designs were assessed using the ROBINS-I tool (Sterne et al., 2016). This tool assesses bias across seven domains: (1) bias due to confounding, (2) bias in selection of participants, (3) bias in classification of interventions, (4) bias due to deviations from intended intervention, (5) bias due to missing data, (6) bias in measurement of outcomes, and (7) bias in selection of the reported result.
Assessments were completed by two authors (K.D. and R.M.). Consensus judgements for each domain and overall are presented.
Data synthesis and analysis
Data on factors related to sustained abstinence following participation in a smoking cessation or relapse prevention intervention were synthesised following the Cochrane guidance for appropriate synthesis without meta-analysis (McKenzie and Brennan, 2022). Effect estimates are summarised using descriptive statistics, from which odds ratios (ORs) were calculated to provide a standardised metric where the data available permitted. Where possible, median OR and ranges are reported for each factor assessed for a relationship with sustained abstinence. Given that measurement method and duration of follow-up have been found to affect estimates of abstinence (West et al., 2005), and the different lengths of follow-up and measurement used to assess abstinence reported by references included in this review, the results are presented separately for short-term (<6 months), medium-term (6–12 months) and long-term follow-ups (>12 months), and for point-prevalence versus continuous measures of abstinence. Smoking relapse prevention trials are denoted in the tables.
Meta-analysis of the effect of intervention on sustained abstinence
Meta-analysis examining the effect of receiving any intervention versus no intervention was used to estimate the overall difference in odds of smoking abstinence. As studies reported abstinence using different metrics, both a point-prevalence meta-analysis and a continuous abstinence meta-analysis were completed.
We had planned to conduct subgroup analyses to examine the effects of different intervention types (e.g. behavioural interventions, pharmacological interventions), however, were unable to do so due to the heterogeneity within therapy types. For instance, the behavioural interventions encompassed a variety of approaches and were often provided in conjunction with different pharmacological aids, meaning that the effects of each could not be separated.
A random effects model was used to estimate odds of abstinence, overall, and for subgroups of less than 6 months, 6–12 months and more than 12 months follow-up time.
Heterogeneity of effects was examined. Possible publication bias was assessed by funnel plots, Egger’s test, trim and fill. The overall effect size was re-estimated to account for possible bias (Henmi & Copas, 2010). Analyses were performed using the package ‘metafor’ in ‘R’.
Results
After the removal of duplicates, a total of 1498 results were identified to be screened. Of these, 26 references met the inclusion criteria. As six of the studies provided additional follow-up data to four studies already included, a total of 20 studies were included in the final sample (Figure 1).
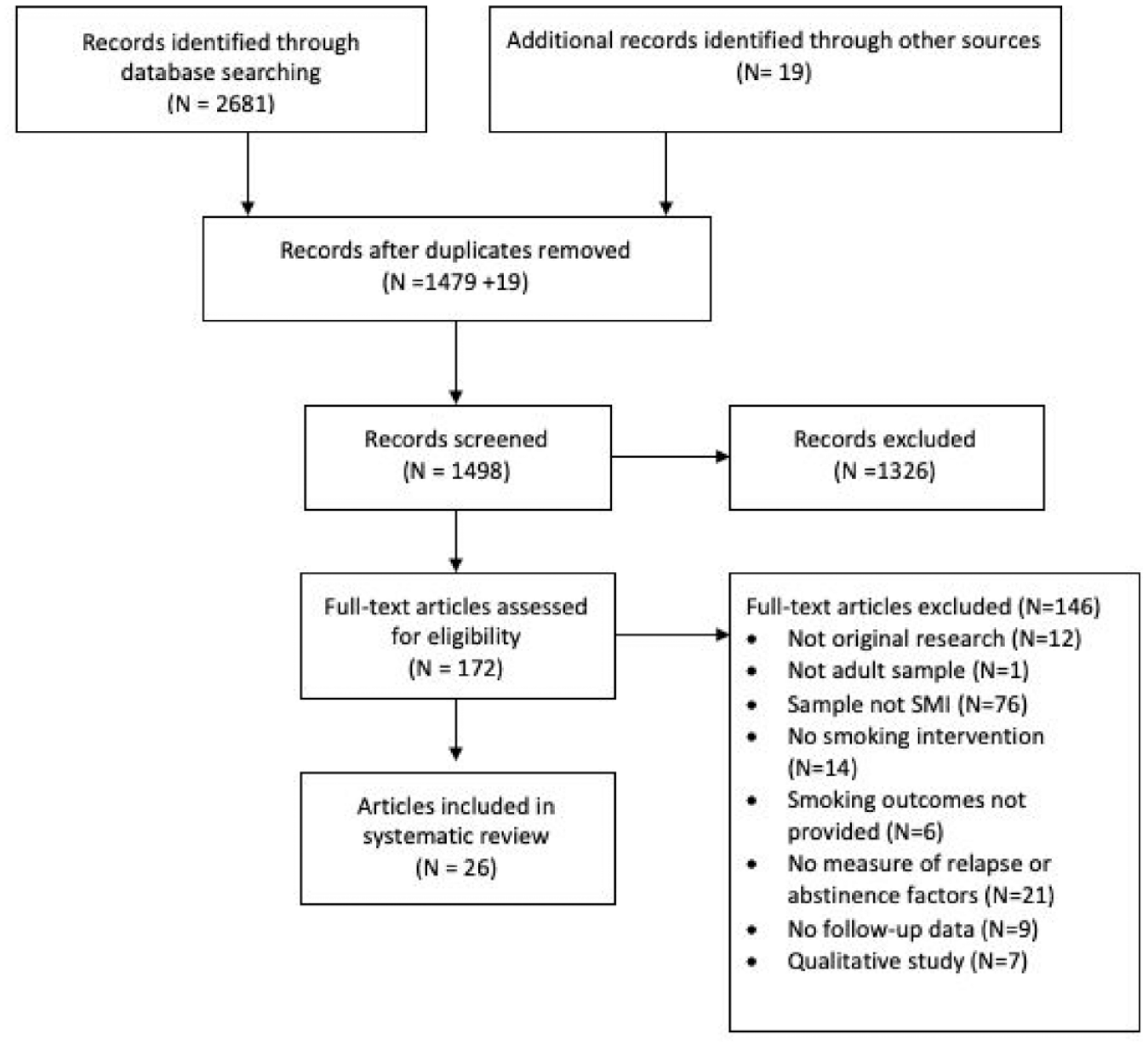
Study inclusion flow diagram based on PRISMA guidelines.
Summary of study characteristics
The majority of studies included were randomised controlled trials. Three non-randomised trials were included (Addington et al., 1998; Cather et al., 2013; Garcia-Portilla et al., 2016) as shown in Table 2. Three studies (four references) consisted of a cessation intervention phase followed by a relapse prevention phase (Cather et al., 2013; Evins et al., 2014; Horst et al., 2005; Thorndike et al., 2016). All but two studies included a control condition (Addington et al., 1998; Cather et al., 2013), typically a pharmacological placebo. All studies were conducted in high-income countries.
Characteristics of studies.
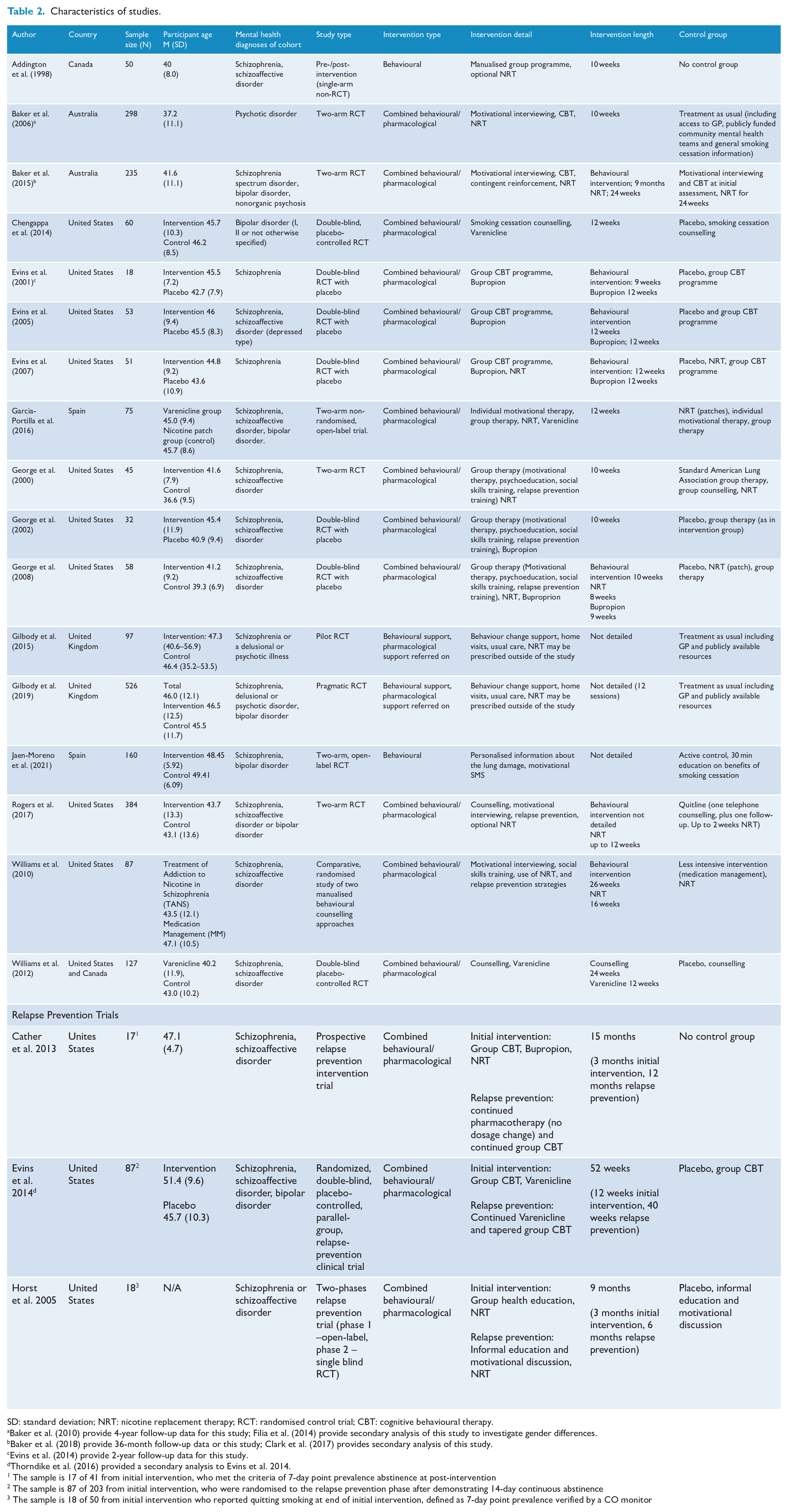
SD: standard deviation; NRT: nicotine replacement therapy; RCT: randomised control trial; CBT: cognitive behavioural therapy.
Baker et al. (2010) provide 4-year follow-up data for this study; Filia et al. (2014) provide secondary analysis of this study to investigate gender differences.
Baker et al. (2018) provide 36-month follow-up data or this study; Clark et al. (2017) provides secondary analysis of this study.
Evins et al. (2014) provide 2-year follow-up data for this study.
Thorndike et al. (2016) provided a secondary analysis to Evins et al. 2014.
The sample is 17 of 41 from initial intervention, who met the criteria of 7-day point prevalence abstinence at post-intervention
The sample is 87 of 203 from initial intervention, who were randomised to the relapse prevention phase after demonstrating 14-day continuous abstinence
The sample is 18 of 50 from initial intervention who reported quitting smoking at end of initial intervention, defined as 7-day point prevalence verified by a CO monitor
Participant characteristics
All studies included samples in which all participants had a diagnosis of SMI (Table 2). Half of the studies recruited from mental health or health services, while other methods included via primary care, media campaigns, research registers and self-referral.
Intervention characteristics
The majority of study interventions provided a combination of pharmacological treatment alongside psychosocial approaches (Table 3). Psychosocial approaches included group cognitive behavioural therapy (CBT) programmes (n = 5; Cather et al., 2013; Evins et al., 2001, 2005, 2007, 2014), individual CBT programmes (n = 2; Baker et al., 2006, 2015), motivational interviewing (n = 8; Baker et al., 2006, 2015; Garcia-Portilla et al., 2016; George et al., 2000, 2002, 2008; Rogers et al., 2017; Williams et al., 2010), smoking cessation counselling (n = 3; Chengappa et al., 2014; Rogers et al., 2017; Williams et al., 2012) and education programmes including relapse prevention (n = 6; George et al., 2000, 2002, 2008; Horst et al., 2005; Jaen-Moreno et al., 2021; Williams et al., 2010). Other approaches included contingent reinforcement (Baker et al., 2015) and existing group programmes adapted for people experiencing SMI (Addington et al., 1998; Gilbody et al., 2015, 2019). The majority of interventions included more than one approach.
Smoking intervention types.
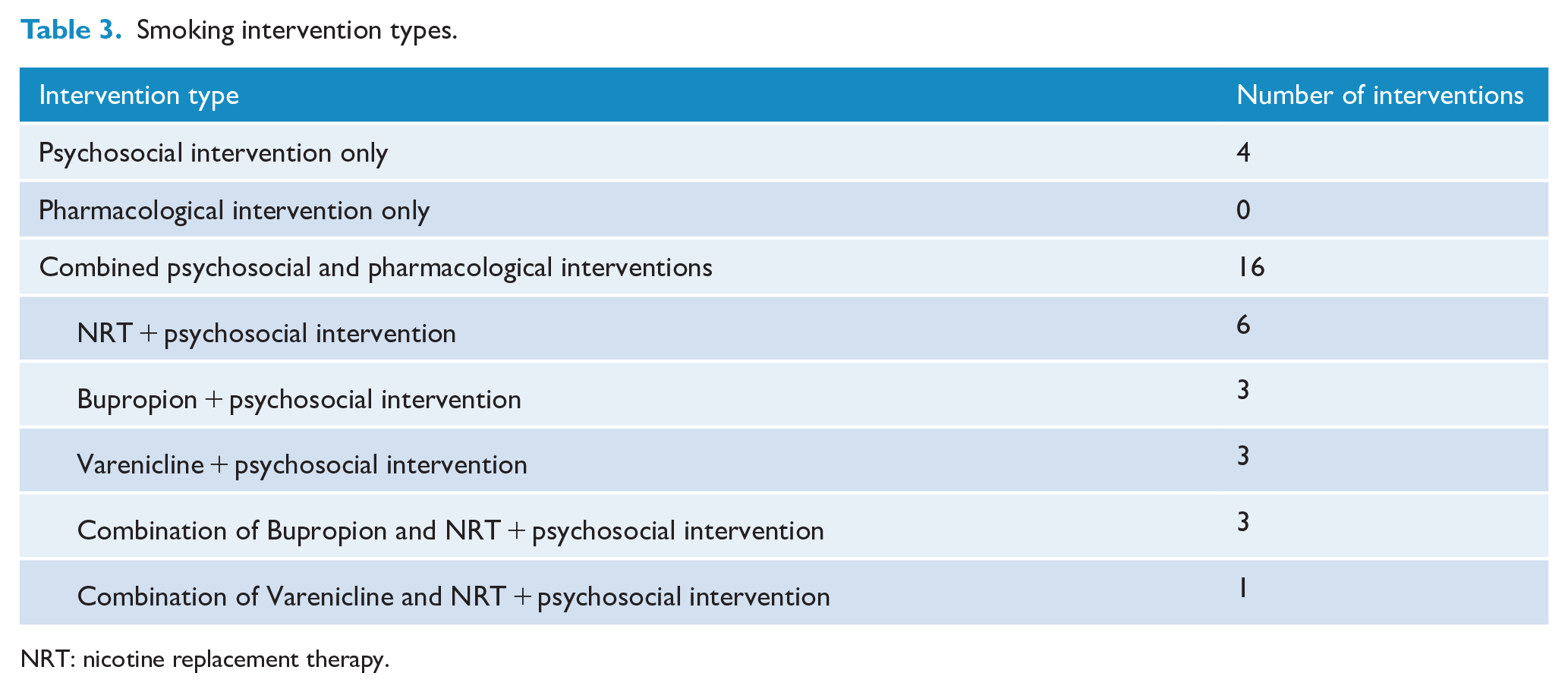
NRT: nicotine replacement therapy.
Smoking outcomes characteristics
Rates of smoking abstinence
Abstinence at the end of smoking cessation interventions ranged between 11.0% and 50.0% (n = 12) when assessed via point-prevalence, and between 10.9% and 37.5% (n = 9) when continuous abstinence was measured. Sustained abstinence assessed via point-prevalence at the latest follow-up ranged between 6.6% and 45.0% (n = 15), and when assessed via continuous abstinence ranged between 5.4% and 19.0% at 6 months, and 3.9% and 14.3% at 12 months. Abstinence following relapse prevention trials ranged between 45.0% and 64.7% (n = 1) when measured via point-prevalence, and between 45.0% and 77.6% (n = 3) when assessed via continuous abstinence at 12 months of relapse prevention (Table 4). Further information on the measurement of abstinence in the included references is available in Supplementary 1.
Smoking outcomes.
SD: standard deviation; ppm: parts per million; CA: continuous abstinence; TANS: treatment of addiction to nicotine in schizophrenia; MM: medication management.
Relapse to smoking
Relapse rates were explicitly reported in four studies (Chengappa et al., 2014; Evins et al., 2014; Garcia-Portilla et al., 2016; Horst et al., 2005), and two reported time to relapse (Evins et al., 2014; Williams et al., 2010). Only one study examined factors associated with relapse (Horst et al., 2005) (Table 4).
Factors associated with abstinence
Intervention-related characteristics
Treatment condition was the factor most commonly measured as a correlate of sustained smoking abstinence: examined by 21 of the included references. This included one study with a follow-up of less than 6 months (Evins et al., 2005) assessed to be at moderate risk of bias (i.e. some concerns), with a standardised OR of 1.13, (95% confidence interval [CI] = [0.07, 18.98]) which was not significant.
Fourteen references with a 6- to 12-month follow-up examined the association with abstinence using point-prevalence measures. The median OR of sustained abstinence was 1.97 (range: 0.49–10.42) for interventions versus control conditions, and three references reported a significant association (Evins et al., 2014; George et al., 2000; Horst et al., 2005). Of these, two were considered at moderate risk of bias and one at high risk. Two were relapse prevention trials. Four references with a 6- to 12-month follow-up examined the association with abstinence using continuous abstinence measures. The median OR of sustained abstinence was 2.48 (range: 0.92–5.28) for intervention compared to control conditions. None reported a significant association. All were considered at moderate risk of bias.
In references with a follow-up longer than 12 months, three examined the association using point-prevalence measures of abstinence. The median OR of sustained abstinence was 1.0 (range: 0.70–1.36) for interventions compared to control conditions and none reported a significant association. One was at low risk of bias, one at moderate risk and one at high risk. Two references examined the association using continuous abstinence measures. One did not provide data beyond a non-significant report (Baker et al., 2010). One was significant in favour of the intervention (OR = 3.4, 95% CI = [1.02, 13.6]) and was a relapse prevention trial (Evins et al., 2014). Both were assessed at moderate risk of bias.
One reference examined the association between participant-rated therapeutic relationship and sustained smoking abstinence (Williams et al., 2010). This study, considered at moderate risk of bias, used continuous abstinence measures at a 3-month follow-up and reported a significant relationship (p = 0.03) in favour of higher ratings.
Programme attendance during intervention was measured by seven references. Four with a 6- to 12-month follow-up examined the association with abstinence using point-prevalence measures. The median OR of sustained abstinence was 2.17 (range: 1.04–3.22) for higher compared to lower attendance and two reported a significant association (Addington et al., 1998; Baker et al., 2006). Of these, one was considered at moderate risk of bias and one at high risk. Three references examined the association with abstinence using continuous abstinence measures, two were considered at moderate risk of bias and one high risk. A median OR could not be calculated due to lack of suitable data, and one reference reported a significant relationship in the direction of higher attendance. Only one reference examined the association at a follow-up greater than 12 months and was considered at moderate risk of bias. This reference did not report a significant relationship.
Participant characteristics
Three references examined gender as a factor associated with sustained abstinence at 6–12 months, one was assessed at low risk of bias and two at moderate risk. For references using point-prevalence measures, the median OR of abstinence was 2.02 (range: 1.33–4.57) for female participants compared to male. One reference reported a significant effect (Clark et al., 2017), with females over 4.5 times more likely to remain abstinent at 12-month follow-up. When assessing the association using continuous abstinence measures, the standardised OR for abstinence was non-significant at 1.10. One reference examined gender with a follow-up greater than 12 months using both point-prevalence and continuous abstinence measures and did not report a significant relationship or provide data beyond significance.
Two references assessed the association between age and sustained abstinence at 6- to 12-month follow-up, both using point-prevalence measures of abstinence. One reference was considered at low risk of bias, and one at moderate risk. The median OR for sustained abstinence was 1.84 (range: 1.0–2.64) for older age. One reference reported a significant association (Thorndike et al., 2016). One reference examined age with a follow-up greater than 12 months using both point-prevalence and continuous abstinence measures and did not report a significant relationship or provide data beyond significance.
Clinical characteristics
Six references compared the use of typical and atypical antipsychotic medication as a factor associated with sustained abstinence. One reference, assessed as at moderate risk of bias, used point-prevalence measures of abstinence at 3-month follow-up and found no significant relationship. Three references examined the relationship at a 6- to 12-month follow-up, all using point-prevalence measures of abstinence. One reference was considered at moderate risk of bias and two at high risk. The median OR for sustained abstinence was 1.77 (range: 1.04–2.55) for atypical compared to typical antipsychotic medication, and one reference reported a significant relationship (George et al., 2000). Two references examined the association with sustained abstinence at a follow-up greater than 12 months, one used point-prevalence measures of abstinence and one used both point-prevalence and continuous abstinence measures. Neither reported a significant relationship or provided data beyond significance. Of these, one was assessed as moderate risk of bias and one at high risk.
The relationship between psychiatric diagnosis and sustained abstinence was examined in four references. Three references assessed the relationship at a 6- to 12-month follow-up, and all used point-prevalence measures of abstinence. The median OR for sustained abstinence was 1.45 (range: 0.86–1.85) for schizophrenia and schizoaffective disorder diagnoses compared to other psychotic disorders and none reported a significant association. One reference was considered at low risk of bias, one at moderate risk and one at high risk. One reference examined the relationship between diagnosis and sustained abstinence at a follow-up greater than 12 months, using both point-prevalence and continuous measures of abstinence. This reference was considered at moderate risk of bias and did not report a significant relationship.
Two references looked at the association between psychosis symptoms and sustained abstinence, one with a follow-up at 6–12 months, and one with a follow-up greater than 12 months. Both used point-prevalence measures of abstinence and neither reported a significant relationship.
The association between physical health variables and sustained abstinence was measured only at 6–12 months and by one reference (Thorndike et al., 2016). A significant association with sustained abstinence was reported for hyperlipidaemia (Mdn = −4.9 vs Mdn = −1.0), with a greater number of those in the sustained abstinence group reporting hyperlipidaemia at baseline. Remaining abstinent was also found to be significantly associated with reduced cardiovascular disease risk and an increase in weight; however, these were likely to be outcomes from the intervention rather than predictors. The reference was considered at moderate risk of bias.
Two references examined the relationship between functioning and sustained abstinence. One examined the relationship at a 6- to 12-month follow-up using point-prevalence measures of abstinence, and one at a follow-up greater than 12 months using both point-prevalence and continuous abstinence measures. Neither reported a significant relationship.
The relationship between substance use and sustained abstinence was assessed by one reference at a follow-up greater than 12 months using both point-prevalence and continuous measures of abstinence. The reference was considered at moderate risk of bias and did not report a significant effect.
Smoking history
Four references examined the relationship between baseline smoking characteristics (e.g. heaviness of smoking, nicotine dependency, number of daily cigarettes) and sustained abstinence. Two references looked at the relationship at a 6- to 12-month follow-up using point-prevalence measures of abstinence. One was considered at low risk of bias and one at moderate risk. Neither reference reported a significant association for any of the variables.
Two references examined the association between baseline smoking factors and sustained abstinence at a follow-up greater than 12 months. One reference examined the association of five different variables with sustained abstinence using point-prevalence and continuous abstinence measures and reported no significant relationships. The reference did not provide any data beyond significance and was considered at moderate risk of bias. One reference, assessed as high risk of bias, reported a significant association between smoking reduction in a previous trial and sustained abstinence at a 2-year follow-up using point-prevalence measures (Evins et al., 2004).
Factors associated with relapse
Only one study looked at factors associated with relapse to smoking (Horst et al., 2005), reporting that the group assigned to nicotine replacement therapy (NRT) were significantly less likely to relapse into smoking than the placebo group (33.3% vs 100%). No other factors were examined.
Risk of bias in included studies
Risk of bias assessments are summarised in Tables 5 and 6. Twenty references (reporting on 17 RCT studies) were evaluated for risk of bias using the RoB 2.0 tool. Three references reporting on non-RCT studies (Addington et al., 1998; Cather et al., 2013; Garcia-Portilla et al., 2016) were evaluated using the ROBINS-I tool (Sterne et al., 2016). For those references assessed using the RoB 2.0 tool (Table 5), the majority of studies were assessed as ‘some concerns’. Four references were considered low risk across all domains, and three references had at least one domain rated as high risk. The predominant reason for assessments noted as ‘some concerns’ was lack of available analysis plan. One study (Gilbody et al., 2015) was rated as ‘some concerns’ and one ‘high risk’ (Rogers et al., 2017) on the ‘measurement of outcome’, due to reliance in part or fully on self-report measures of abstinence. For those references assessed by the ROBINS-I tool (Table 6), all three were considered to be at serious risk of bias. This was largely due to ‘bias due to confounding’, for example, not controlling for confounding variables such as severity of mental illness or smoking history. Decisions on risk of bias assessments can be found in Supplementary 3.
Risk of bias assessments (RoB 2.0).
Filia et al. (2014) conducted a secondary analysis of the study by Baker et al. (2006) on the same outcome time point.
Clark et al. (2017) conducted a secondary analysis of the study by Baker et al. (2015) on the same outcome time point.
Thorndike et al. (2016) conducted a secondary analysis of the study by Evins et al. (2014) on the same outcome time point.
Risk of bias assessments (ROBINS-I).
Meta-analysis of effect of intervention
Point-prevalence abstinence overall
The aggregated estimate for point-prevalence abstinence was 1.49 (95% CI = [1.05, 2.11], p = 0.03), indicating an overall 49% higher odds for the intervention groups to show abstinence at follow-up compared to control groups (Figure 2). Heterogeneity was low to moderate (I2 = 34.9%, Q = 26.42, df = 17, p = 0.07). There was evidence of asymmetry, indicating possible publication bias. So, the overall effect size was re-estimated as OR = 1.38 (95% CI = [0.92, 2.10]).
Overall effect of any intervention versus no intervention measured via point-prevalence abstinence.
Point-prevalence abstinence by follow-up time
Only one reference had a follow-up time of less than 6 months. This was collapsed into the 6–12 months category, thus the analysis was run on only two subgroups. For the less than or equal to 12 months subgroup, the aggregated estimate for abstinence was 1.69 (95% CI = [1.12, 2.56]), indicating an overall 69% higher odds for intervention groups to show abstinence at follow-up within 12 months compared to control groups (p = 0.06). For the greater than 12 months subgroup, the aggregated estimate for abstinence was 0.95 (95% CI = [0.53, 2.11], p = 0.54; Figure 3).
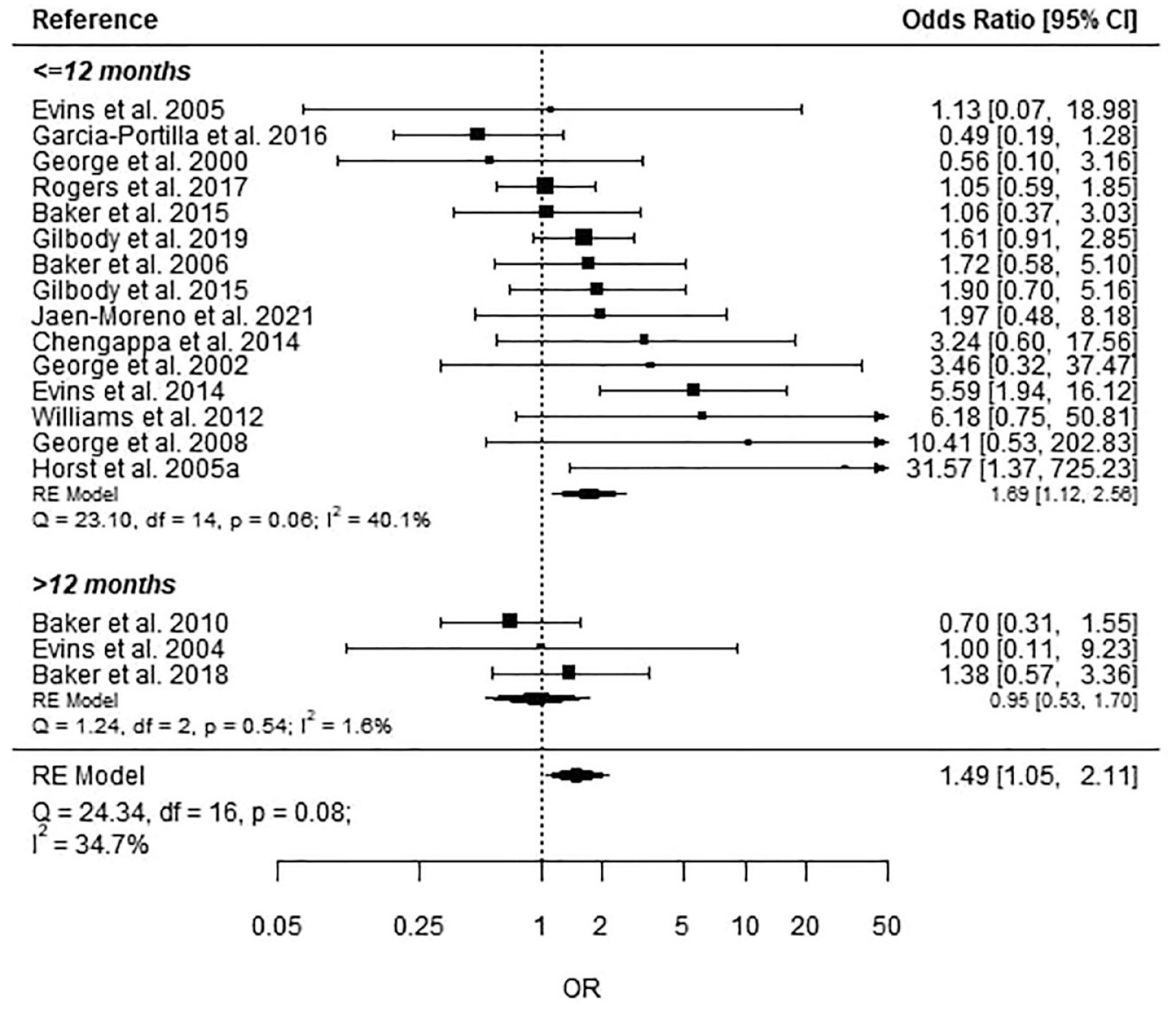
Point-prevalence abstinence by follow-up time.
Continuous abstinence
As there were only five references included, no subgroup analyses were performed. The estimated OR = 1.60 (95% CI = [0.67, 3.83], p = 0.29) showed higher odds in the intervention groups for continuous abstinence relative to control groups, but the CI was wide. There was no evidence of asymmetry, though with only five studies this is difficult to demonstrate (Supplementary 4).
Discussion
Summary of findings
To our knowledge, this is the first study to systematically review the literature examining the factors associated with sustained abstinence in people experiencing SMI following a smoking cessation intervention. The key finding was that participation in smoking cessation and relapse prevention interventions in general was associated with higher odds of abstinence in medium-term follow-ups compared to control groups. This finding was of borderline significance at up to 12-month follow-up, but the effect was no longer demonstrable at follow-ups greater than 12 months. There was a lack of information on the effect of other factors associated with abstinence in the short, medium and long term, largely due to their being rarely measured beyond the end of smoking cessation studies. Despite increased interest in investigating smoking cessation interventions in people with SMI, there was a lack of well-designed studies of sufficient sample size that investigate the important question of what factors predict sustained abstinence following successful quitting.
The majority of references included in the review explored the association between intervention and abstinence. The finding that participation in an intervention overall increased the odds of sustained abstinence at follow-up, compared to control groups, suggests the interventions do have a positive impact on sustained abstinence in this population. However, this finding may be skewed by the much higher odds reported by two relapse prevention studies, which provided more intense support for a longer duration. Furthermore, the heterogeneity in study and intervention types included in this review meant that more detailed analyses to establish whether particular interventions were associated with greater effects could not be conducted.
In short-term follow-ups (i.e. <6 months) only therapeutic relationship was reported as a significant factor in predicting sustained abstinence, however, this was measured by just one reference and was at moderate risk of bias. Most references measured the effect of potential predictors of abstinence over the medium term (i.e. 6–12 months), with the effect of intervention most commonly examined, followed by programme attendance. There was limited measurement of participant characteristics such as demographic background, psychiatric diagnosis or smoking behaviours when commencing the intervention. Factors associated with abstinence over long-term follow-up (i.e. >12 months) were rarely measured, and only smoking reduction in one previous trial was reported to have a significant relationship. However, the sample size was small and the study was considered at high risk of bias due to participants in the placebo group taking the study drug during the follow-up period.
Abstinence rates in the included studies varied widely depending on the length of follow-up and whether abstinence was assessed via point-prevalence or continuous abstinence measures. Point-prevalence estimates ranged between 6.6% and 45.0% at longest follow-up, while continuous abstinence measures revealed more conservative estimates of 5.4–19.0% at 6-month follow-up and 3.9–14.3% at 12-month follow-up. Although this is only reflective of the included references, and prevalence rates may differ in the broader smoking literature on people experiencing SMI, it highlights the relatively low sustained abstinence rates in this group. While direct comparisons cannot be drawn, general population estimates report a smaller and higher range of 25–50% point-prevalence of abstinence in the 12 months following a quit date (Ferguson et al., 2005; García-Rodríguez et al., 2013), depending on the intervention, length of follow-up and method used for determining abstinence.
Session attendance was examined by seven references and significantly associated with abstinence outcomes in three. Since the study interventions differed in length and intervention type, direct comparisons could not be drawn and an ideal attendance rate could not be concluded. Similarly, therapeutic relationship was related to abstinence in one study (Williams et al., 2010). These findings suggest that participant engagement may be an important factor for success; however, the small number of references examining these factors meant the evidence of an effect could not be determined.
There was limited evidence for a relationship between participant characteristics and smoking abstinence. Only one of three references found an association with age, in which participants in the abstinent group were older (Thorndike et al., 2016) and one of four references found a significant association with gender (Clark et al., 2017). Female participants were found to report a higher likelihood of sustained abstinence than their male peers, in contrast to the broader research on smoking cessation in which women reportedly face greater difficulties in maintaining long-term abstinence (Smith et al., 2016). Sampling bias may contribute to this finding, as a higher proportion of participants were male.
Only one reference of the six, which examined antipsychotic medication as a correlate, found a significant effect. Those prescribed an atypical antipsychotic were more than twice as likely to report abstinence at follow-up than those on typical antipsychotics (George et al., 2000). Other references, which examined mental health diagnosis and type of antipsychotic prescribed, found no significant relationship to smoking abstinence. Given that the inclusion criteria required participant samples to primarily comprise people experiencing a psychotic disorder, and that none of the references directly compared to a general population sample, it is likely that the homogeneity in diagnosis prevented any meaningful association with sustained abstinence being detected. The inclusion of people experiencing SMI in large RCTs would provide further information on the effect that mental health diagnosis may have on long-term abstinence outcomes in relation to the general population (Talukder et al., 2021).
Despite people experiencing SMI reporting heavier smoking and greater nicotine dependence than the general population, smoking characteristics at baseline were not related to sustained abstinence in the four references that were examined for this, suggesting that they may not be contributing factors to the lower success and abstinence rates in this group. Alternatively, this may reflect that quitting smoking is equally difficult regardless of smoking heaviness and dependence, or that there is not enough range in the variable to show a correlation with the outcome (abstinence) due to all participants scoring highly.
Finally, evidence for the role of physical health factors in smoking abstinence outcomes was limited to a single reference (Thorndike et al., 2016). Following a varenicline intervention, participants in the abstinent group reported higher rates of cardiometabolic issues than those who relapsed to smoking. This may suggest that poorer physical health acted as a motivating factor for continued abstinence, in line with findings from the general population in which ‘health concerns’ are often cited as a reason for smoking cessation (McCaul et al., 2006).
A number of factors commonly reported as being associated with smoking abstinence and/or smoking relapse in the general population were not measured in the studies included in this review. For instance, education, substance use, financial reasons, smoking status of social and household contacts, family and peer support to quit and social consequences of smoking (e.g. others dislike scent; Lee and Kahende, 2007; Murray et al., 2000). These may have provided a more comprehensive picture of the factors involved in successfully maintaining abstinence in people experiencing SMI and whether these differ from those seen in the general population.
Methodological considerations
Criteria for inclusion in this review required a minimum of 3-month follow-up to measure abstinence (point-prevalence or continuous abstinence), shorter than the Cochrane accepted and Russell Standard’s recommended 6 months (West et al., 2005). Given the scarcity of studies in this population and the well-documented rates of relapse, the shorter period was chosen to broaden the number of studies captured and increase the likelihood of a period of abstinence being reported. The majority of references measured abstinence outcomes via objective means, with all except two (Addington et al., 1998; Rogers et al., 2017) utilising CO monitoring in keeping with best practice in cessation trials. However, the definition of abstinence and cut-off for CO readings varied and the preferred standard of measuring abstinence – defined as continuous abstinence for 3 months or more – was met by only six references. A consistent approach to defining abstinence, as outlined in the Russell Standard, would improve comparability between studies and bring clarity to the interpretation of their effectiveness (West et al., 2005). Furthermore, inclusion in the review required study samples to have at least 75% of participants experiencing a psychotic disorder, or that the data required for extraction to be reported separately for people with a psychotic disorder, resulting in well-known studies such as the EAGLES study (Anthenelli et al., 2016) being excluded.
Finally, a number of the studies included were designed to primarily address the safety of pharmacological therapies and to assess their impact on psychiatric symptoms. This, in addition to high dropout rates, resulted in small sample sizes that are potentially underpowered to detect any meaningful effect of the interventions on sustained abstinence or factors associated with abstinence.
Strengths and limitations
All studies included in this review were investigating smoking abstinence via an intervention and their eligibility criteria required that participants were interested in smoking cessation. This increases the likelihood that the abstinence rates reported, and any factors associated with them, are representative of people experiencing SMI who are motivated to cease smoking. In addition, the inclusion criteria for this review focused only on people with psychotic conditions, therefore findings may not be generalisable to other mental illnesses that are often grouped under the term SMI (e.g. posttraumatic stress disorder [PTSD], severe depression).
The exclusion of studies that examined enforced smoking cessation, for instance, during hospital stays, may have inadvertently limited the review to studies that only encompass participants living in the community. Furthermore, since this review aimed to examine factors associated with smoking abstinence, studies investigating the impact of interventions on smoking reduction were excluded. While complete abstinence is most desirable given the health benefits of doing so, a reduction in smoking and nicotine consumption may also warrant investigation as this may be a more achievable real-world goal. Future research may examine factors associated with smoking reduction and draw comparisons with those associated with abstinence to identify where additional supports may be needed to move people towards abstinence. A better understanding of the potential benefit of e-cigarettes and novel approaches such as tailored text messaging support (Boland et al., 2018) warrants exploration in the SMI population (Kock et al., 2019).
Finally, a meta-analysis was completed to examine the overall effect of receiving an intervention on sustained abstinence, compared to no intervention; however, the variation across included references in study design, type of intervention delivered and measurement of abstinence, in addition to the limited data available meant that more complex analyses could not be conducted for individual factors. Furthermore, we had planned to conduct subgroup analyses by intervention type, however, this was not possible due to variance within types (e.g. behavioural interventions encompassed a range of approaches) and were often combined meaning the effects of each could not be separated). Where more data are available in the future, further research may employ more sophisticated methods to further develop knowledge in this area.
Recommendations
While much of the research into smoking cessation in people experiencing SMI has focused on developing interventions to support quitting, a greater focus on supporting long-term abstinence is much needed. None of the included studies explicitly examined predictors of sustained abstinence and most only examined intervention as a correlate with abstinence outcomes. Future research could focus on identifying the specific factors that contribute to ongoing abstinence in people experiencing SMI, which may aid in the design of more effective interventions. Co-designing smoking cessation interventions with people experiencing SMI who smoke may also assist in ensuring interventions meet these specific needs and are appropriate in their demands on participants.
More high-quality research is needed to determine the long-term effectiveness of pharmacological treatments such as varenicline, bupropion and NRT on smoking cessation in people experiencing SMI. While such medications appear to aid in initial smoking cessation attempts, to date there is limited evidence on their long-term benefits in people experiencing SMI, how they can be used to promote sustained abstinence and whether any adverse events may be associated with prolonged use in this population.
Conclusion
Future research should aim to better understand how abstinence can be maintained following a smoking cessation attempt among people experiencing SMI. Further assessment of the effectiveness of interventions designed to promote ongoing cessation and prevention of relapse among larger sample sizes is needed, with a particular focus on identifying predictors of long-term abstinence in this population. High-quality research that minimises risk of bias is needed to enable better understanding of this important question.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221147206 – Supplemental material for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention
Supplemental material, sj-docx-1-anp-10.1177_00048674221147206 for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention by Kimberley Davies, Ryan J Courtney, Miranda Summersby-Mitchell, Rachel Morell, Nancy Briggs and Julia M Lappin in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674221147206 – Supplemental material for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention
Supplemental material, sj-docx-2-anp-10.1177_00048674221147206 for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention by Kimberley Davies, Ryan J Courtney, Miranda Summersby-Mitchell, Rachel Morell, Nancy Briggs and Julia M Lappin in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-3-anp-10.1177_00048674221147206 – Supplemental material for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention
Supplemental material, sj-docx-3-anp-10.1177_00048674221147206 for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention by Kimberley Davies, Ryan J Courtney, Miranda Summersby-Mitchell, Rachel Morell, Nancy Briggs and Julia M Lappin in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-4-anp-10.1177_00048674221147206 – Supplemental material for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention
Supplemental material, sj-docx-4-anp-10.1177_00048674221147206 for A systematic review of factors associated with sustained smoking abstinence in people experiencing severe mental illness following participation in a smoking intervention by Kimberley Davies, Ryan J Courtney, Miranda Summersby-Mitchell, Rachel Morell, Nancy Briggs and Julia M Lappin in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research was supported by the National Drug and Alcohol Centre (University of New South Wales), which is supported by funding from the Australian Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by a Career Development Fellowship (grant no. 1148497; awarded to Dr Courtney) from the Australian National Health and Medical Research Council.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.