
Abstract
Suicide is the most common cause of premature mortality in schizophrenia, with a lifetime risk ranging from 4.9% to 10% [1, 2]. The prevalence of deliberate self-harm in schizophrenia is up to 50% [3]. Suicide prevention is one of the main targets of mental health care.
An inherent weakness of suicide studies is inadequate case findings. This is not merely a problem of attrition or short follow-up period for suicide outcomes, but because for any given subject at any given time, their ultimate status is unknown. This is counter to the basic rule of test development, that is, the requirement for a gold standard for comparison [4].
A suicide event should be conceptualized as a hazard or risk rather than as all-or-none status. A status of non-suicide could change to suicide as time progresses. A suicide that occurs early should be accounted for differently (possibly as a hazard function to indicate a higher risk) rather than as a suicide occurring late during the follow-up period. The time dimension should be treated as a key variable.
Nevertheless, the majority of previous studies used case–control designs. Hawton et al. conducted a systematic review and found only five longitudinal suicide studies among 1328 published studies [5]. A case–control study cannot account for time dimension of variables, it also assumes that controls in the study have a status of non-suicide at all times.
Objective
To overcome the aforementioned shortcomings, the author adopted a hazard analysis and cohort design. Castle Peak Hospital, Hong Kong is one of the five centres of Early Assessment Service for Young People with Psychosis (EASY) – an early intervention programme in Hong Kong. The aim of the present study was to identify risk factors for deliberate self-harm and completed suicide in young Chinese people suffering from schizophrenia.
Method
Subjects
In four consecutive years from 1 July 2002 to 30 June 2006, all patients who entered the early intervention programme with a chart diagnosis of schizophrenia in the computerized case register were recruited as subjects. The diagnosis of schizophrenia was confirmed using ICD-10 criteria, and further ascertained by consensus with an experienced consultant psychiatrist. Subjects with other principal psychiatric diagnoses were excluded.
Data collection
In the period between January and March 2007, case notes and discharge summaries of the subjects were reviewed. The follow-up period was calculated from the dates of the first and the last outpatient attendance prior to the time of data collection. Subjects were regarded as having completed suicide if the following two criteria were satisfied: (i) they were identified as dead at the end of the study period; and (ii) the cause of death was self-inflicted. The coroner's verdict was not used because it would have underestimated completed suicide cases [6–8]. Due to the fact that suicide intent is very difficult to prove, it was not included in the criteria of completed suicide in the present study. The nomenclature of deliberate self-harm was defined in accordance with guidelines of the World Health Organization/European Study on Parasuicide: ‘an act with non-fatal outcome, in which an individual deliberately initiates a non-habitual behaviour that, without intervention from others, will cause self-harm, or deliberately ingests a substance in excess of the prescribed or generally recognized therapeutic dosage, and which aimed at realizing changes which the subject desired via the actual or expected physical consequences’ [9]. The status of completed suicide and deliberate self-harm was ascertained by case-note review and computerized clinical data, and further clarified by interviewing treating staff. A proforma data retrieval form was used. Data concerning a total of 51 pre-defined independent variables (Appendix I) were collected.
Statistical analysis
Subjects were categorized into event groups and a censored group. Two event groups (completed suicide group and combined group of completed suicide and deliberate self-harm) were identified. The reason for combining completed suicide and deliberate self-harm cases was because a ‘pure deliberate self-harm’ group excluding completed suicide cases could cause selection bias and underestimation of suicidal behaviour.
The time to event, that is, the duration of time from the first attendance to the occurrence of either of the two outcome events, was calculated.
Statistical analysis was performed using SPSS for Windows version 14 (SPSS, Chicago, IL, USA). Univariate Cox proportional hazard model was used to assess the effect of 51 independent variables on the occurrence of dependent variables. Independent variables with p<0.05 were identified as risk factors for suicide. Multivariate Cox proportional hazard model was used to account for interrelationships between risk factors. PASS (version 2002) was used to calculate the post-hoc power for those variables that had been regarded as risk factors in the literature but were found to have insignificant p in the present study. Post-hoc power could estimate the size of Type II error for a particular independent variable.
Results
A cohort of 234 subjects was recruited (therefore 234 was the denominator for analysis). The mean follow-up duration was 953 days (range=22–1727 days). At the time of data collection 207 subjects were active cases. Inactive cases (n=27) included completed suicide (n=8), transfer-out (n=4; reasons for transfer out were not related to suicide), and dropout (n=15; i.e. not attending any psychiatric service for >1 month).
Event cases included completed suicide (n=8) and deliberate self-harm (n=29). Among the deliberate self-harm cases (n=29), four subjects committed suicide during the follow-up period. For ease of description, the combined group of completed suicide and deliberate self-harm is denoted by the term ‘suicidal behaviour’ (n=33). The mean follow up for suicidal behaviour (n=33) was 517 days (range=22–1666 days).
Sample characteristics
All subjects were Chinese in ethnicity. The male: female ratio was 1:0.8. The mean age was 21.9 years at the time of entering EASY. A total of 90.6% of subjects (n=212) in the cohort were single, 51.3% (n=120) were unemployed, 22.6% (n=53) were students, and 94.0% (n=220) were living with their families. Apart from having a diagnosis of schizophrenia, six subjects had a secondary diagnosis of mild mental retardation, three had borderline intelligence, and two had borderline personality disorder. The prevalence of substance misuse in the cohort was 21.4% (n=50). A total of 52.6% (n=123) of subjects had been admitted to a psychiatric hospital during an average of 2.6 years of follow up; 46.2% (n=108) of subjects were documented to have non-compliance or non-attendance for >1 month.
Rates of suicidal behaviour
Forty-eight subjects (20.5%) had a past history of deliberate self-harm prior to entering EASY. After an average of 2.6 years of follow up, 27.8% (n=65) of subjects had at least one episode of suicidal behaviour. The occurrence rate for suicidal behaviour (n=33) in EASY was 14.1%.
Risk factors for suicidal behaviour
Table 1 shows the comparative analysis of sociodemographic, extrapyramidal side-effect, and ‘level of care’ variables. Subjects with suicidal behaviour tended to have a history of substance abuse (p=0.07; power=0.44, which was inadequate to reject the null hypothesis). Table 2 shows the medications for the two groups of subjects prior to the outcome events or at the end of the follow-up period. The 11 risk factors identified in univariate Cox proportional hazard model are shown in Table 3.
Comparative analysis on sociodemographic, EPSE, and level of care variables
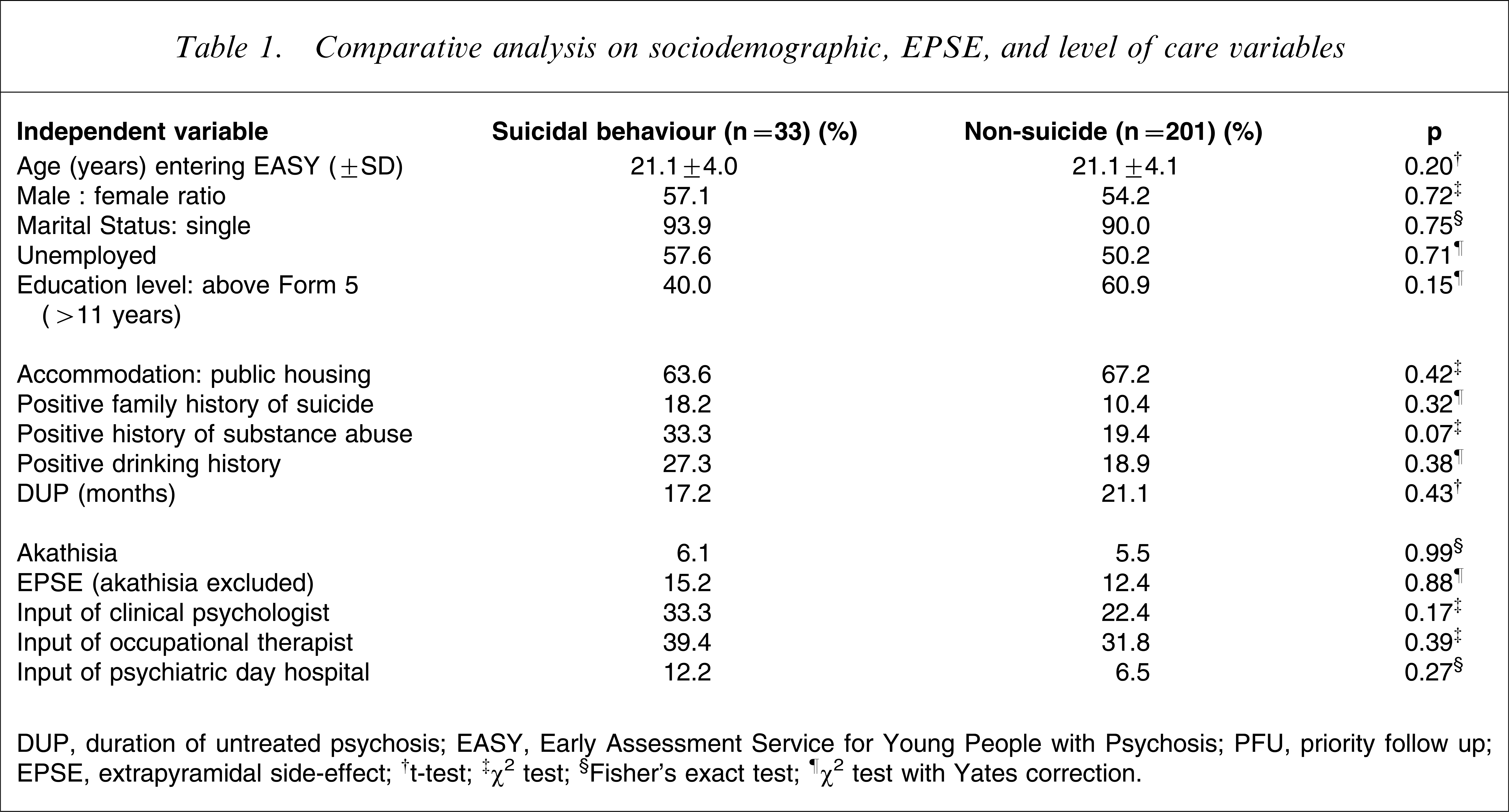
DUP, duration of untreated psychosis; EASY, Early Assessment Service for Young People with Psychosis; PFU, priority follow up; EPSE, extrapyramidal side-effect.
†t-test; ‡χ2 test; §Fisher's exact test; ¶χ2 test with Yates correction.
Comparative analysis on medication variables
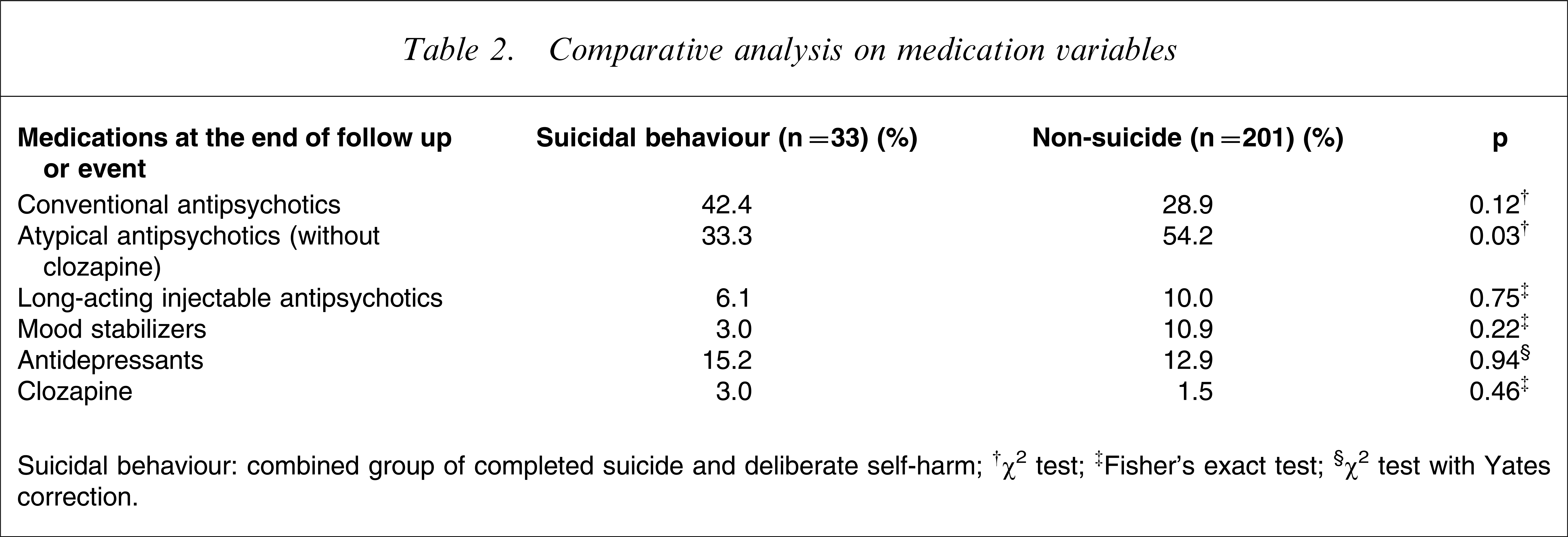
Suicidal behaviour: combined group of completed suicide and deliberate self-harm.
†χ2 test; ‡Fisher's exact test; §χ2 test with Yates correction.
Risk factors for suicidal behaviour (n=33; univariate Cox proportional hazard model)
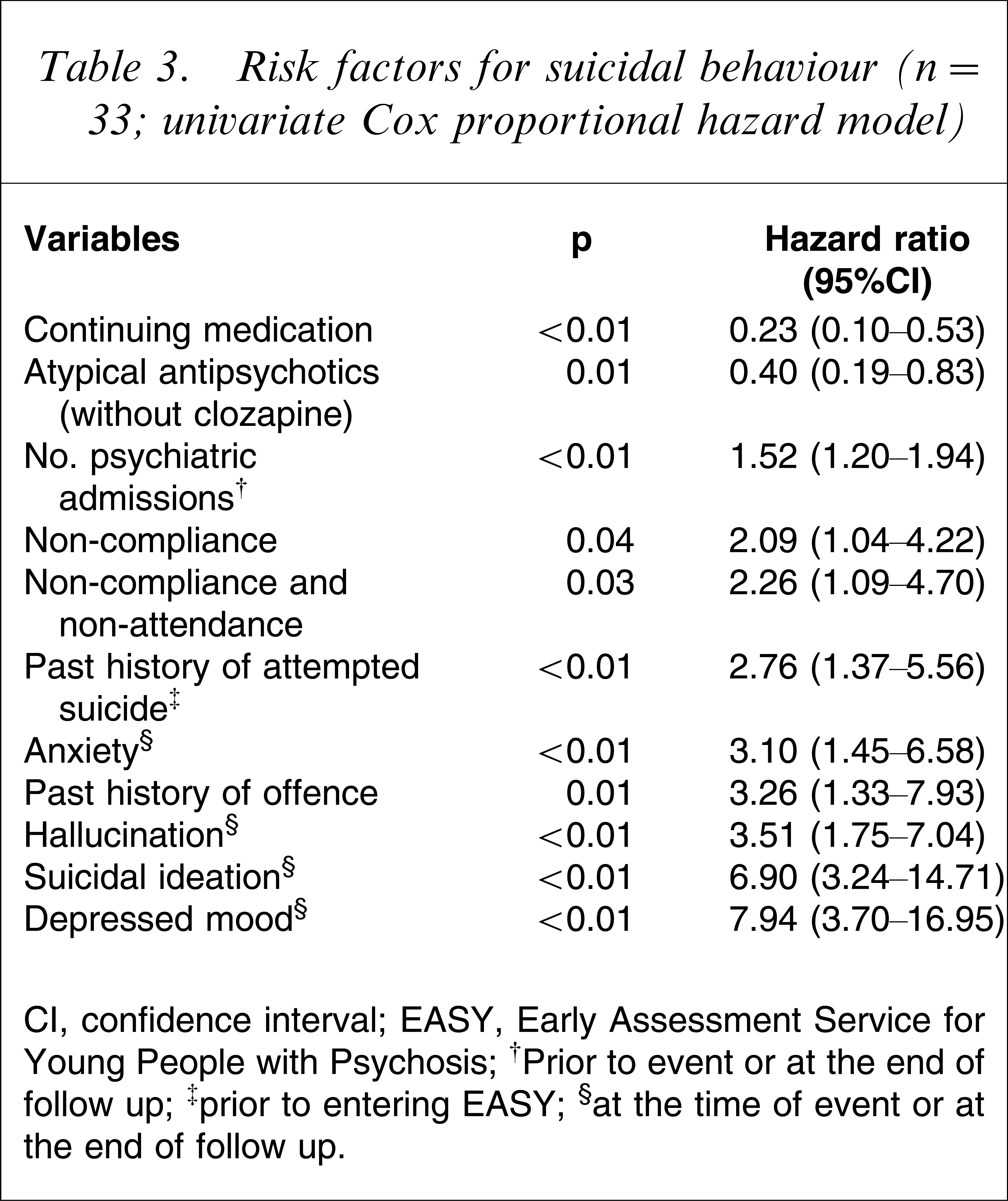
CI, confidence interval; EASY, Early Assessment Service for Young People with Psychosis.
†Prior to event or at the end of follow up; ‡prior to entering EASY; §at the time of event or at the end of follow up.
Based on the present sample size, multivariate analysis was able to identify significant models that contained three variables. After performing multivariate analysis on all the possible permutations (each containing three variables) of the 11 risk factors, the variable of ‘non-compliance’ was found to be insignificant. Table 4 details the significant multivariate model that best explains the variance.
Risk factors for suicidal behaviour† (n=33; stepwise multivariate Cox proportional hazard model‡)
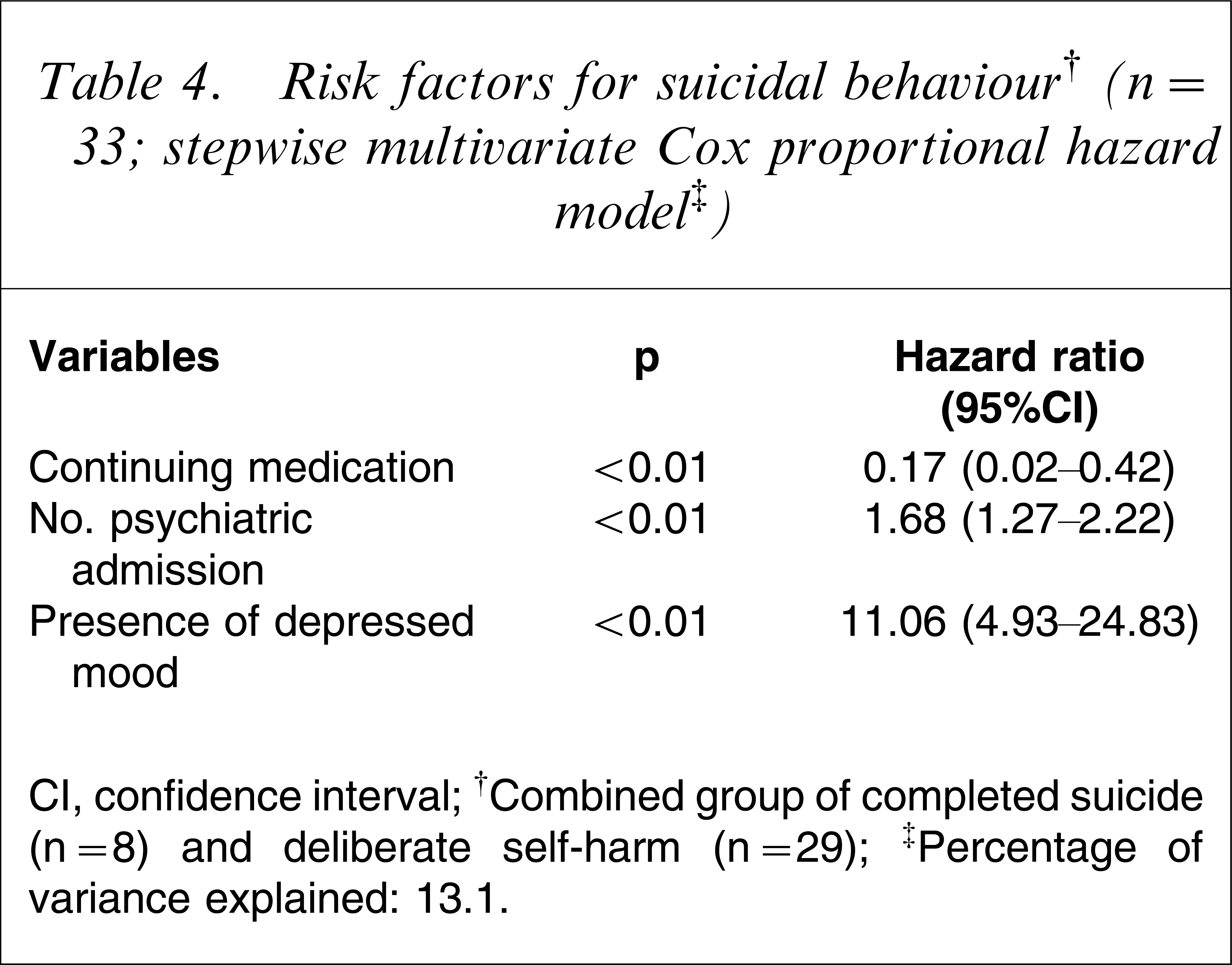
CI, confidence interval.
†Combined group of completed suicide (n=8) and deliberate self-harm (n=29).
‡Percentage of variance explained: 13.1.
Risk factors for completed suicide
The results of the univariate and multivariate Cox proportional hazard model are shown in Tables 5 and 6, respectively.
Risk factors for completed suicide (n=8; univariate Cox proportional hazard model)
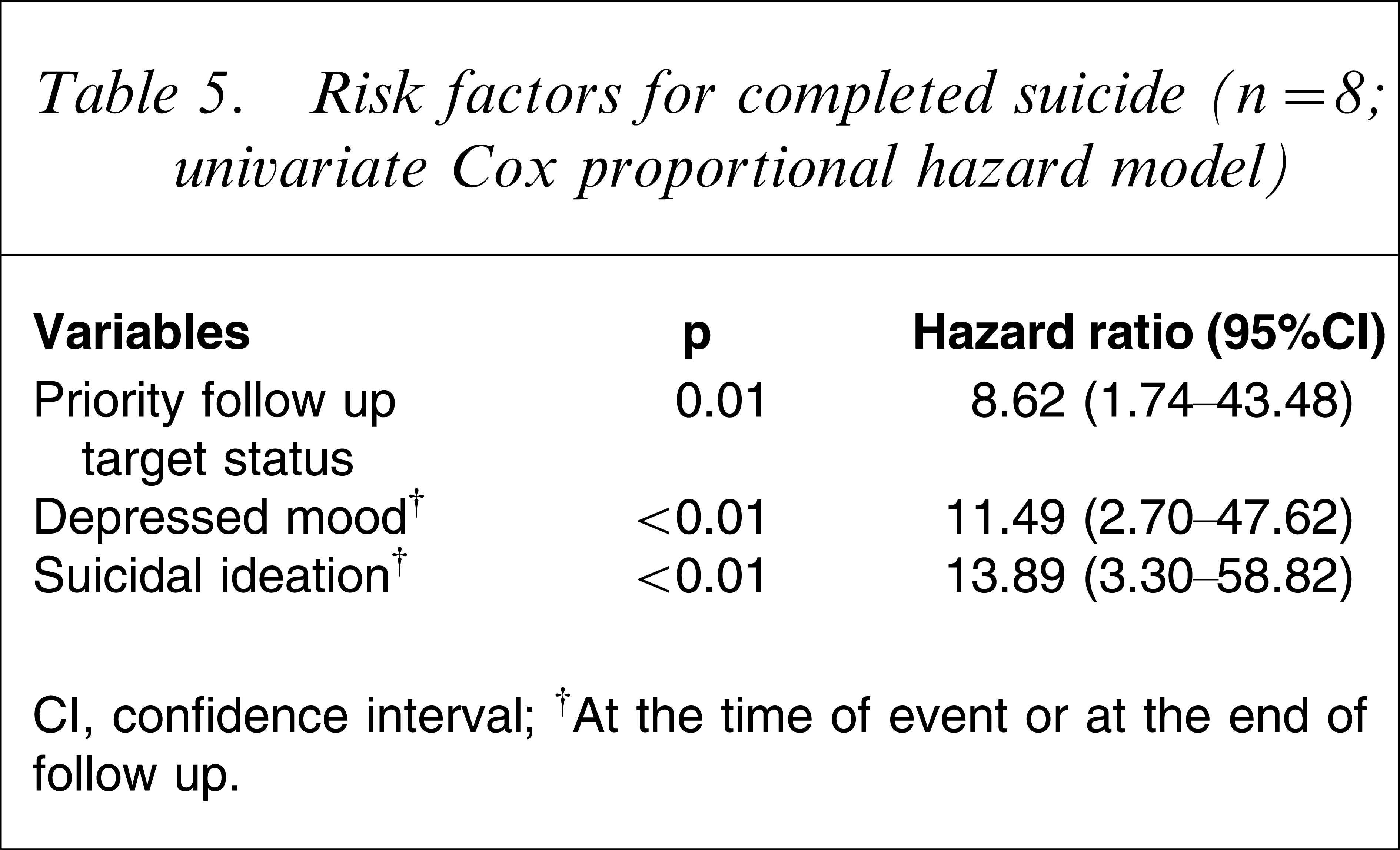
CI, confidence interval.
†At the time of event or at the end of follow up.
Risk factors for completed suicide (n=8; stepwise multivariate Cox proportional hazard model†)
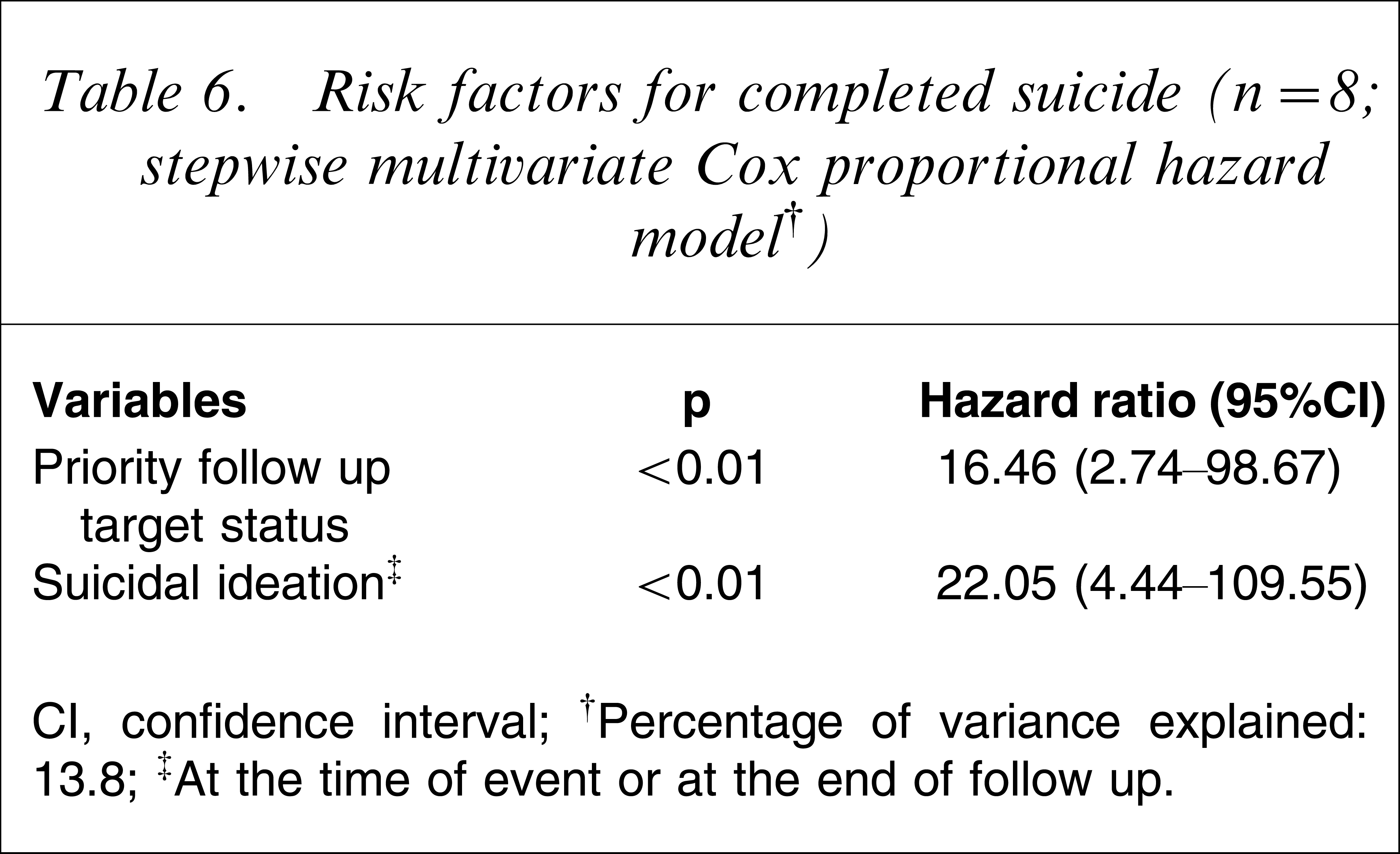
CI, confidence interval.
†Percentage of variance explained: 13.8.
‡At the time of event or at the end of follow up.
Discussion
The occurrence rate of suicidal behaviour (14.1%; n=33) in EASY is comparable to figures from other early intervention services. A French study on deliberate self-harm in first-episode psychosis found an occurrence rate of 11.3% in a 2 year follow-up period [10]. Another similar Danish study found a rate of 11.3% in a 1 year follow-up period [11]. By the end of an average of 2.6 years of follow up in EASY, 27.8% (n=65) of patients suffering from schizophrenia would have at least one episode of suicidal behaviour. This figure is less than the lifetime rates reported in the literature [2, 3]. Nevertheless, it suggests that suicidal behaviour occurs early in the course of schizophrenia.
Previously well-reported risk factors were found to be significant in the present study [5]. The association between depressed mood, a past history of attempted suicide, and future suicidal behaviour cannot be overemphasized. In the literature, depressed mood and a past history of attempted suicide are robust indictors of future suicide in schizophrenia and other psychiatric disorders [12]. Clinicians should assess carefully patients with schizophrenia who have a depressed mood and provide adequate treatment for depression. Biological and psychological intervention has proven effective in treating depression [13].
Risk factors more specific to Hong Kong
The priority follow-up (PFU) system was established in Hong Kong in 1982, whereby psychiatric patients with a history of violence or who were assessed to have a violent disposition were registered. Non-PFU status is given to a patient who is assessed to have no risk of violence. If such a risk is assessed to be present, a patient is categorized as PFU (target) or PFU (subtarget), in increasing order of risk of violence. The present findings suggest that PFU status could indicate suicide risk instead of being merely a proxy to assess violence.
In the literature, hallucination is seldom regarded as a risk factor and may even be associated with a reduced suicide risk [5]. Previous findings, however, are not directly comparable to the present results because the present study includes both suicide completers and attempters as subjects of interest. A recent study found a positive correlation between attempted suicide and hallucination but recruited subjects with first-episode psychosis rather than first-episode schizophrenia [11].
In the present study 9% of subjects had ceased to take medication after an average of 2.6 years of follow up. Evidence-based literature offers no consensus regarding when antipsychotic medication could be discontinued. Local guidelines in Hong Kong also give recommendations based on clinical experience [14]. The present study indicated that continuing medication was associated with a reduced risk of suicidal behaviour. Given this finding, patients should be informed of the possible protective effect of continuing medication on suicide risk before deciding to discontinue antipsychotic medication.
It was a surprise to find that prescribing atypical antipsychotic medication reduced the risk of suicidal behaviour. Literature lends no strong support on ‘anti-suicidal’ effect in atypical antipsychotic medications apart from clozapine [15]. Psychiatrists’ prescribing practice could explain the findings. At EASY, conventional antipsychotic medications remain the first-line treatment for schizophrenia [14], with 73.5% (n=172) of subjects starting treatment with conventional antipsychotic medication. But by the end of follow up, 53% (n=124) were on atypical antipsychotic medication. The chance to receive atypical antipsychotic medication increased as the subjects received EASY follow up for a longer time. Because the time to event was shorter in the event cases (n=33) than in the censored cases, the suicidal subjects (n=33) would be less likely to receive atypical antipsychotic medication. The second possible explanation is the confounding effects of other variables in particular psychiatric symptoms. These variables, however, had already been controlled in multivariate analysis. Third, atypical antipsychotic medication is less likely to cause akathisia, which has been reported to increase suicide risk [16]. Although there was no difference in extrapyramidal side-effects between suicidal and non-suicidal subjects, it was possible that failure to recognize akathisia contributed to suicide. Fourth, there may be a genuine ‘anti-suicidal’ effect due to atypical antipsychotic medication. This hypothesized effect would best be investigated in a randomized controlled study, but ethical consideration would be a serious concern.
The limitations of retrospective cohort design include information bias and confounders. There are also three major limitations of case-note review: non-standardization, underreporting, and rater value judgement. First, the case notes were not originally prepared for research purposes and therefore might have problems of inconsistency and non-standardization. Second, negative entry of a particular variable on past records may be due to its true absence or to missing information. It is possible that certain information enquired about on the data retrieval form had not been regarded by clinicians as relevant to a particular subject and therefore did not appear in the case notes. Third, although a single rater was involved, he was not blinded to the outcome event while collecting the data. The rater's value judgement could result in observer bias.
Theses limitations were balanced against the virtue of the highly specialized service. Approximately two-thirds of the variables were crude and factual information that was gleaned from past records, while the proforma data retrieval form would likely minimize rater value judgement. It is not possible to blind the rater if longitudinal information such as time to event needs to be obtained. The difference between the suicidal and non-suicidal group was unlikely to be due to systematic bias because clinicians could not have known which patients would later deliberately harm themselves or commit suicide. Random bias resulting in false-positive findings is very unlikely because of the highly significant p.
This study had a large Type II error, especially in the analysis involving completed suicide (n=8), while Type II error was less of a problem in the analysis involving the combined group of deliberate self-harm and completed suicide (n=33). There were also limitations related to identification of event cases. For completed suicide it was possible that the treating staff might have overestimated the self-inflicted act as the cause of death, and thereby overestimate the rate of completed suicide. If an attempted suicide was not documented in the case notes, it could result in underestimation of deliberate self-harm. Among the subjects classified as inactive (n=27) who had been discharged from psychiatric service at the time of data collection, the author could account for only eight cases of completed suicide. The remaining 19 subjects could possibly develop suicidal behaviour subsequently. This could underestimate the rate of suicidal behaviour.
Clinicians working in early intervention programmes should be vigilant with regard to patients who pose a high suicide risk. The present findings are useful to the early intervention programme for psychosis in Hong Kong, because the risk factors so identified are locally specific and could be elicited easily in daily clinical practice. In the future, a prospective cohort study to identify risk factors for suicide in young Chinese people suffering from schizophrenia is recommended.
Footnotes
Appendix I. Independent variables
Age at time of entering EASY (continuous) Sex Marital status (single, married or divorced) Employment (student, unemployed, open-employment, supported-employment) Education (primary, F3, F5, F7, university/tertiary) Living (family, alone, others) Accommodation (public housing unit, private housing, village house, hostel) Family history of suicide Degree of relatives having history of suicide (primary, secondary, distant, no applicable) History of substance abuse Drinking history Past history of offence Type of offence (against person, against property, drug, not applicable) Medical history Clinical practice Number of admission to psychiatric ward at end of follow up or before outcome event ∗ (continuous) Input from clinical psychologist Input from occupational therapist Input from psychiatric day hospital Input from day engagement training Input from community psychiatric nurse Priority follow-up system (non-PFU, PFU-Target) Continuing prescription of drug at the end of follow up or before outcome event Medication prescribed at the end of follow up or before outcome event includes conventional antipsychotics Medication prescribed at the end of follow up or before outcome event includes atypical antipsychotics (excluding clozapine) Medication prescribed at the end of follow up or before outcome event includes long acting injectable antipsychotics Medication prescribed at the end of follow up or before outcome event includes mood stabilizers (including lithium) Medication prescribed at the end of follow up or before outcome event includes antidepressants Medication prescribed at the end of follow up or before outcome event includes lithium Medication prescribed at the end of follow up or before outcome event includes clozapine Presence of akathisia or recent prescription of propanolol (proxy) at the end of follow up or before outcome event Presence of extrapyramidal side-effects (apart from akathisia) or recent prescription of anticholinergics (proxy) at the end of follow up or before outcome event Psychiatric symptoms Secondary psychiatric diagnosis Past history of DSH prior to entering EASY Past history of DSH at the end of follow up or before outcome event Duration of untreated psychosis (continuous) Non-compliance Non-compliance and non-attendance more than 1 month Presence of delusion at the end of follow up or before outcome event Presence of hallucination at the end of follow up or before outcome event Presence of thought disorder at the end of follow up or before outcome event Presence of first rank symptoms of schizophrenia at the end of follow up or before outcome event Presence of affective blunting at the end of follow up or before outcome event Presence of agitation at the end of follow up or before outcome event Presence of perplexity at the end of follow up or before outcome event Presence of anxiety at the end of follow up or before outcome event Presence of depressed mood at the end of follow up or before outcome event Presence of suicidal ideation at the end of follow up or before outcome event Presence of feeling of hopelessness at the end of follow up or before outcome event Presence of loss of interest at the end of follow up or before outcome event Presence of loss of energy at the end of follow up or before outcome event Presence of negative symptom at the end of follow up or before outcome event
DSH, XXX; EASY, Early Assessment Service for Young People with Psychosis; PFU, priority follow up.