
Abstract
Introduction
Aggression is a serious issue in psychiatric inpatient facilities and can threaten patient and staff safety and negatively impact on the therapeutic milieu of the inpatient unit. Aggressive behaviour is not only common during admission to adolescent psychiatric inpatient facilities (Dean et al., 2007; Greene et al., 2006) but is also often the reason for referral of young people to youth mental health services (Connor et al., 1998). In the literature, aggression has been defined as “a bodily response with the intended infliction of bodily harm” (Glasser, 1998: 887). The current research addressed the distinction between aggression involving violence towards others, including property destruction, and acts of aggression towards oneself, also referred to as self-harming behaviour.
Identifying patients that are at high risk of committing aggressive acts is critical in successfully managing aggressive behaviour in adolescent inpatient units. Consequently, mental health professionals are required to conduct regular risk assessments as part of hospital policy. Risk assessment is the evaluation of the likelihood that an individual will become aggressive and contributes to the subsequent development of interventions to manage or reduce the likelihood of aggression (Monahan, 1995).
The development of aggression risk assessment tools has for the most part been in adult samples. While there is growing empirical evidence on risk factors for aggression in youth, very few risk assessment measures have been developed for this age group, often resulting in the use of adult tools in young populations. As such, it is not surprising that unstructured clinical methods of risk assessment, that is, a judgement made by the clinician based on their knowledge of the client’s history, expertise, prior experience and intuition, remain the preferred method in clinical practice in adolescent settings.
It is important that the risk factors and information in aggression risk assessments are tailored and relevant to young people to provide an accurate indication of risk for the individual. While there tends to be some overlap with respect to the risk factors associated with adolescents who engage in other-directed aggression and those who engage in self-directed aggression (Becker and Grilo, 2007), differences in the clinical factors that predict self- and other-directed aggression in the adolescent psychiatric population have been found (Vivona et al., 1995). A prior history of other-directed aggression is the single best predictor for future aggression in youth (Borum, 2000). This finding has also been documented in adolescent inpatient samples (Dean et al., 2007). Similarly, a history of self-harm has been found to predict future engagement in self-directed aggression in adolescents with major depressive disorder (Wilkinson, 2011). However, whilst male sex has been found to be predictive of other-directed aggression (Becker and Grilo, 2007; Fryer et al., 2004), female sex has been found to be associated with self-harm in young inpatient samples (Becker and Grilo, 2007). Although diagnosis as a risk factor for aggression has been deemed inconclusive in some studies (Dean et al., 2007), a diagnosis of depression has been found to be associated with self-directed aggression in adolescent inpatients (Becker and Grilo, 2007).
The aim of this study was to examine the predictive validity of unstructured clinical risk assessment in adolescent inpatients by retrospectively examining the association between risk assessment rankings assigned by psychiatric staff on admission and subsequent incidents of self- and other-directed aggression recorded in critical incident reports by nursing staff occurring within the first 4 weeks of inpatient stay. Additional risk factors for aggression were also assessed including sex, history of physical aggression and self-harm, and diagnosis to determine whether unstructured clinical risk ratings were more predictive of engagement in aggression than certain risk factors alone.
It was hypothesised that higher risk ratings for aggression and self-harm would be associated with a higher frequency and severity of aggression and self-harming behaviour in the first 4 weeks of inpatient stay. In addition to the risk assessment rating, it was also hypothesised that a history of physical aggression would be associated with more frequent and severe aggression, and a history of self-harm and female sex would be associated with more frequent self-directed aggression in the first 4 weeks of admission.
Method
Ethics approval was obtained from Austin Health and La Trobe University. The study was conducted at the Marian Drummond Adolescent Unit (MDAU). The MDAU is a 12-bed inpatient unit at the Austin Health Child and Adolescent Mental Health Service in Melbourne, Australia providing short- to medium-term assessment and treatment for adolescents with serious psychiatric, behavioural and emotional disturbances.
A file audit of admissions for the period September 2006 to July 2009 was conducted at the MDAU examining unstructured clinical risk assessment practices. Inclusion criteria required children to be aged 13–18 years. Demographic and clinical information and admission risk assessment ratings were accessed from the medical files and databases. History of self-harm was coded in three levels: absence of self-harming; self-harm ideation only; or self-harming act. History of aggression was re-coded into a dichotomous variable defining the presence/absence of a history of physical aggression towards others (excluding property damage) in response to the very low frequencies of patients with a history of verbal or property damage only. Risk assessment ratings were based on the subjective unstructured clinical judgement of the adolescent psychiatrist or the psychiatric registrar. Generally, the psychiatrist was informed by varying degrees of referral information and pre-admission assessment, which included a structured form to record presenting history including history of aggression, suicidal behaviour, self-harm, juvenile justice, involuntary admissions, family history of aggressive behaviour and any current criminal charges. Risk rankings consisted of four levels: low, medium, high and very high risk.
Episodes of aggression occurring within the first 4 weeks of inpatient stay were recorded from critical incident reports containing information on the date, nature of aggression and intervention response. Frequency of aggression (towards staff, other patients or property) and self-harm were assessed by the number of times a patient engaged in aggression or self-harm. Episodes of other-directed aggression that occurred during the study period were then assessed for severity. The severity of aggression for any one incident was determined as not being severe if MDAU staff were able to manage the child, and severe if MDAU staff required the assistance of staff external to the unit to contain the patient. As a result, severe aggression was typically physical in nature. Severity of aggression was dichotomously coded as no severe aggression (absence of severe aggression) and severe aggression (one or more incidents of severe aggression). This decision was made on the basis that there were very low frequencies of patients who engaged in one or more episodes of severe aggression and allowed for adequate expected cell frequencies for chi-square and logistic regression analyses.
Data were analysed using Windows SPSS Version 16.0. The data were screened and descriptive statistics were explored. Risk factors associated with aggression were identified by correlation and chi-square analyses. Non-parametric Spearman rank correlation was conducted in response to non-normally distributed data and the ordinal nature of the risk assessment rankings. Dichotomous dummy variables were coded for each of the eight diagnostic categories and the three levels of the history of self-harm variable. Binomial logistic regressions were performed to investigate whether the identified risks and the risk assessment rankings were predictive of engagement in aggressive behaviour in the first 4 weeks of admission. An error rate of alpha = 0.05 (two-tailed) was set to determine statistical significance.
Results
A total of 197 adolescents were admitted to the MDAU during the study period. Of these, three patients were excluded because of incomplete risk assessments. A further patient was excluded owing to being discharged on admission. The ages of the remaining 193 adolescents ranged from 13 to 18 years (mean = 15.46, SD = 1.25). The sample was predominantly girls (77.2%) and comprised primarily of crisis admissions (82.9%). The mean length of stay was 28 days (range = 1–172 days).
Table 1 illustrates that the majority (82.4%) of adolescents were classified as low risk for aggression. Few (10.9%) were aggressive with only nine of these patients engaging in severe aggression. Over half (64.2%) of adolescents were classified as moderate risk for self-harm. The proportion of patients who engaged in self-harm was low with 31 (16.1%) patients self-harming. A history of aggression in the unit was rare (14.0%); however, the majority of adolescents had previously self-harmed (75.1%).
Frequencies and percentages of risk assessment rankings, self- and other-directed aggressive incidents in the first 4 weeks of admission, and history of aggression and self-harm for adolescent inpatients.
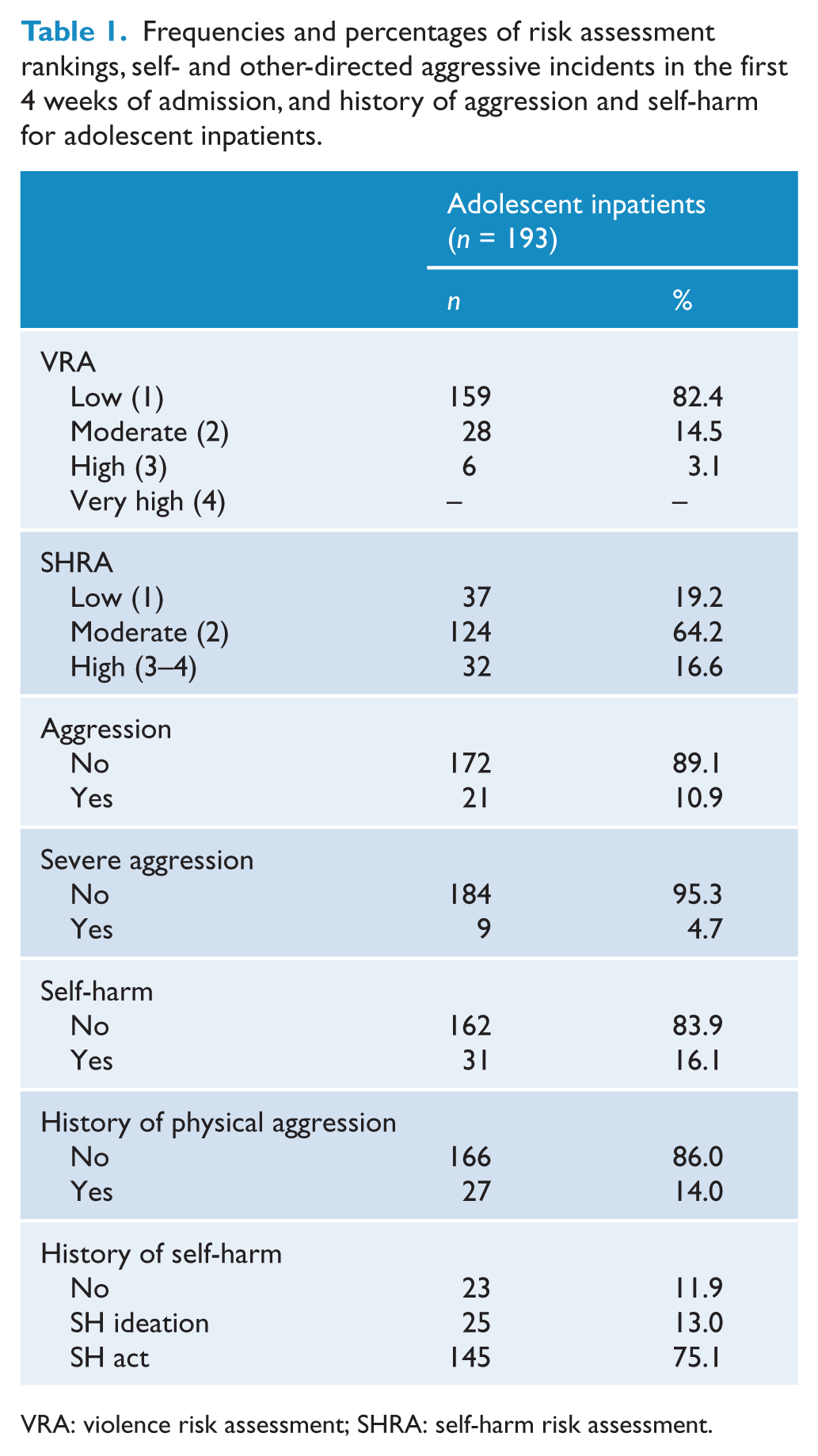
VRA: violence risk assessment; SHRA: self-harm risk assessment.
Primary diagnoses were reduced to eight categories according to the DSM-IV (American Psychiatric Association, 1994): mood disorders (depression, dysthymic disorder, cyclothymic disorder, bipolar disorder and unspecified mood disorder); anxiety disorders (generalised anxiety disorder, separation anxiety, anxiety disorder not otherwise specified, mixed anxiety depressive disorder, acute stress disorder, social phobia, specific phobia, obsessive compulsive disorder, and post-traumatic stress disorder); adjustment disorder; disruptive behavioural disorder (oppositional defiant disorder); relationship disorders (parent–child relationship disorder and attachment disorder); psychotic disorders (schizophrenia, schizophreniform disorder and schizoaffective disorder); developmental disorders (pervasive development disorder not otherwise specified and autism); and eating disorders (anorexia nervosa and eating disorder not otherwise specified). Two cases with a primary diagnosis of somatoform disorder not otherwise specified and one case with borderline personality disorder could not be classified into the above diagnostic categories and were removed from further analyses that examined primary diagnosis.
The proportion of adolescents who engaged in self-, other-directed, and severe aggression for each primary diagnostic category was explored. Table 2 indicates that the majority of adolescents with mood disorder were not aggressive (94.1%) and did not engage in severe aggression (98.0%). Patients with adjustment disorder and relationship disorder were the most likely to become aggressive followed by those diagnosed with a psychotic disorder. Two patients (22.2%) with adjustment disorder and four patients (19.0%) with a psychotic disorder engaged in severe aggression. Adolescents diagnosed with adjustment disorder were also likely to self-harm with one-third (33.3%) of these patients self-harming.
Frequencies of self- and other-directed aggression and severity of aggression in adolescent inpatients by primary diagnosis.
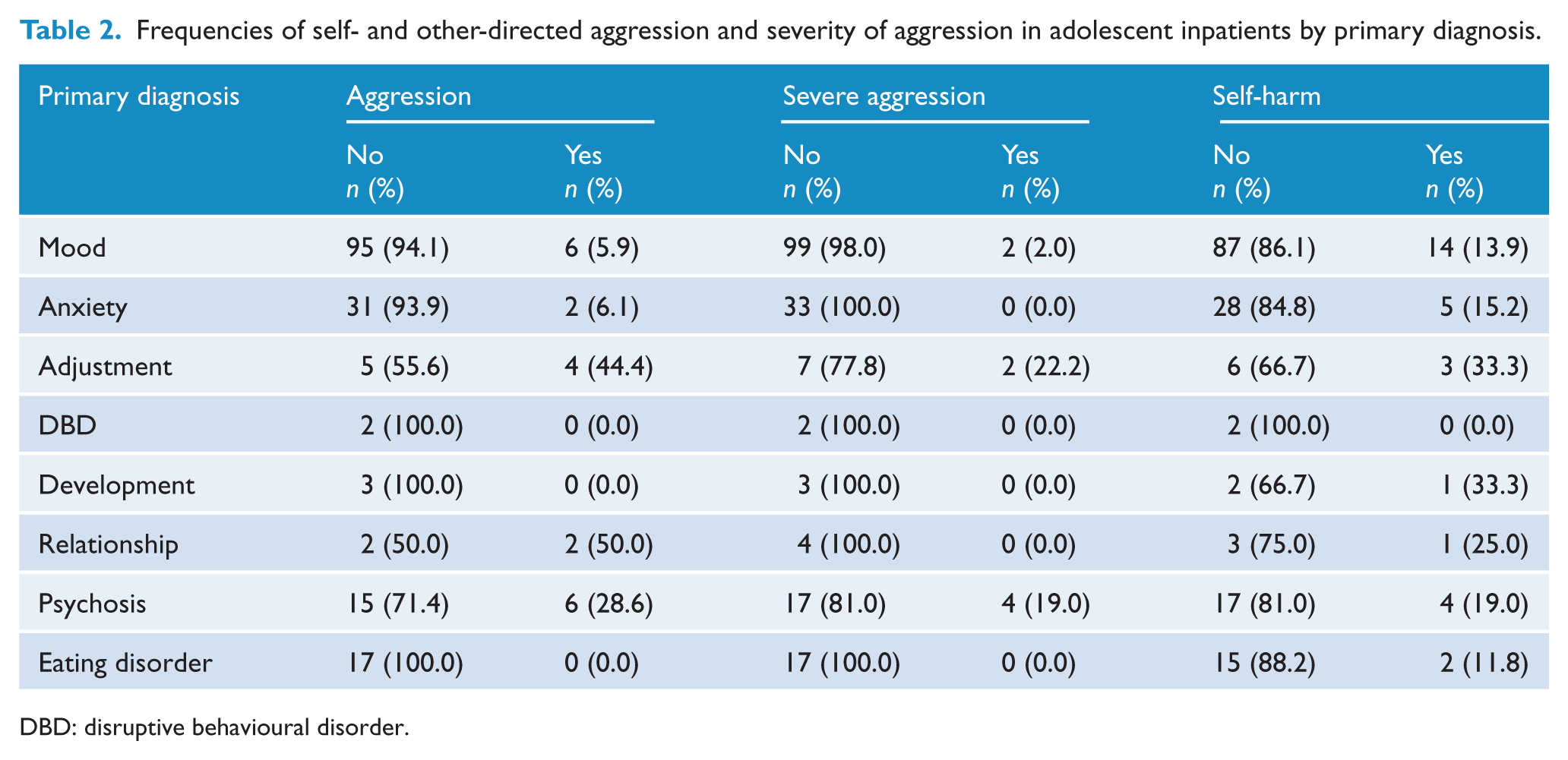
DBD: disruptive behavioural disorder.
Low, significant, positive correlations were found between episodes of aggression and the risk assessment, history of aggression, adjustment disorder, relationship disorder and psychotic disorders, indicating that high risk assessment scores and the presence of these predictor variables were associated with aggressive behaviour. Low, significant, negative correlations were found between aggression and mood disorder, indicating that the presence of a primary diagnosis of mood disorder was associated with less frequent aggression. Low, significant, positive correlations were found between severe aggression and the risk assessment, history of aggression, adjustment and psychotic disorders, indicating that higher risk assessment ratings and a presence of these variables were associated with severe aggression. No significant correlations were found between engagement in aggression or severe aggression and sex. The self-harm risk assessment was not correlated with self-directed aggression; however, the variables of sex, and history of self-harm ideation and act were significant, indicating that female sex and a history of self-harm were associated with engagement in self-harm.
Chi-square analyses confirmed that the risk assessment remained significant with other-directed aggression (Fisher’s exact test, p = 0.00) as did history of aggression (Fisher’s exact test, p = 0.00), mood disorder χ2 (1, n = 193) = 4.32, p = 0.04, adjustment disorder (Fisher’s exact test, p = 0.01) and psychotic disorder (Fisher’s exact test, p = 0.02). Relationship disorder did not remain significant. Owing to the low number of adolescents engaging in severe aggression, this variable was not assessed beyond correlation analyses as the assumption of expected cell frequencies for chi-square and logistic regression analyses were violated. The self-harm risk rating was not significant with engagement in self-directed aggression following chi-square analyses; however, it was included in regression analyses to address the hypothesis of this study. Sex χ2 (1, n = 193) = 4.56, p = 0.03, history of self-harm ideation (Fisher’s exact test, p = 0.02) and history of self-harm act χ2 (1, n = 193) = 5.59, p = 0.02 remained significant with engagement in self-harm.
Binomial logistic regressions assessed the extent to which risk assessment ratings predicted engagement in aggressive behaviour in the first 4 weeks of admission. Results are displayed in Table 3. Variables assessed for predictive validity of frequency of aggression represented a significant model, χ2 (3, n = 197) = 24.78, p = 0.00, and accounted for between 12.0% and 24.2% of the variability in aggression. The predictor variables adjustment disorder and psychotic disorder were removed from the regression analysis as they were not found to significantly contribute to the variability in aggression. The model correctly identified 98.3% of children who did not engage in aggression and 23.8% who did engage in aggression. As can be seen by the negative B value in Table 3, a primary diagnosis other than mood disorder was the strongest predictor of aggression and the odds ratio indicates that those with a primary diagnosis of a mood disorder were approximately 4.2 times less likely to become aggressive. The violence risk assessment was the next strongest predictor, indicating that those with higher risk assessment ratings were 3.83 times more likely to become aggressive. History of aggression was also significant and the odds ratio indicated that adolescents with a history of aggression were 3.88 times more likely to become aggressive.
Direct logistic regression analysis of all adolescent inpatient presentations predicting engagement in other-directed, severe and self-directed aggression.
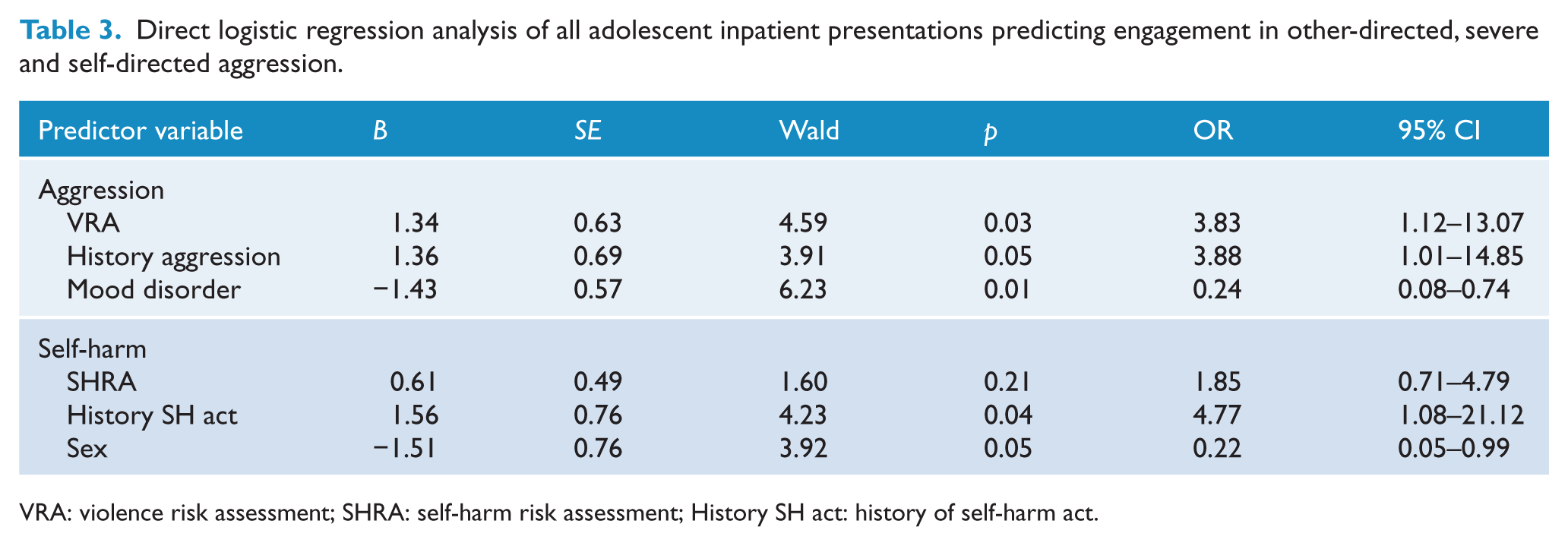
VRA: violence risk assessment; SHRA: self-harm risk assessment; History SH act: history of self-harm act.
Variables assessed for predictive validity of self-harm represented a significant model, χ2 (3, n = 197) = 15.38, p = 0.00; however, they only accounted for between 7.7% and 13.1% of the variability in self-harm. The self-harm risk assessment was not a significant predictor of self-harm; however, history of a self-harm act was the strongest predictor, indicating that adolescents with a history of a self-harming act were 4.77 times more likely to engage in self-harm. The predictor variable history of self-harm ideation was removed from the regression analysis as it was not found to significantly contribute to the variability in self-directed aggression. Sex also made a significant contribution to the model, indicating that females were 4.5 times more likely to engage in self-harm.
Discussion
Research on risk assessment practices and the prediction of aggression and self-harm in the young psychiatric inpatient population is relatively limited. Results of this study provide partial support for the predictive validity of unstructured clinical risk assessment of self- and other-directed aggression in an Australian adolescent psychiatric inpatient unit. The use of unstructured clinical risk assessment measures of other-directed aggression in this population was supported. However, in line with previous research (Apperson et al., 1993; McNiel and Binder, 1991), the association between the risk assessment rankings and engagement in other-directed aggression was moderate. Correlations were relatively low and the amount of variance in aggression accounted for by the risk assessment rankings was relatively small. This result was also found in the child inpatient unit at the same facility (Phillips et al., 2011). Nevertheless, as with the child unit (Phillips et al., 2011), results of this research suggest that unstructured clinical risk assessment is a better indication that an individual will engage in other-directed aggressive behaviour than a prior history of physical aggression alone. The severity of aggression could not be analysed by way of multivariate analyses because of the small number of adolescents who engaged in severe aggression during the study period. Nevertheless, correlational analyses suggested a relationship between the risk assessment and episodes of severe aggression.
The results of this study did not support the use of unstructured clinical risk assessment measures of self-directed aggression in adolescent inpatient units. The current findings therefore indicate that although clinicians are relatively good at predicting patient engagement in aggression, their ability to predict engagement in self-harm is less reliable when relying on unstructured clinical judgement. It could be argued that both other-directed aggression and self-harming behaviours are somewhat dependant on environmental and contextual factors but the difference in the predictive ability of the regression equations suggests that self-harming behaviour may be even more so. It is possible that once admitted to the inpatient facility, contextual triggers were removed from the high-risk individual’s environment and self- harming behaviour decreased as a consequence. In addition, self-harm is sometimes a learnt behaviour in adolescent psychiatric settings. That is, patients pick up self-harming behaviours from their inpatient peers during admission. This may explain the proportion of adolescent inpatients that were classified as low risk for self-harm on admission yet engaged in self-harming behaviour. Furthermore, high-risk patients are managed differently to low-risk patients and generally are provided a greater level of supervision, higher levels of medication to manage distress, or admission to the high-dependency section of the unit. As such, the opportunity to self-harm is diminished in these patients.
These findings present important implications for the use of unstructured clinical risk assessment methods of self- and other-directed aggression and the risk factors to be considered when assigning risk in clinical practice. A history of self-harming was the best indication that a patient would engage in self-directed aggression followed by female sex. Whist these findings are consistent with the literature (Becker and Grilo, 2007; Wilkinson, 2011), it was expected that the risk assessment would be a stronger predictor of self-harm during inpatient stay than history of self-harming alone. History of self-harm is just one of many factors considered by clinicians when assigning risk on admission. This would suggest then that when assigning risk, clinicians should consider giving more weight to history of self-harm, irrespective of other risk and protective factors, when making clinical judgements, particularly when assessing females. The nature, frequency and lethality of past self-harming behaviour were not recorded for the purpose of this study but are likely to have contributed to the level of risk assigned on admission and consequently warrant further research with respect to the prediction of self-harm.
The methodological limitations should be considered when interpreting the results of this research. This was a single-site, retrospective study and aggressive incidents were recorded from a critical incident report database rather than employing standardised tools to record aggression and a proxy measure of the severity of aggression was employed. Nevertheless, critical incident reports have been found to produce reliable information on aggressive behaviour (Garrison et al., 1990) and the current research sought to examine data related to the risk assessment of aggression in line with routine clinical practice. Risk factors with too few cases were excluded from regression analyses, in spite of significant correlations, due to violating the assumptions of logistic regression. Predictor variables, such as a primary diagnosis of a psychotic disorder, could not be analysed for the predictive validity of aggression, although correlation analyses suggested a possible relationship.
The baseline frequency of aggression varies across different community and clinical populations and was not accounted for in this study. In the current sample, the base rate of aggression was very low. Low base rates can result in high error rates in the prediction of aggression (Borum, 1996). Adolescents with a significant history of aggression were excluded from the MDAU between January 2007 and February 2009 because of WorkSafe limits and renovations that took place in the unit. As a result, only mood disordered adolescents without a history of aggression were admitted for a substantial proportion of the data collection period and results may not be representative of mood disordered adolescents. In fact, this was the case for the entire adolescent sample as the MDAU based its admission criteria on history of aggression during this time. In refusing to admit adolescents with a history of aggression, the unit successfully reduced aggression for this period. During this time only eight (6.8%) patients were recorded to have become aggressive compared with 13 (17.3%) during the period prior to and following the restriction period. In addition, there was an extended period, during which time, limited numbers and no males were admitted to the unit as they failed the test for history of violence. This resulted in fewer than normal admissions and a skewing of the sex balance towards female patients. This needs to be considered when interpreting the results around the relationship between sex and aggression.
Conclusion
The current research sought to examine the predictive validity of unstructured clinical risk assessment in predicting self- and other-directed aggression in adolescent inpatients. Based on professional expertise, prior experience and intuition, clinicians were found to be relatively good at predicting other-directed aggression in adolescent inpatient units; however, they were less successful at predicting self-directed aggression in this population when relying on unstructured clinical risk assessment. It is possible that environmental and contextual factors associated with self-harm were removed from the individual’s environment during admission to the inpatient unit. It may also be the case that treatment was effective in reducing risk during inpatient stay. Given that a history of self-harm was the strongest predictor of engagement in self-harm on the unit, there is opportunity for an improved risk assessment measure and this could be further improved by examining the features of past self-harming behaviours and their contribution to risk of future self-directed aggression.
Footnotes
Acknowledgements
The authors would like to thank the staff at the Austin Health CAMHS for their assistance with this research. We would particularly like to acknowledge Menka Krcoska, Ward Clerk.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.