
Abstract
For approximately 20 years researchers have reported that gay, lesbian and bisexual young people are at an increased risk of depression and suicide. The 1989 Report of the Secretary's Task Force on Youth Suicide in the United States suggested that ‘gay youth’ were two to three times more likely to attempt suicide than other young people and that they ‘may comprise up to 30% of completed youth suicides annually’ [1, p.115]. Despite the debate and methodological issues linked to this report [2], more recent research with population-based samples has also concluded that gay, lesbian and bisexual youths, i.e. those adolescents attracted to the same and both sexes are at an increased risk of suicide and depression in New Zealand and the United States [3–6] and at increased risk of depression in Hong Kong [7]. Many studies have attributed the increased incidence of psychopathology in gay, lesbian and bisexual youth to environmental factors, in particular a milieu that is negative and unsupportive of these young people [4,6,8–11].
Few studies have investigated whether any differences in risk exist within the gay, lesbian and bisexual adolescent population or between youths attracted to the same sex and those attracted to both sexes. A literature search revealed that only a small number of surveys have published research in the area of sexual orientation and mental ill-health from nationally representative samples of adolescents. These are the survey series done under the umbrella of the National Longitudinal Study of Adolescent Health (AddHealth) from the United States [6], the Young in Norway Study [12] and Youth 2000 from New Zealand [13]. Furthermore, most research in the area of sexual orientation and suicidality or mental ill-health has relied on convenience samples of adolescents or has not included a comparison group of heterosexual young people [10]. In New Zealand there have been population-based publications from the Christchurch Health and Development longitudinal study [3] and from the Youth2000 survey series based on the 2001 survey [14], although the latter has not been reported in scientific journals.
The first nationally representative Youth2000 survey of New Zealand secondary school students conducted in 2001 indicated that almost one quarter of non-heterosexual or sexual minority students (i.e. those who reported being attracted to the same or both sexes, not sure of their sexual attractions or attracted to neither sex) reported significant depressive symptoms [14] and non-heterosexual orientation was associated with an increased risk of suicide [13]. Researchers from the Christchurch longitudinal study (which includes 28 people classified as being gay, lesbian and bisexual in a birth cohort of 1,265) concluded that gay, lesbian and bisexual young people are at increased risk of suicide and multiple psychiatric disorders compared with their heterosexual peers [3]. Neither of these studies investigated potential differences in findings between gay/lesbian and bisexual youths or patterns of help-seeking behaviour among these young people. Since the publication of the Christchurch longitudinal research in 1999 anecdotal reports suggest that adolescents are ‘coming out’ at a younger age than they did a decade or two earlier [15]. Coming out at an early age can lead to additional developmental challenges and younger adolescents may be less well equipped to deal with the societal stigma that is still associated with non-heterosexual orientation. Coming out can lead to a reduction in an adolescent's social support [11]; supports that are thought to be protective against suicidality [2].
In this study our aim was to determine whether secondary school students in New Zealand who are attracted to the same or both sexes or who are not sure of their sexual attractions differ, in regard to their risk of self-harm, suicide and depression compared to those who are attracted to the opposite sex. We have investigated differences in help-seeking behaviour between students who were not exclusively opposite-sex attracted to those who were. We hypothesized that we would replicate earlier findings that students who were not heterosexual or opposite-sex attracted would report increased rates of self-harm, suicide and depression. We also hypothesized that those who were attracted to the same sex would be at the greatest risk for adverse outcomes and that those who were not exclusively opposite-sex attracted would find it harder to access help for an emotional worry than those who were attracted to the opposite sex.
Method
We have used data collected in Youth’07, the second Youth 2000 national cross-sectional population-based youth health and wellbeing survey conducted in New Zealand. The study method of Youth’07 is described in detail elsewhere [16]. In summary, 9,107 randomly selected secondary school students completed the survey, accounting for 3.4% of the total 2007 secondary school roll in New Zealand. Response rates for schools and students were 84% and 74% respectively. The anonymous comprehensive 622 item survey was administered using Internet tablets (hand-held computers) [17]. Written consent was required from each participating school and each student provided their consent before being able to access the Youth’07 survey questionnaire. Ethics approval was gained from the University of Auckland Human Subjects Ethics Committee.
Sexual orientation was measured by the question: ‘Which are you sexually attracted to?’ Analyses primarily categorized students into five sexual attraction groups; those attracted to the opposite sex, the same sex, both sexes, those not sure and those attracted to neither sex as it was hypothesized that there were meaningful differences in mental health outcomes between each of the groups.
Measures
Demographic information
Participants identified whether they were male or female. There were no question options that allowed participants to identify gender diversity (such as being transgendered). The number of participants by age for certain sexual attraction groups was small, so age was categorized as ‘15 or less’ or ‘16 or older’. Participants were asked to identify the ethnic groups which they identified with, based on the New Zealand Census standard 2001/2006 ethnicity question [18]. Those students who chose more than one ethnic group were assigned a single ethnic group using the Statistics New Zealand ethnicity prioritization method [19]. For data analyses ethnicity was grouped: New Zealand European, Māori, Pacific, Asian and Other. Socioeconomic deprivation of each student's area of residence was measured using the New Zealand Deprivation Index (NZDep2006) [20]. NZDep2006 combines eight dimensions of deprivation derived from the NZ census and assigns each census area unit a deprivation decile (a decile of 1 represents areas with the least deprived scores and 10 represents areas with the most deprived scores). For data analyses students were grouped into one of three decile bands; indicating low (deciles 1 to 3), medium (deciles 4 to 7) and high (deciles 8 to 10) levels of socioeconomic deprivation.
Awareness of same-sex attraction and coming out
The possible responses to ‘How old were you when you became first aware of your sexual attractions to people of the same sex?’ were aggregated to ‘11 or less’, and ‘12 or older’. Students attracted to the same or both sexes were also asked ‘Have you come out (told people close to you openly of your sexuality)?’ Those that gave an affirmative response were classified as ‘students who have come out’.
Depression
‘Significant depressive symptoms’ were identified by scores greater than 28 on the Reynolds Adolescent Depression Scale, Short Form (RADS-SF). This score was based on the analysis of the 2001 survey data, which showed that a level of 28 best matched the cut-off of the full Reynolds Adolescent Depression Scale and gave closer agreement than the lower recommended RAD-SF cut-off level of 26 in the percentage classified with significant levels of depressive symptoms [21].
Self-harm
Deliberate self-harm was defined as an affirmative response to the question “In the last 12 months, have you ever deliberately (on purpose) hurt yourself or done anything you knew might have harmed you or even killed you?”
Suicidality
Suicidal ideation was identified by an affirmative response to the question ‘During the last 12 months have you seriously thought about killing yourself (attempting suicide)?’ Suicide attempts were identified by an affirmative response to the question ‘During the last 12 months have you tried to kill yourself (attempt suicide)?’.
Help-seeking
Accessing help from a health professional for emotional worries was identified by an affirmative response to the question ‘In the last year, have you ever seen a health professional such as a doctor, nurse or school guidance counsellor for emotional health worries?’ Having difficulty accessing help was defined by a student selecting ‘an emotional worry’ in response to the question, ‘In the last 12 months have you had any difficulty getting help for any of the following?’ (‘An emotional worry’ was one of 10 responses).
Analysis
Students were recruited using a two-stage clustered sample design with unequal probabilities of selection. In all analyses the data have been weighted by the inverse probability of selection, and the variance of estimates was adjusted to allow for correlated data from the same schools. Total numbers and adjusted percentages were calculated for the selected health behaviours or outcomes. Multiple logistic regression models, including the possible confounders of age, sex, ethnicity and level of neighbourhood socioeconomic deprivation, were used to investigate the associations between sexual attraction and the health behaviours and health outcomes. The interaction between sexual attraction and sex was tested for each outcome or health behaviour and where this interaction was significant, analyses were stratified by sex. Because of the number of very small cell sizes for the analyses testing the associations between sexual attraction and help seeking behaviour, those who were attracted to the same or both sexes, not sure of their sexual attractions or attracted to neither sex were combined into a single category (‘not exclusively opposite-sex attracted’). All analyses were carried out using SAS software version 9.1 (2004) using the survey procedures.
Results
In total, 8,002 students (88%) answered the question on sexual attraction. Of those who did not respond to this question 117 (1%) declined to answer the question; 550 (6%) skipped the entire sexual health section; and 438 (5%) had quit the survey before reaching this question. Responders to the sexual attraction question appeared similar to the total sample surveyed in Youth’07 (Table 1).
Characteristics of responders to the sexual attraction question compared to the overall sample
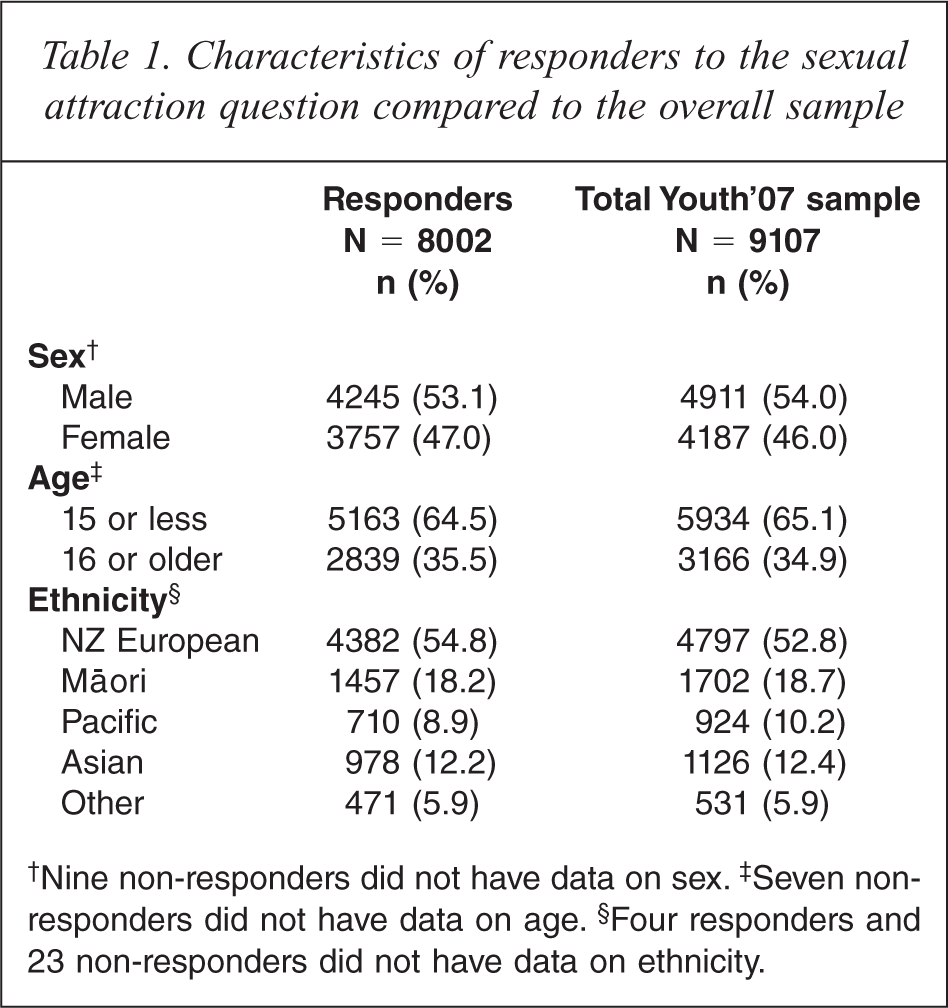
†Nine non-responders did not have data on sex.‡ Seven non-responders did not have data on age.§ Four responders and 23 non-responders did not have data on ethnicity.
The distribution of students by sexual attraction was broadly similar across age groups, sex and ethnicity, although numbers of respondents in some categories were small (Table 2). Most of the students attracted to the same sex and both sexes were not aware of their same-sex attraction at age 11 or less (Table 2). At the time of completing the survey approximately a third of students attracted to the same sex (23 of the 73) and less than half of those attracted to both sexes (111 of the 270) had come out.
Characteristics of students by sexual attraction
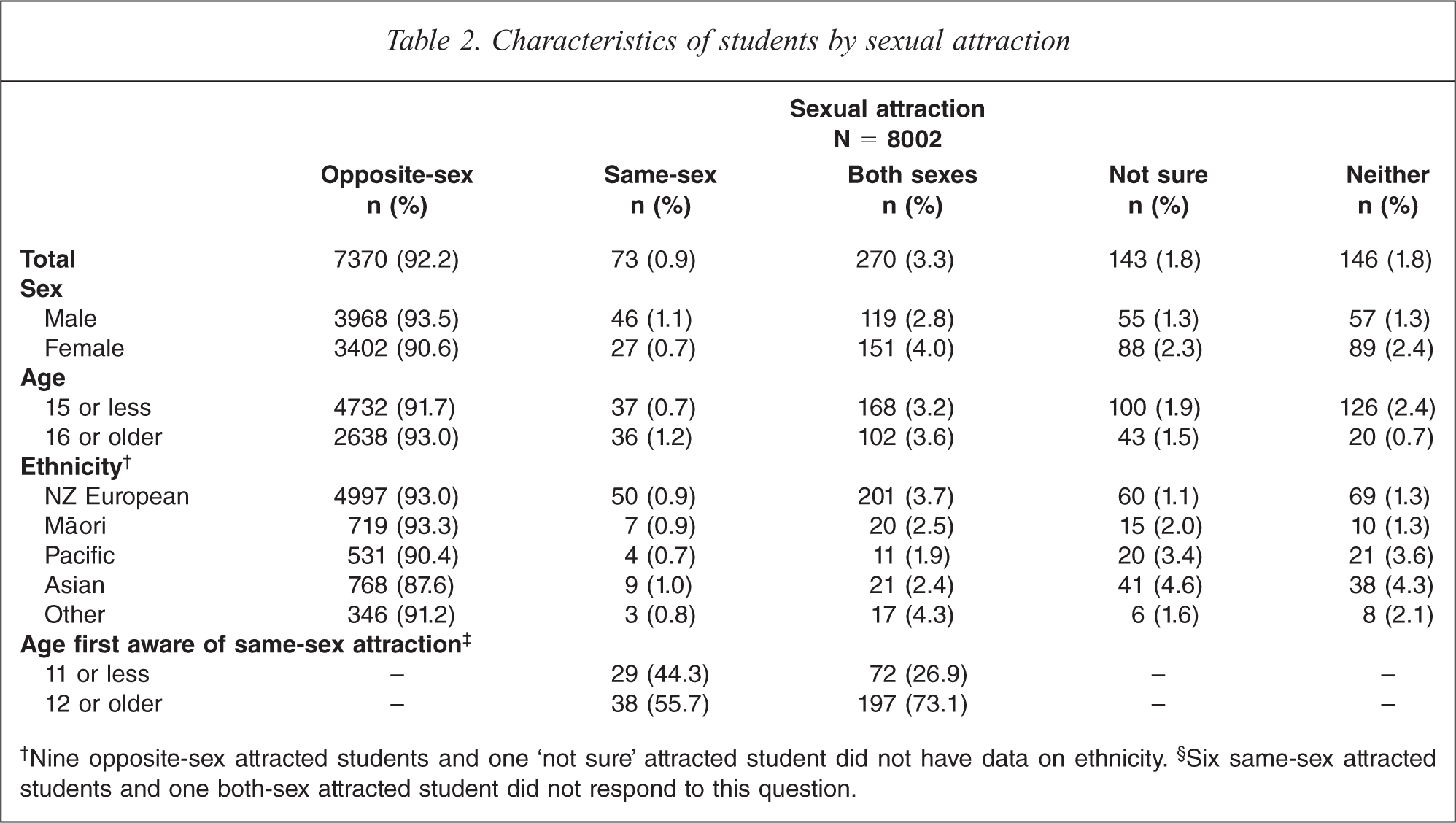
†Nine opposite-sex attracted students and one ‘not sure’ attracted student did not have data on ethnicity.§ Six same-sex attracted students and one both-sex attracted student did not respond to this question.
There were significant associations between sexual attraction and the risk of self-harm, suicidality and significant depressive symptoms with students attracted to both sexes at greatest risk and those attracted to the opposite sex or to neither sex at the least risk (Table 3). Students who reported being attracted to the same sex and those not sure of their sexual attraction had higher odds of significant depressive symptoms, self-harm and suicidality, whereas students attracted to neither sex had lower or broadly equivalent odds compared to students attracted to the opposite sex. The association between sexual attraction and having seriously thought about suicide was different for males and females, with males broadly following the pattern described above. However amongst females only those attracted to both sexes had considerably increased odds of serious suicidal thoughts. There was no significant interaction between sex and sexual attraction for self-harm, suicide attempts and significant depressive symptoms.
Associations between sexual attraction and depression, self-harm and suicidality
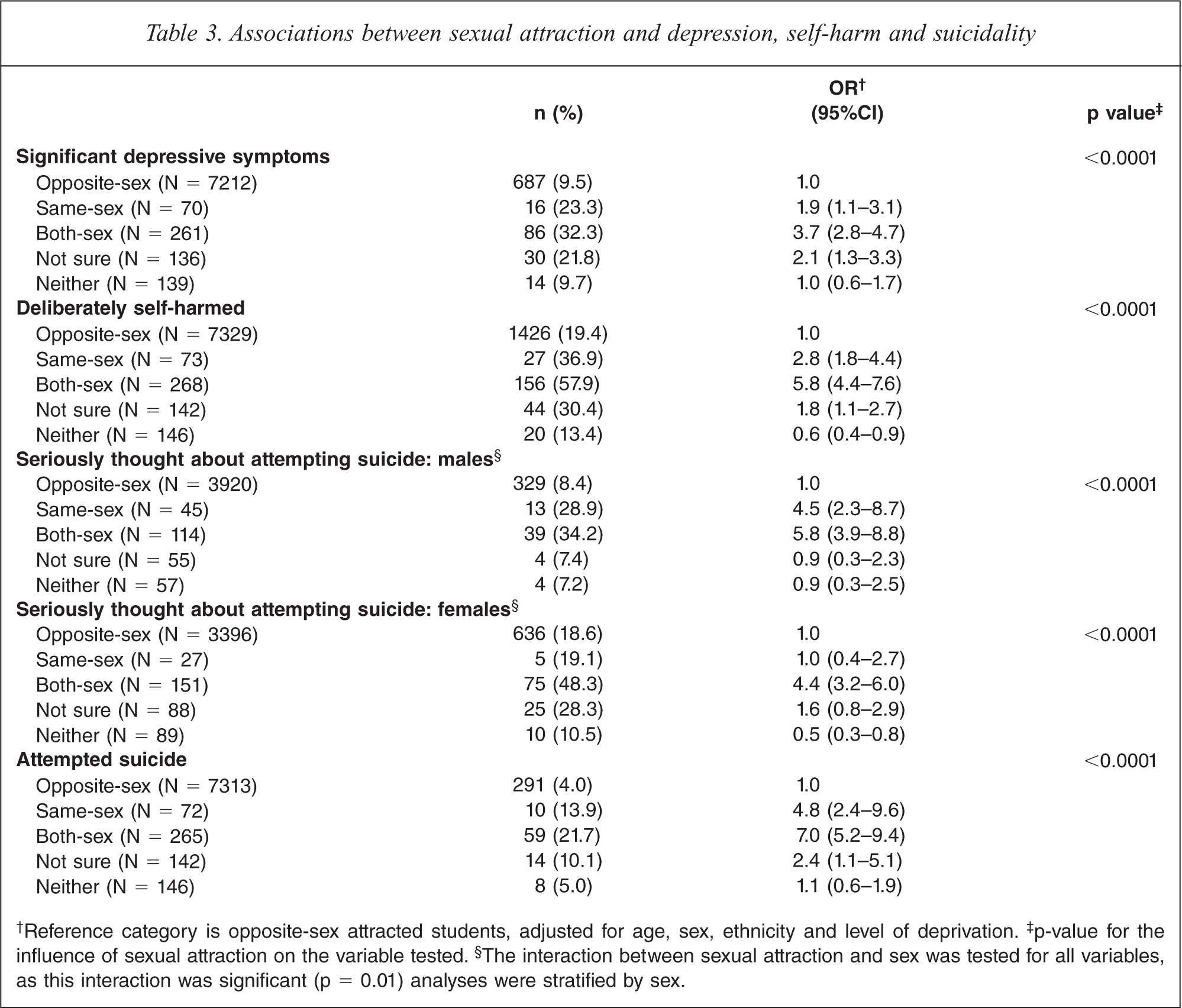
†Reference category is opposite-sex attracted students, adjusted for age, sex, ethnicity and level of deprivation.‡ p-value for the influence of sexual attraction on the variable tested.§ The interaction between sexual attraction and sex was tested for all variables, as this interaction was significant (p = 0.01) analyses were stratified by sex.
There were significant interactions between sexual attraction and sex for having seen a health professional for emotional worries (p = 0.02) and having had difficulty getting help for an emotional worry (p = 0.004) (Table 4). The interaction effect was related to the magnitude of the effect, as not exclusively opposite-sex attracted males and females both reported more help-seeking behaviour and difficulties getting help for an emotional worry compared to their opposite-sex attracted peers, but these differences were more pronounced in males (for example OR 2.9 compared to 2.1 and 3.7 compared to 1.8) (Table 4).
Associations between sexual attraction and help-seeking
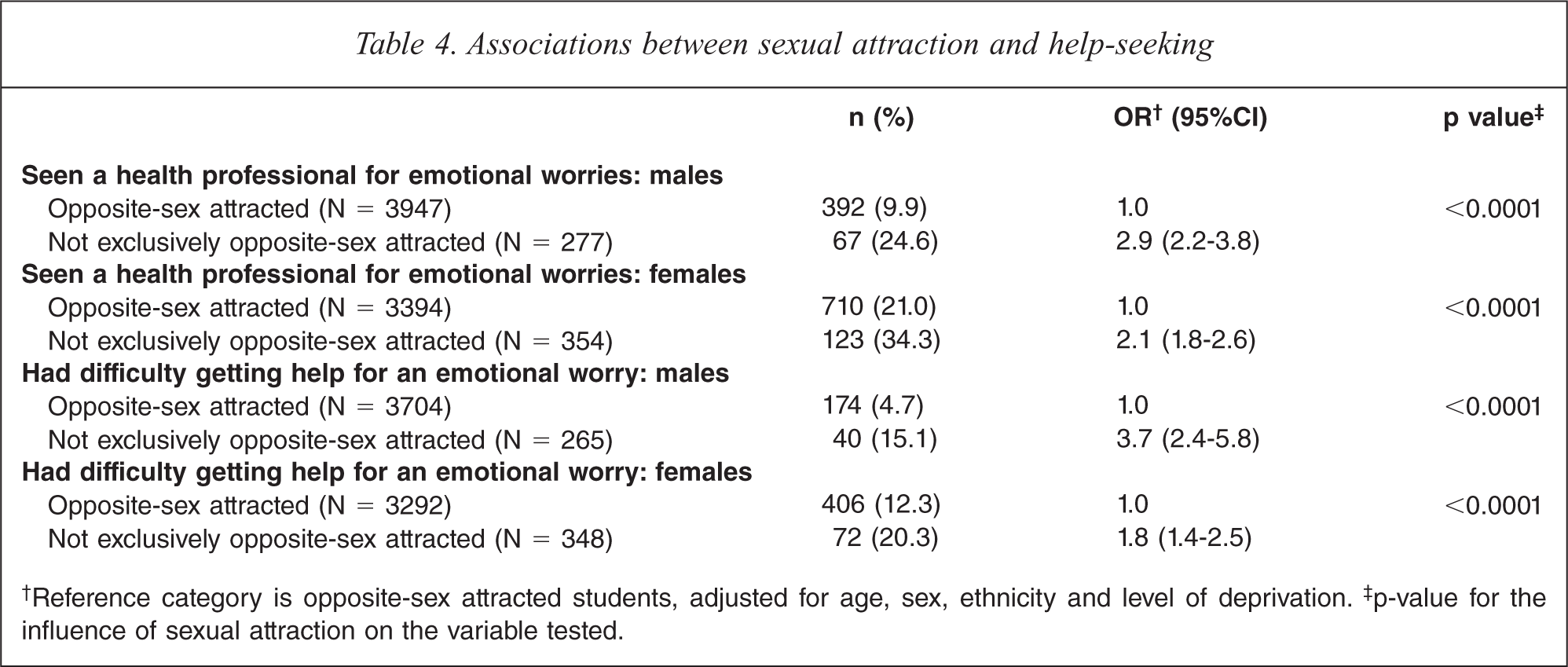
†Reference category is opposite-sex attracted students, adjusted for age, sex, ethnicity and level of deprivation.‡ p-value for the influence of sexual attraction on the variable tested.
Discussion
Summary of main findings
We have investigated sexual orientation and its associations with depression, self harm, suicidality and help-seeking behaviour in a large national survey of secondary school students in New Zealand. Most of the same- and both-sex attracted students surveyed in Youth’07 were not suicidal and did not have significant depressive symptoms. However, we showed that students who were attracted to both sexes, the same sex and were not sure of their sexual attractions were at increased risk of self-harm, depression and suicide when compared to their straight or opposite-sex attracted peers. Students who were not exclusively opposite-sex attracted were also more likely to have seen a health professional for emotional worries and to have more difficulty getting this help. This is in line with previous research that has shown that although the majority of gay, lesbian and bisexual adolescents will grow up to lead happy, healthy, productive lives [2] they are at greater risk of self-harm, depression and suicide [3,13].
Only a small proportion of students reported that they were sexually attracted to the same sex (0.9%), with nearly four times that many responding that they were sexually attracted to both sexes (3.3%). These figures are in line with large scale studies of high school students in North America [22,23]. To the best of our knowledge only three nationally representative survey series in the United States, Norway and New Zealand have investigated the prevalence of adolescent sexual orientation and mental health outcomes [6,12,14].
With increasing age the proportion of students not sure of their sexual attractions decreased, and few students attracted to the same or both sexes reported that they were aware of their same-sex sexual attractions before the age of 11, indicating that adolescence is a time when young people are making sense of their sexuality [11]. Over 60% of students attracted to the same or both sexes had not ‘come out’ [24]. This is not surprising as most students were aged 15 years or less, at the time of completing the survey. However, the 134 students who were out, are potentially at risk of chronic stress, including verbal and physical abuse from both peers and adults [10] as gay and lesbian students tend to report elevated rates of victimization and homophobic bullying from their peers at school [9].
To date studies examining the associations with adverse mental health outcomes and sexual orientation have grouped gay, lesbian and bisexual young people together [3,7,25]. This may be because of small samples or may reflect an assumption on the part of the researcher that an adolescent's report of bisexuality is a precursor to a gay or lesbian identity [23]. In this study, where students who reported different sexual attractions were maintained as separate groups, we found that students attracted to both sexes were at greater risk of depression and suicide than students attracted to the same sex. Nearly a third of the students attracted to both sexes reported significant depressive symptoms and more than 20% had attempted suicide in the previous 12 months. More than half of students attracted to both sexes had deliberately self-harmed in the previous 12 months, however caution is required when interpreting this result as it was not possible to ensure that the students’ intentions were self-inflicted harm from the single item used. We were unable to explore the reasons for this increased risk, but it has been suggested that it may be symptomatic of a personal struggle related to managing an identity that is not as clearly defined as being gay/lesbian/same-sex attracted or straight/opposite-sex attracted [26]. In addition, being attracted to both sexes may result in marginalization in both heterosexual and gay or lesbian networks.
Our results contrast with two recent population-based studies from North America in which young people who were less certain of their sexuality or were ‘sexually questioning’ are at greater risk of depression or suicide when compared to their gay, lesbian, bisexual or heterosexual peers [27,28]. In our study students who were not sure of their sexual attractions or were attracted to neither sex were at decreased risk relative to students attracted to both sexes.
Strengths and limitations
This survey includes data from a large nationally representative sample of secondary school students from throughout New Zealand. A reliable and valid instrument for assessing depression was used and the survey as a whole had been subjected to extensive pilot and field testing prior to Youth’07 being conducted. We are not aware of comparable analyses examining the mental health of students attracted to the same and both sexes in Australasia.
There are some limitations. The survey is of secondary school students so the findings cannot be generalized to all New Zealand adolescents. Because students could only select that they were either male or female it was not possible to explore the role of gender diversity (i.e. whether students were transgendered or intersex) in the context of sexual attraction. There were no questions addressing sexual identity and sexual behaviour could not be established, so sexual attraction was used as a proxy measure of sexual orientation. However, a review of eight school-based adolescent health surveys in North America recommends using a sexual attraction question, especially if the survey includes younger adolescents [29]. The review also found that adolescents appeared to be less willing to disclose a ‘stigmatized sexual identity’, even in anonymous and confidential surveys, than they were to disclose sexual attractions and sexual behaviours [29]. Finally, not all students completed all sections of the survey questionnaire. Some areas, particularly in the later sections of the Youth’07 questionnaire had missing data. This may be because the sexual health questions came towards the end of the questionnaire, as the twelfth of fifteen topic sections the questionnaire included.
Conclusion
Few secondary school students report that they are attracted to the same or both sexes but those who did reported an increased risk of depression, self-harm and suicidality and they experienced more difficulty getting help for an emotional worry. Health professionals need to create environments where adolescents can talk openly about sexual attractions and they should screen for symptoms of depression and self-harm in students reporting that they are attracted to the same or to both sexes. Health professionals also need to work towards creating a milieu that is accepting and supportive of students that are not exclusively opposite-sex attracted.
Footnotes
Acknowledgements
The authors would like to thank the schools and students that participated in Youth'07.
Everyone who contributed significantly to this study has been named as an author on this manuscript. The authors alone are responsible for the content and writing of the paper.