
Abstract
Overt and impulsive aggressive behaviours, incorporating verbal abuse or physical aggression, are one of the most common reasons for referral in young people presenting to child and adolescent mental health services [1–3]. Impulsive aggression is considered a reliable construct: it can be measured, it occurs across a variety of disorders and it may be informative about the severity but not the type of illness [4]. Aggression in young people may reflect impaired developmental capacity to regulate behaviours, linked with impulsivity and poor affect regulation [5], and is a strong predictor of adult psychopathology [6]. Despite the importance of responding therapeutically to aggression and behavioural disturbances in young people, inpatient psychiatric units may be reluctant to admit young people at risk of physical aggression due to assumed safety concerns and perceived lack of clinical benefit [7]. In some circumstances this may act as a barrier to treatment access in young people at high risk for aggression during admissions.
Identifying high-risk patients is essential for providing targeted interventions to prevent aggression in inpatient settings, and can enable clinical teams to optimize the therapeutic environment for the needs of young people exhibiting aggressive behaviours. But one of the challenges in this area is the substantial heterogeneity of research findings. For example, although one study reported that aggressive behaviour during admission was not linked to any specific diagnosis [8], other studies have reported an association between inpatient aggression and developmental disorders [9], mental retardation [9], [10], disruptive behaviour disorders [9], [11], and learning disorders [11]. Other patient features linked to aggression include younger age [12], male gender [12], and history of abuse, neglect or foster care [8], [13]. Self-harming behaviour has been reported to co-occur with aggression [8], [13], and is sometimes referred to as ‘self-directed aggression’ [14], yet the role of self-harming behaviour as a predictive factor has not been adequately examined.
Although evidence is emerging to suggest that hospitalization alone [15] or behavioural management during admission [3] may reduce aggressive behaviour, there is little evidence available to inform our understanding of the admission outcomes of young people exhibiting aggression. Barton et al. report that involvement in critical incidents increased risk of poorer outcomes, as rated retrospectively from medical charts [11]. Aggression during admission has been associated with longer length of stay [16] and increased use of concurrent routine medications [17]. It is not well established how aggressive behaviours might impair admission outcomes. Possible mechanisms include the detrimental effects of coercive interventions such as restraint [12], [18] or changes in nursing behaviour that may impair the therapeutic relationship [19]. To the best of our knowledge there are no prospective studies examining the effects of aggression during admission on clinical outcomes and symptom changes.
The aim of the present study was to address this gap by examining aggression in a child and adolescent mental health inpatient unit. Specifically, we sought to (i) describe frequency of aggressive behaviours within the unit; (ii) compare patients exhibiting physical aggression with other patients; and (iii) examine whether aggression during admission impaired clinical outcomes. We hypothesized that aggressive behaviour during admission would be associated with increased duration of admission, increased use of routine psychotropic medications, and smaller improvements in symptom severity ratings between admission and discharge.
Methods
Study site
The study site was a 10-bed child and adolescent inpatient psychiatric, tertiary care unit that provided short- to medium-duration admissions including stabilization of crisis presentations, planned diagnostic assessments and brief intensive therapy. Care was provided by a multidisciplinary team of medical, nursing and allied health staff who specialize in child and adolescent mental health. This evaluation was conducted as a quality assurance activity. Most young people admitted to the unit exhibited complex psychopathology. The presence of aggressive behaviours unresponsive to outpatient interventions was an indication for inpatient assessment and management.
Ward policies for management of aggression utilized a comprehensive behavioural management programme [3], based on available treatment guidelines [1] and principles of the Positive Parenting Programme (Triple P) [20]. The primary component involved reinforcing appropriate behaviours (using verbal encouragement and individualized small rewards) and extinguishing disruptive and potentially dangerous behaviours, using a hierarchy of interventions, starting with the least restrictive possible. Interventions included engaging with the patient about behaviour choices, quiet time, time-out in a designated room (open or closed) or seclusion or pro re nata (‘as needed’; PRN) medication. This management approach was supported by individualized patient management plans, and staff training emphasizing consistent management and early intervention. This programme reduced the frequency of aggressive behaviour [3]. Patterns of medication prescribing and administration (both routine and PRN medications) have been reported elsewhere [21], [22].
Monitoring aggression
Between October 2004 and December 2005, all episodes of aggression were prospectively documented by nursing staff in a designated register at the time of the incident. Completing a written report following an incident has been demonstrated to produce reliable coverage of aggressive behaviour [12]. Types of aggressive behaviour documented were based on categories used in the literature [10–12], [23], and included physical aggression (directed towards staff, others or property) and non-physical aggression (verbal abuse and severe oppositional behaviour). Episodes of self-harming behaviour were also recorded.
Other information collected
For all patients medical charts were reviewed on site to collect additional information. For each patient the following information was collected: demographic details (age, sex, living situation); admission details (duration of admission; source of referral; history of previous admissions); and clinical details (diagnoses, history of abuse, suicidality (ideation or attempt), deliberate self-harm, and use of medications). Diagnostic assessments were undertaken prospectively during admission by child psychiatrists.
Clinicians also completed the Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA) at admission and discharge, as part of routine outcome monitoring. The HoNOSCA is a brief, clinician-rated measure of global mental health severity [24]. A total score was calculated from the first 13 scale scores, as reported elsewhere [25].
If a patient experienced more than one admission during the study period, the first admission with completed outcome data was selected for inclusion in the analysis.
Statistical analysis
Patients exhibiting persistent aggression were compared with other patients. Persistent physical aggression was defined as more than one episode of physical aggression during admission, as documented within the register of aggressive episodes. Group comparisons utilized independent samples t-tests for continuous variables (e.g. age, duration of admission) and χ2 tests for categorical variables (e.g. sex, key diagnoses, history of abuse). Variables significantly associated with persisting aggression were then modelled with logistic regression, effect modification tested by stratification, confounding by comparing crude and adjusted odds ratios and multi-colinearity by bivariate analysis followed by tests of homogeneity.
Changes in HoNOSCA scores over time were analysed using repeated measures analysis of variance (ANOVA) with the between-groups factor being aggression group (persistent aggression or not during admission) and the within-groups factor being time (admission and discharge). Analysis examined overall change in total scores between admission and discharge, and change over time between groups (interaction of time and treatment). For all analyses an alpha of 0.05 was used to determine statistical significance.
Results
Admission characteristics
During the study period, 134 patients were admitted to the unit. The mean patient age was 13.8 years (SD = 2.9, range = 5.8–18.0), and the majority of patients were female (83/134; 61.9%). Four patients (3.0%) were Aboriginal and Torres Straight Islanders. Average admission duration was 21.2 days (SD = 25.6, median = 12.0, range = 1–175), and 15.9% of patients had experienced a prior admission to the unit (21/132). More than one psychiatric diagnosis was assigned in 54% of patients (72/134; range = 0–4).
Most common diagnoses were mood disorders (39/134; 29.1%), anxiety disorders (29/134; 21.6%), attention-deficit–hyperactivity disorder and disruptive behaviour disorders (ADHD/DBD; 28/134; 20.9%); adjustment disorders (23/134 17.2%); and pervasive development disorders (PDD; 22/134; 16.4%). Almost half of all patients had a history of aggression (64/134; 47.8%), and a substantial proportion of patients had a history of abuse (34/134; 25.4%), deliberate self-harm (74/133; 55.6%) or suicidality (76/134, 57.1%).
Patterns of aggression
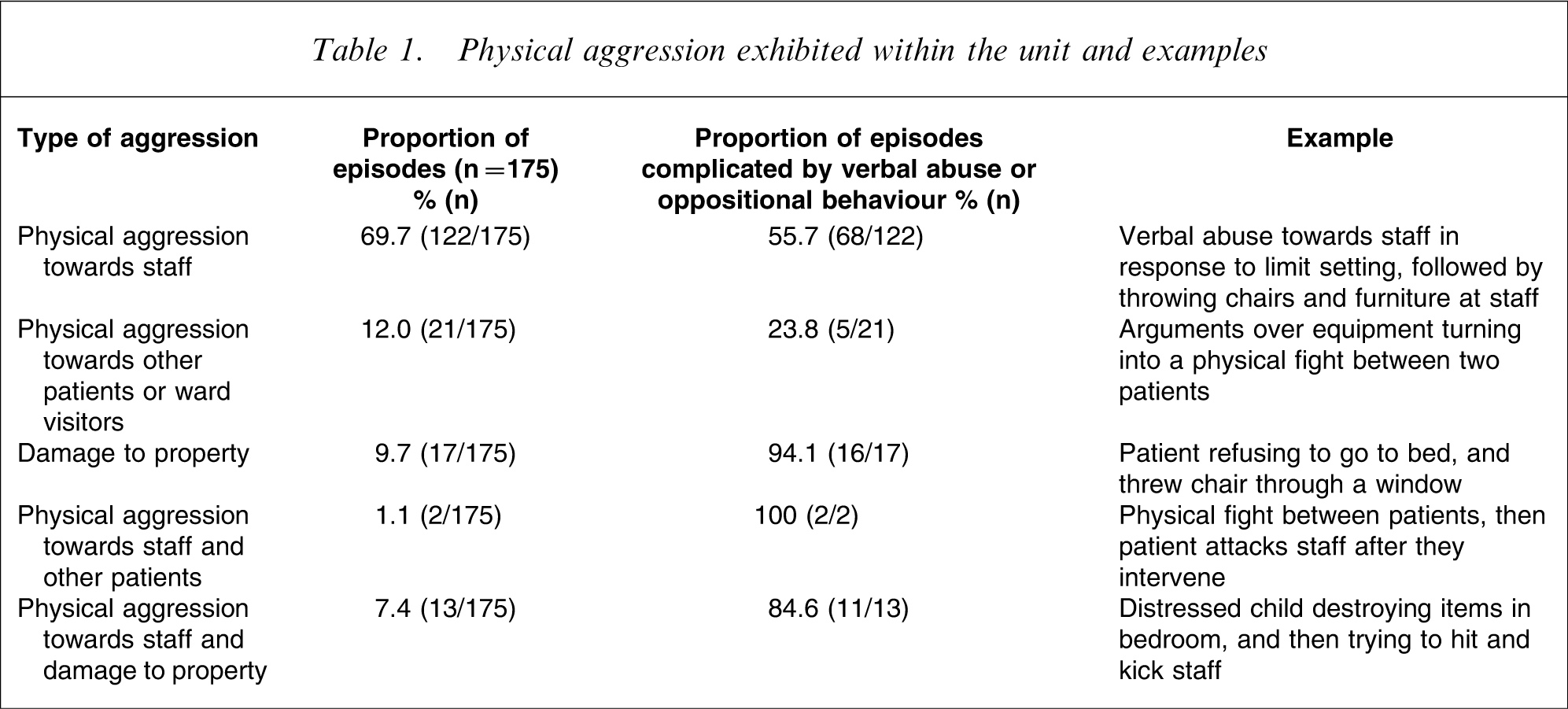
During the study period 31 patients (23.1%) exhibited any physical aggression during admission. The total number of episodes of physical aggression was 175. Eleven patients within this group exhibited only one episode; 16 patients exhibited 2–6 episodes, and four patients exhibited ≥10 episodes of physical aggression. The mean number of episodes per patient was 5.7 (median = 2.0, SD = 10.86, range = 1–53). The most frequent type of physical aggression was physical aggression directed towards staff, which contributed to 78.3% of incidents (137/175). Further descriptions about the aggressive incidents are reported in Table 1. As can be seen in Table 1, most aggressive incidents were also complicated by verbal abuse or oppositional behaviour.
Physical aggression exhibited within the unit and examples
Twenty-five episodes of self-harm were also documented, involving nine patients. Four adolescent girls did not exhibit any other form of aggression; they were admitted for suicide ideation and were diagnosed with a mood or anxiety disorder. The remaining five patients (three boys, aged 10–12 years) exhibited both aggressive behaviour and self-harm, and were diagnosed with ADHD/DBD, PDD or mental retardation. Patient numbers were insufficient to permit further statistical comparisons between these subgroups.
Predictors of persistent physical aggression during admission
Initial bivariate comparisons indicated that persistent aggression (more than one episode of physical aggression) during admission was associated with younger age (t = 3.63, p < 0.001), male gender (χ2=10.17, p < 0.01), a history of aggression (χ2=21.73, p < 0.001), use of psychotropic medications at presentation (χ2=12.62, p < 0.001), higher rates of PDD (χ2=14.00, p < 0.001), and ADHD/DBD (χ2=8.26, p < 0.05). Patients exhibiting persistent aggression were less likely to have a mood disorder (χ2=9.65, p = 0.001), a history of self-harm (χ2=15.75, p < 0.01), and suicidality (χ2=13.26, p < 0.01; Table 2).
Demographic and clinical characteristics of admissions with and without persistent aggression†
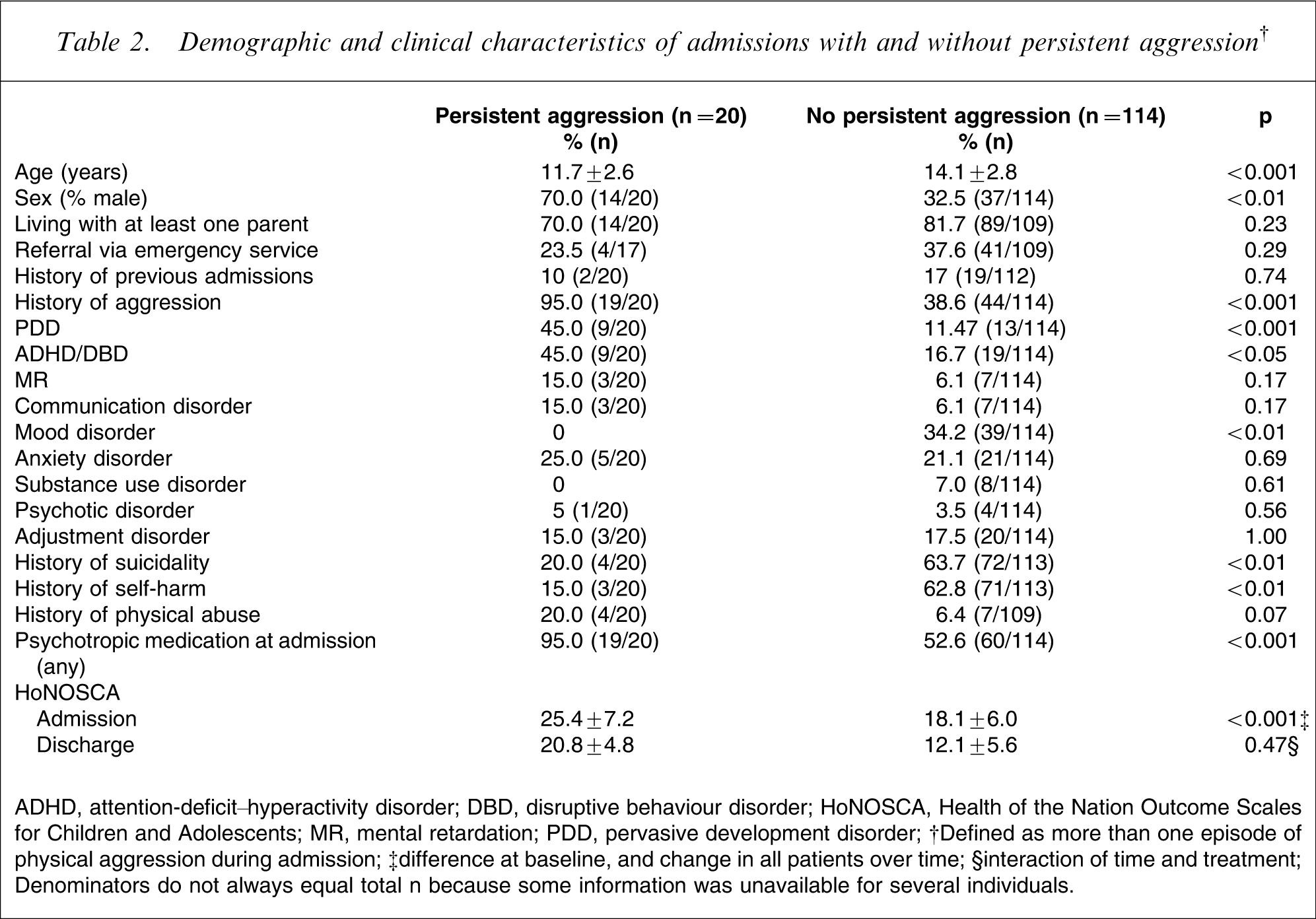
ADHD, attention-deficit–hyperactivity disorder; DBD, disruptive behaviour disorder; HoNOSCA, Health of the Nation Outcome Scales for Children and Adolescents; MR, mental retardation; PDD, pervasive development disorder.
†Defined as more than one episode of physical aggression during admission; ‡difference at baseline, and change in all patients over time; §interaction of time and treatment.
Denominators do not always equal total n because some information was unavailable for several individuals.
When these factors were then modelled using logistic regression, variables that remained independently associated with increased odds of persistent aggression included history of aggression, use of medications at presentation and absence of self-harm. Age, gender, diagnoses of PDD, ADHD/DBD, or problems related to mood disorders or suicidality were not significant (Table 3).
Logistic regression predictors of persistent aggression during admission
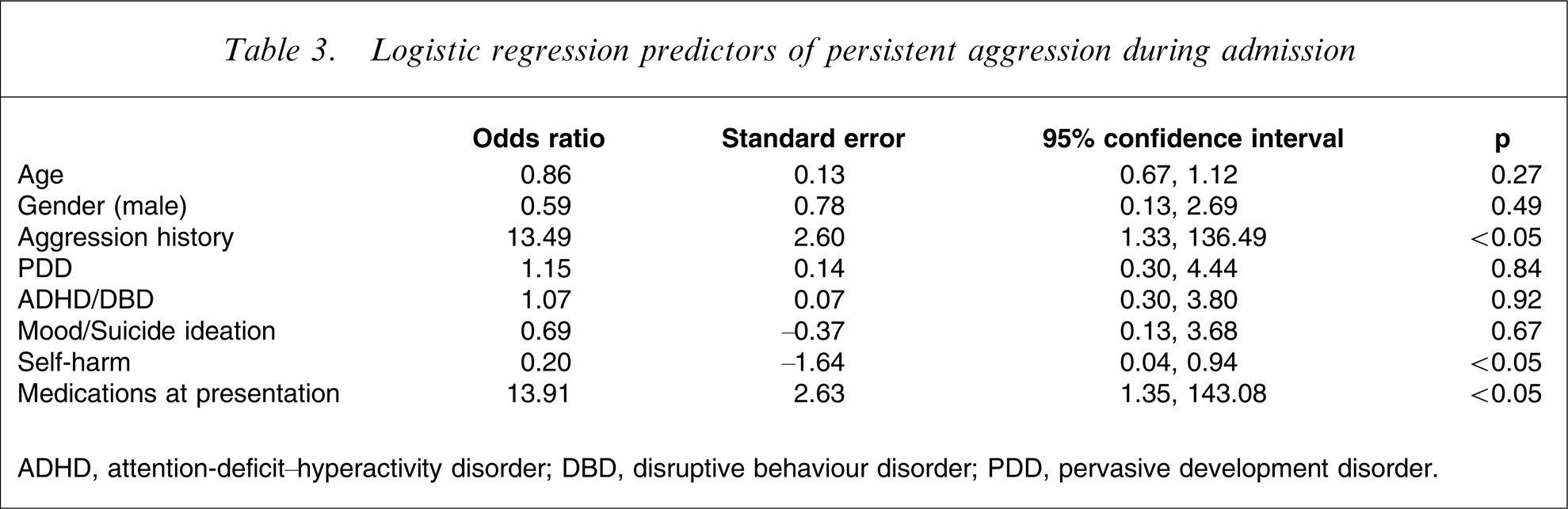
ADHD, attention-deficit–hyperactivity disorder; DBD, disruptive behaviour disorder; PDD, pervasive development disorder.
Impact of aggression on admission outcomes
Pre- and post-admission HoNOSCA scores were available for a subset of patients (47/134). There was a significant reduction in HoNOSCA total scores over time in all patients (F1,45=34.34, p < 001, ηp
2=0.43), but there were no significant differences over time between patients who were aggressive and those who were not (F1,45=0.54, p = 0.47, ηp
2=0.01; Figure 1). Similarly, when missing discharge data were ascribed baseline values there was a significant improvement over time in all patients (F1,69=22.66, p < 001, ηp
2=0.25), with no significant differences between groups (F1,69=0.09, p = 0.77, ηp
2=0.00). To assess whether this subset of admissions was representative, admissions with and without HoNOSCA ratings available were compared. No differences were detected for age, sex, presence of aggression, duration of admission, or key diagnoses.
Changes in symptom severity as rated by the Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA) between admission and discharge, for admissions with and without persistent aggression (defined as more than one episode of physical aggression during admission).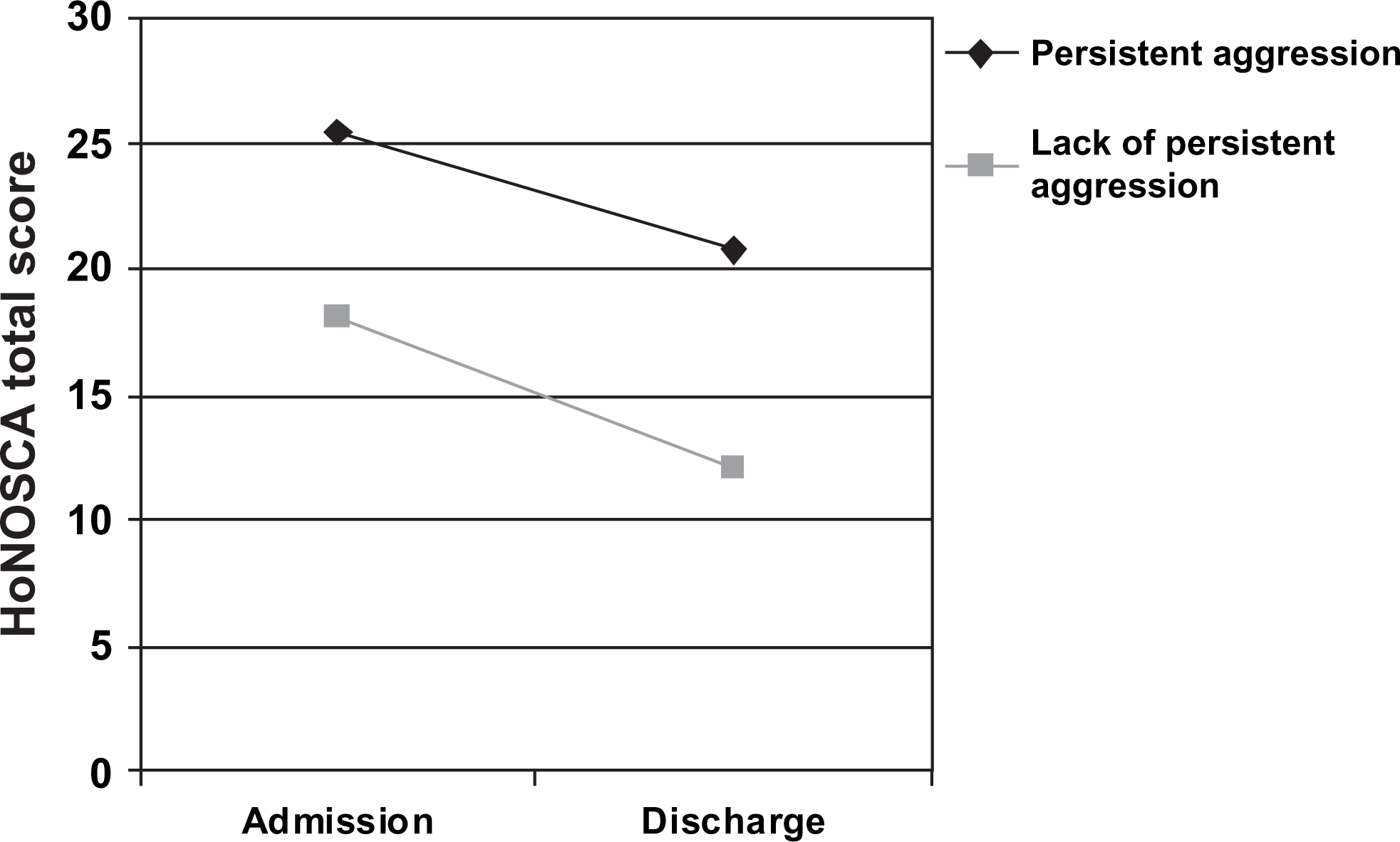
There were no differences in medication changes between groups: 15.8% (3/19) of admissions in which aggression occurred resulted in an increase in number of medications used, compared to 15.0% (17/113) of admissions in which aggression did not occur (χ2=0.01, p = 1.00). Rates of polypharmacy did not change between admission and discharge. For patients exhibiting aggression, polypharmacy rates were 55.0% (11/20) at admission and 52.6% (10/19) at discharge. For other patients, 24.6% (28/114) were receiving polypharmacy at admission, and 22.1% (25/113) were receiving polypharmacy at discharge.
Patients exhibiting persistent aggression had a significantly longer length of stay (mean = 33.4 days, median = 22.5, SD = 32.2) compared to other patients (mean = 19.1days, median = 11.0, SD = 23.8; t = − 2.34, p < 0.05). Patients exhibiting persistent aggression were more likely to be referred to intensive treatment services after discharge (16.7% vs 7.3%) but this was not statistically significant (χ2=1.57, p = 0.20).
Discussion
The aim of the present study was to examine predictors of persistent physical aggression and its impact on admission outcomes in children and adolescents admitted to a psychiatric inpatient service. Factors that predicted persistent aggression included history of aggression, use of medications at presentation and absence of self-harm. Aggression was associated with a greater length of stay but, contrary to our hypotheses, aggressive behaviour during admission did not lead to increased number of medications and did not compromise improvement in symptom severity as measured on HoNOSCA.
Less than one-quarter of patients exhibited physical aggression during admission. This rate is lower than rates reported elsewhere, which range from 41% to >90% [8], [9], [11]. There are a number of differences between the present population and those in previous studies that may explain differences in findings. In contrast with the present study, in which average length of stay was approximately 3 weeks, Connor et al. reported a rate of physical aggression exceeding 90% in a long-term residential unit in which the average length of stay approximated 3 years [8]. Both patient characteristics and environmental determinants of aggressive behaviour may differ between short- and long-stay units. Nonetheless, the present findings suggest that high rates of physical aggression are not inevitable in short-term inpatient facilities. It is possible that the lower rates of aggression observed in the present study were due to existing behavioural management policies within the unit.
Significant independent predictors of persistent aggression during admission included history of aggression, use of medications at presentation and absence of self-harm. Much existing research also reports that history of aggression is a major risk for aggressive behaviour during admission [8], [9], [11–13], [26]. The significance of medication use at presentation may stem from medications acting as a proxy marker for severity; patients receiving psychotropic medication may represent a clinical subgroup for whom non-pharmacological interventions have been ineffective. This finding also indicates that use of medication in itself does not prevent emergence of aggressive behaviour, and that aggression-specific strategies may still be required in young people receiving medication.
The role of other patient factors such as diagnosis in predicting aggression is unclear from the present findings and the existing literature. The lack of clarity about this issue highlights the possibility that environmental factors such as unit characteristics and approaches to aggression management may be stronger predictors of behaviour than patient factors [12], [16], [27], [28]. This reinforces the importance of examining aggression risk as an interaction between patient factors and environmental factors, rather than being determined by patient characteristics alone. It is also possible that the predictors of mild aggression may differ to predictors of more serious or frequent aggression. Unfortunately the present sample size was not large enough to assess the differential predictors or impact of differing aggression severities. Predicting risk of aggression or violence is a challenging task and the present findings do not permit development of a simple risk prediction tool. Identifying high-risk patients potentially allows more targeted strategies for prevention, but it remains unclear whether this is more effective than providing such interventions for all patients. It is likely that a combination of milieu-based and individualized interventions may be most appropriate for managing aggression in this clinical environment.
A number of interesting associations were observed between persistent aggression and internalizing symptoms. A number of reports link self-harming behaviour with aggression [8], [13], suggesting that they are related behaviours. But only three patients in the present cohort exhibited both behaviours during admission. Furthermore, a history of self-harming behaviours was linked to a lower risk of aggression. These findings suggest that self-harm and aggression are not inevitably linked; further research is required to clarify this relationship. Aggression may occur in young people with mood disorders [29]. But we observed lower rates of aggression in admissions in which a mood disorder was diagnosed. This has been reported elsewhere [9]. It is possible that young people with mood disorders respond well to the therapeutic effects of inpatient admission, and are less likely to externalize distress. Alternatively, the presence of aggression during admission may influence the diagnostic process.
There is limited research examining clinical outcomes in young people exhibiting aggressive behaviour during inpatient admission. The process of determining whether a young person is suitable for admission to an inpatient unit is complex and based on many factors, such as individual needs, severity of presentation, availability of alternative interventions and capacity for the child to benefit from admission. This process is likely to differ substantially between units. Our findings suggest that young people exhibiting aggression may still receive some benefit from admission, and that excluding young people from inpatient services based on aggression risk alone could be considered unethical because it denies them potentially effective treatment.
Patients exhibiting persistent aggression experienced longer admissions. Aggression may be a symptom that requires a longer duration of treatment to resolve. Alternatively, parents and carers may be more anxious about the child returning home from hospital and this might delay the discharge process. It is possible that longer admissions permitted the observed clinical improvement to occur.
The relationship between aggression and greater symptom ratings at admission has been reported elsewhere [30], and reinforces the need to consider the needs of this group within a therapeutic framework. The present findings are in contrast to those of Barton et al., who reported that critical incidents during admission were associated with poorer clinical outcomes [11]. There are a number of key differences between these two studies that may explain the contrasting results. Critical incident reporting, used by Barton et al., typically captures more severe behaviours and includes a range of non-aggressive behaviours (e.g. running away), compared to the register of aggressive incidents as used in the present study. Different types of incidents may differentially influence outcome. Additionally, the present outcomes were rated prospectively, not retrospectively from charts. It is possible that the presence of aggression influences clinical information recorded in charts, which may have influenced retrospective ratings of outcome; it is unclear whether aggression may have influenced HoNOSCA ratings of improvement in the present study. The generalizability of the present findings needs to be confirmed given the small number of patients for whom pre- and post-outcome data was available. Nonetheless, the present findings suggest that young people with aggressive behaviours can exhibit significant improvement in symptoms with inpatient care.
Although young people admitted to inpatient units for aggressive behaviour often receive increases in concurrent medication use during admission [17], aggression during admission did not lead to increases in number of routine medications or rates of polypharmacy. This may reflect high rates of medication use and polypharmacy at admission, and that inpatient admission is often a time for reviewing medications and discontinuing them in a safe and well-monitored environment [31]. It is possible that aggression may have influenced medication use in other ways, such as dose increases. Further research is required to increase our understanding of the effects of aggression on patterns of medication prescribing.
The present study had a number of limitations. Aggressive incidents were not recorded using standardized instruments, but were recorded in a designated register by nurses at the time of incident. While this potentially allows subjective bias to act as a systematic source of error, other studies suggest that completing a report following an incident is a feasible technique that produces reliable coverage of aggressive behaviour [12]. Severity of incidents was not recorded. It was conducted in a single unit, which limits the generalizability of the findings. The small sample size resulted in low power to detect potentially important group differences; for example, a larger sample size may have generated a significant relationship between aggression and physical abuse or other factors. Outcome data for the HoNOSCA were available only for a small subset of patients, so these findings may not be fully representative and should be considered preliminary only. Nonetheless, to the best of our knowledge this is the largest study examining aggression and prospectively rated clinical outcomes within a child and adolescent inpatient unit.
In conclusion, aggression during admission was more likely to occur in those with a history of aggression, receiving medications at presentation and without a history of self-harming behaviour. Contrary to hypotheses and existing research, aggression during admission does not appear to be a barrier to clinical improvement. Further research is necessary to clarify how children and adolescents with aggressive behaviour can receive the most benefit from inpatient admission while minimizing the risks to the patient and those around them.