
Abstract
Self-harm in adolescents is common, with the prevalence ranging from 4% in the general adolescent population to 60–80% of adolescent psychiatric inpatients [1]. Self-harm is a risk factor for suicide attempts, with 70% of adolescents who self-harmed also reporting at least one suicide attempt [2].
The term self-harm encompasses a wide range of intentions and behaviours. Deliberate self-harm (DSH) describes a purposeful self-injurious act committed without intent to die [3]. A suicide attempt refers to engagement in potentially self-injurious behaviour in which there is at least some intent to die [4]. Suicidal ideation refers to thoughts of harming or killing oneself [5]. Suicidal behaviour is a broad term that ranges from death by suicide to intentional, non-fatal self-harm [6]. For the purposes of this literature review, when the term ‘self-harm’ is used, it includes both suicide attempts and self-injury without suicidal intent.
Most theoretical models of self-harm propose a diathesis-stress model in which the psychiatric, psychological, and biological factors predispose a person to suicidal behaviour, while stressful life events interact with such factors to increase the risk [5]. The most common reported reason for self-harm is to relieve unwanted feelings, with self-harm functioning as a form of emotional regulation [7]. In a study of self-harm among community adolescents the most common reasons for self-harm were: feeling depressed or all alone, negative feelings toward themselves, a means of distraction or feeling a need to hurt oneself [8].
Self-harm is one of the most serious global health problems for adolescents and young adults. DSH is one of the top five causes of acute hospital admissions for young people [9]. A study of 7854 high school students showed that 6.2% of the students met the criteria for DSH in the previous 12 months [10], and 29 anonymous self-report questionnaire studies from nine countries revealed that between 7and 10% of adolescent students reported having made one or more suicide attempts [11]. In addition, World Health Organization (WHO) data describe the global rate of suicide increasing between 1950 and 2004 [4]. More than 60% of Australian university-age students reported suicidal ideation [12].
An Australian epidemiological study described 12% of 13 to 17 year olds reporting suicidal ideation, 9% a suicide plan, 4.2% a suicide attempt and 0.9% a suicide attempt requiring treatment. Non-suicidal DSH was not investigated in this survey [13]. Depression was the main risk factor for suicidal ideation and attempts in a New Zealand longitudinal cohort, but other risk factors included a family history of suicide, childhood sexual abuse, peer affiliations and poor school achievement [14]. A Western Australian study found that being female, having a parent who smoked, being in a step/blended family, having emotional problems as a child, living in a family with an inconsistent parenting style and having a teenage mother increased the risk of later hospitalization for self-harm [15].
Other demographic factors demonstrated to be risk factors for suicidal behaviour include being female, being young and having lower educational achievement [16,17]. Differences between races are also seen, with Caucasians more likely to engage in self-harming behaviour than African-Americans [1]. Psychiatric disorders such as major depression, anxiety disorders, eating disorders, impulse-control disorders, addictions, psychotic and personality disorders are important risk factors for suicidal behaviour [3,17–19]. The presence of multiple disorders is especially associated with an elevated risk [4]. Other demonstrated predictors are sexual abuse in childhood, experiencing major life events, multiple hospital admissions and previous episodes of self-harm or suicide attempts [5,20,21].
There is evidence for a heritable risk of suicide and suicidal behaviour, even after controlling for heritable disorders such as mood and psychotic disorders [4]. Monozygotic twins have a higher concordance of suicidal behaviour than dizygotic twins [22], even when controlling for other risk factors such as diagnosis. In one twin sample all first suicide attempts were made before the age of 18, suggesting that genetic risk was most likely to initially present in adolescence [23].
Family relationship difficulties are also associated with self-harm, with one study finding that 77% of 710 children with self-harm reported difficulties in relationships with family members. In this study the next most frequent type of problem concerned relationships with friends, particularly in females. Problems with schoolwork were recorded for more than two thirds of the patients [21]. Other studies have confirmed family relationship factors such as parenting style as a risk factor [15].
In addition to diagnostic, personal and social factors, it has been suggested that ward situational factors such as the length of stay, the number of admissions and amount of leave from the ward are related to suicidal behaviour [24,25]. However, there is a lack of evidence for this hypothesis. Concerning staff attitudes, a study by Wheatley and Austin-Payne [26], who investigated nursing staff knowledge and attitudes towards self-harm, found that staff who had negative attributional theories about the reasons young people self-harmed were less likely to want to assist them when they were distressed. Staff can also have gaps in knowledge, especially about subgroups of the population who are at higher risk of self-harming behaviour [27].
Accurate knowledge about factors linked to self-harm is crucial for staff working in an inpatient unit, not only to identify those young people at most risk and minimize repeated self-harm, but also to design interventions to prevent and manage this behaviour. It is also important to understand possible protective factors. One study demonstrated that clinical assessments of risk in first time cases of self-harm are predictive of further episodes [28]. This knowledge about risk and protective factors could be used in the development of an effective inpatient treatment program targeting minimization of self-harm and suicidal behaviour.
Aim
The aim of this research was to describe risk factors for self-harm for children and adolescents in a mental health inpatient unit.
Method
Participants
All participants were patients admitted to a mental health inpatient unit of a paediatric teaching hospital in Sydney, from January 2006 to December 2009. A file audit was used to identify risk factors for self-harm. In total, 294 patients were admitted from January 2006 to December 2009. From this group 150 patients with self-harm were identified. Six patients were excluded due to insufficient data, resulting in a final sample of 144. The non-self-harm group consisted of a consecutive sample of 56 patients without self-harm (neither in the past, nor during admission), who were admitted during the same time period.
Self-harm group
All patients who exhibited any form of self-harm prior to admission or as an inpatient were included in this group. Past self-harm was identified by file audit. Self-harm as an inpatient was identified from the Incident Management System (IMS), an electronic program designed to track and manage adverse events in hospitals. Nurses, doctors and other staff members across all shifts electronically recorded all incidents of aggression, absconding or self-harm according to mandatory guidelines, with reports regularly monitored by the Nursing Unit Manager for accuracy and appropriateness of reporting [29].
The mean age of the group with self-harm was 14 years (range 6–16 years), with 73% female, 92% were born in Australia, 96% had an English speaking background and 4% identified as Aboriginal.
Non-self-harm group
The mean age of this group was 13 years (range 7–17 years), with 50% female, 73% were born in Australia, 89% had an English speaking background and 3% identified as Aboriginal.
Data analysis
A retrospective file audit of patient files was conducted using Powerchart, a computerized medical record system. A file audit checklist was developed for both the self-harm group and the control group. The recorded data were divided into multiple categories, based on risk factors found in a review of the literature. Factors included demographic information, diagnosis, home situation, environmental stressors, any history of trauma and previous mental health care. The records were reviewed twice, once by the first author and then by another author (E.B.), to minimize intrapersonal bias.
Statistical analysis
Statistical analysis was performed using SPSS version 15 (Chicago, IL). To determine factors associated with self-harm a binary logistical regression analysis was used, with self-harm as the dependent variable. A chi-square test was undertaken as the initial analysis, with age converted to a binary variable (10 and under, 11 and above). The factors found to be significantly associated with self-harm were entered into a logistical regression analysis, in order of significance; that is, using a sequential forwards method. Variables were entered if they met a significance of p < 0.05 or an adjusted odds ratio (OR) (exp (B)) of > 2.
Results
Descriptive findings
Of those who self-harmed the most common behaviour was cutting, in 57% of subjects, followed by poisoning (47%). Other methods used included self-strangling (7%), self-hitting (6%), head banging (4%), swallowing objects (4%) and burning (3%). Sixty-seven percent had a history of more than one self-harm episode. Twenty percent of subjects with a history of self-harm hurt themselves during their admission, most commonly by cutting (10%) or attempting to strangle themselves (8%). Other methods used were hitting (5%), head banging (4%), poisoning (3%) and swallowing objects (1%). Half self-harmed more than one time during their admission.
Patients with self-harm had two admissions on average and a mean length of stay of 19 days. On average, those without self-harm had just one admission, but a longer mean length of stay of 31 days. The most common diagnosis in the DSH group was depression (60%), followed by adjustment disorder (34%) and post-traumatic stress disorder (PTSD) (26%). In the group without self-harm psychosis was the most common diagnosis (29%), followed by attention-deficit hyperactivity disorder (ADHD) (25%) or anxiety disorder (25%).
Of the patients with DSH 58% were not living in an intact family (i.e. without one or both of their biological parents) compared to 45% of the controls. Of those with DSH 22% were living with a stepmother or stepfather, compared to 7% of those without self-harm. A high percentage of DSH patients reported environmental stressors, with family stressors the most common (94%), followed by problems at school (90%) and friendships (78%). Those without self-harm also had a high percentage of environmental stressors, but their most common stressor was school (84%), followed by problems within the family (71%) and friendships (59%).
A history of trauma was reported by 91% of those who self-harmed, with the most common reported trauma being bullied at school (39%). A history of trauma was also seen in 52% of the non-self-harmers, with bullying at school again the most commonly reported trauma (18%). Sixty-nine percent of the self-harmers had a family member with a mental health history, compared to 66% of the non-self-harmers. Forty percent of the self-harmers had no history of mental health care prior to admission, while only a quarter of the non-self-harmers had no mental health care before their admission.
Univariate analysis
As shown in Table 1, in the univariate model self-harm was associated with being 11 years of age or older (OR = 8.0), female gender (OR = 2.0), being born in Australia (OR = 3.4) and living with a step parent (OR = 3.6). Patients who did not receive mental health care before their first admission were also significantly more likely to have self-harmed (OR = 2.06). A diagnosis of depression was associated with almost a five-fold increase in self-harm (OR = 4.9).
Univariate and multivariate regression analysis of variables associated with self-harm
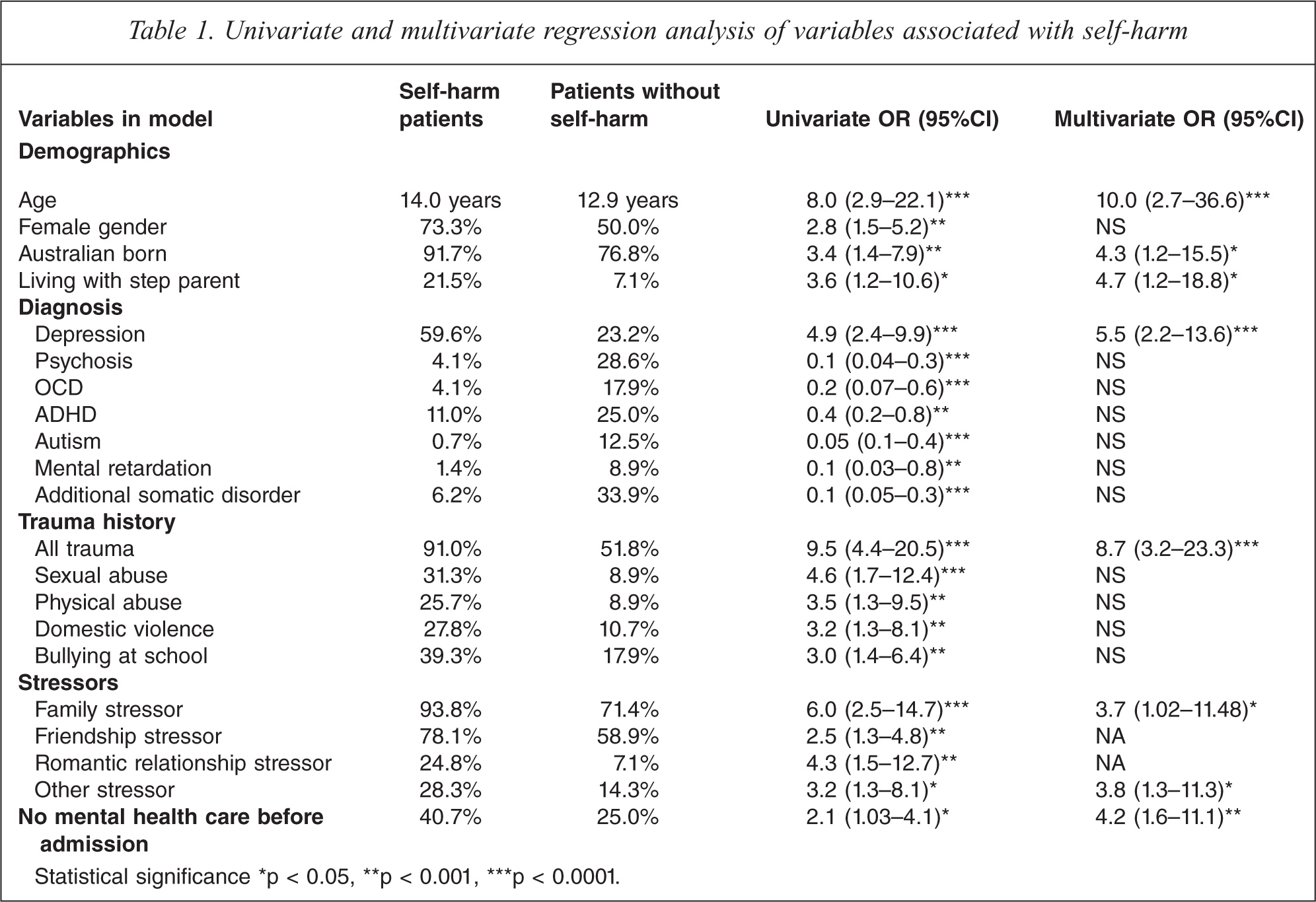
Statistical significance *p < 0.05, **p < 0.001, ***p < 0.0001.
A history of any form of trauma was associated with a nine-fold increase in self-harm (OR = 9.5). A history of sexual assault was associated with almost a five-fold increase (OR = 4.6). Other significant reported traumas included being bullied at school (OR = 3.0), physical abuse (OR = 3.5) and domestic violence (OR = 3.2). Reported conflicts or stressors in the family increased the risk six times (OR = 6.0). Other stressors included romantic relationship break-ups (OR = 4.3), conflicts with friends (OR = 2.5) and any other stressors (OR = 3.2), for example, moving between different group homes or religious pressure.
Suicidal behaviour was less likely to occur with patients with a diagnosis of psychosis (OR = 0.1), autism (OR = 0.05), OCD (OR = 0.2), mental retardation (OR = 0.1), ADHD (OR = 0.4) or an additional somatic disease such as asthma or diabetes (OR = 0.1).
Multivariate analysis
The final multivariate model is shown in Table 1 and Figure 1, which graphs the OR and 95% confidence intervals of the final variables in the model. This model accounts for 54% of the variance in self-harm. Gender was not significant in this model. Self-harm was ten times more likely in patients aged eleven and over (OR = 10.0) and five times more likely in those living with a step parent (OR = 4.7). Self-harm was increased more than five times in patients with depression (OR = 5.5) and was almost nine times more likely in subjects who had a history of trauma (OR = 8.7). A history of family problems increased the risk almost four fold (OR = 3.7) as did other reported stressors (OR = 3.8). Patients without mental health care prior to admission were more than four times more likely to self-harm than those who had accessed some form of mental health care (OR = 4.2). Those born in Australia had a greatly increased risk of self-harm compared to those born in other countries (OR = 4.3).
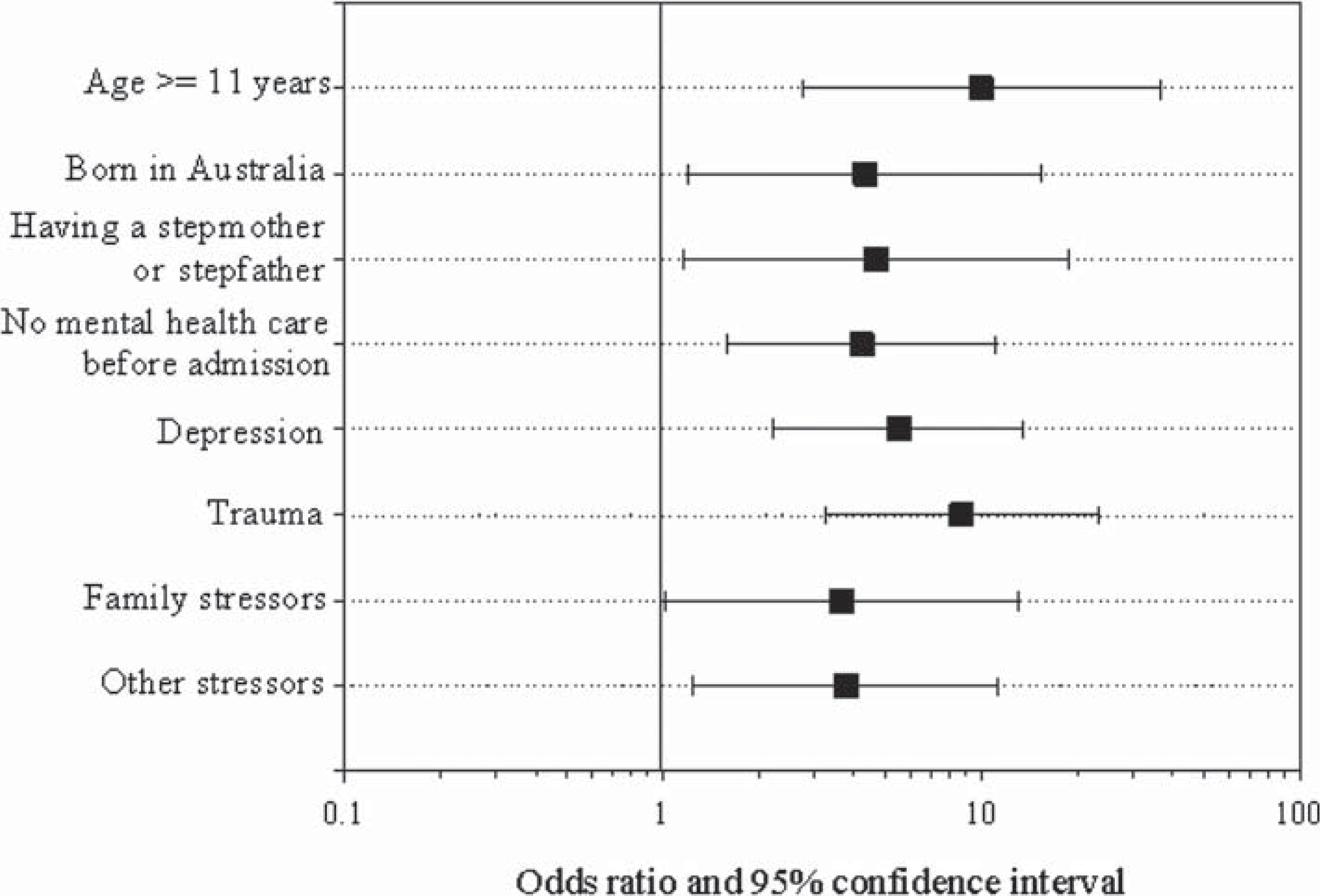
Adjusted odds ratios of factors associated with self-harm.
Discussion
This study found that 51% of the children and adolescents admitted to a mental health inpatient unit harmed themselves before or during admission, with higher rates among females and those aged 11 years or older. These rates are similar to those found in previous studies [1,16,17,21] and confirms that self-harm or suicidal behaviour is one of the major symptoms reported by adolescents in mental health inpatient units.
The methods of self-harm were similar to those found in previous surveys of community samples of adolescents [10,27]. Cutting was the most common method of self-harm, followed by self-poisoning.
Several factors were identified that increased the likelihood of self-harm, including a diagnosis of depression, female gender, increasing age, being Australian-born, living with a step parent, not having received previous mental health care, having a history of trauma, and having other stressors such as problems within the family, with friendships or at school. Many of the results have been reported in previous studies as risk factors for self-harm [27], in particular depression, older age and female gender [13,15, 30].
Those with self-harm were less likely to be living in an intact family but this was not statistically significant. However, living with a step parent increased the risk in our group, even in the final model where trauma was included as a potential confounder. Samm et al. [31] studied 4389 school children and found that of the adolescents in non-intact families, those with a step parent in the family reported suicidal thoughts more frequently than adolescents in single parent families. The most likely explanation for this is that living with a step parent is an epiphenomenon of earlier abuse, however, this remains a risk factor in our study even when earlier abuse is controlled for. Living with a step parent could also be an additional risk factor because of divided parental attention (e.g. a parent attempting to meet the needs of both their child and their new partner) and the consequential loss of focus on the child or adolescent. Children with psychological disorders may also be more likely to develop a conflictual relationship with a step parent because they have a mood or behaviour disturbance. It is also possible that a child has negative feelings about a step parent living with them, and this adds to their risk of self-harm. However, such hypotheses need further investigation.
The presence of sexual abuse and romantic relationship stressors were no longer significant contributors to outcomes when the factor depression was added to the regression analysis. This suggests that these two factors mediated their effects through an increase in depression, or that the sample size was not large enough to show an effect. Previous research has found that the presence of romantic stressors, such as a break up, was associated with higher levels of depression and behaviour problems. Romantically involved girls experienced higher levels of depressive symptoms, while romantically involved boys had higher levels of externalizing behaviours, compared to their non-dating peers [32]. A history of trauma remained highly significant in the final model, confirming other studies linking trauma and self-harm [20,21].
This study also revealed the presence of risk factors that have not been identified in previous research. Australian born young people had a greatly increased risk of self-harm in both the univariate and multivariate models. This study hypothesized that immigrants would show more suicidal behaviour than the native inhabitants, because of problems with acculturation, adjustment to a different culture and possible discrimination; however, our results showed the opposite. One possible explanation for our finding is that participants born outside Australia may have differing cultural backgrounds, and these cultures may protect against self-harm [5]. Religious beliefs may also come into play, as may a stronger family structure.
Another novel finding was that patients who did not receive mental health care before their first admission were significantly more likely to harm themselves than patients who did receive care before their first admission. This suggests either that self-harm is an early phenomenon of mental illness, in adolescents in particular, or that these patients were unable to access services until the identification of self-harm and an emergency response. Good clinical practice includes rapid access to mental health services when self-harm occurs, to prevent further episodes and treat any underlying mental illness [28]. It is of concern that some patients’ first access to services was when the symptoms were severe enough to require admission. This would suggest either a lack of awareness of the need for early intervention with self-harm, or a shortage of community mental health services, in particular crisis services, for children and adolescents in the hospital catchment area. An Australian survey found that only 50% of children and adolescents with mental health problems had attended any service during the previous six months and only 17% had attended a mental health service in the last month [13].
Previous studies have shown that documented problems within the family, friends, romantic relationships and problems at school can be major stressors for children and adolescents and can be risk factors for suicidal behaviour. The only stressor not significantly associated with suicidal behaviour in our study was school. This is most likely explained by the finding that the majority of both groups had documented problems at school, leading to little variance in scores.
Limitations of this study
The data for this study was obtained from a retrospective file audit and it is possible that some information may be missing. Self-harm as an inpatient was taken from the electronic incident management system and there may be varying thresholds for reporting among ward staff. We also used a broad definition of self-harm and were unable to clearly differentiate the motivation behind the self-harm, or to separate out risk factors for specific types of DSH.
The sample was drawn from just one ward so it is not possible to generalize the findings to other settings. Further research is needed to investigate risk factors for self-harm in internationally representative samples.
Recommendations
While increasing age, female gender, a history of trauma and a diagnosis of depression are well known as risk factors for self-harm our results suggest that family factors, in particular living with a step parent significantly add to the risk. While we may hypothesize about the reasons for this, child and adolescent services should be aware of the increased risk of self-harm in young people with mental health problems who live in blended families. This finding also validates the importance of treatment approaches involving the parent and step parent as well as the child or young person.
Although the findings are limited by the retrospective nature of this study and reliance on file audits, they provide clinically relevant information for considering risks for self-harm. This study supports the need for further research, particularly of a prospective nature, on factors related to self-harm in adolescents.
Footnotes
Acknowledgements
We would like to thank Jenny Peat for her statistical advice and Lucres Nauta, the research supervisor of L.M. and E.B. at De Vrije Universiteit, the Netherlands.