
Abstract
Many countries report higher rates of suicide mortality of Indigenous populations compared to non-Indigenous [1], including Australia's Aboriginal and Torres Strait Islander people [2]. The underlying causes of Indigenous suicides have been linked to factors such as colonialism and difficulties integrating into mainstream societies [3]. The size of this problem is believed to be increasing: Hunter et al. [4] found a more than three-fold increase in numbers of Australian Indigenous suicides between 1990 and 1996, while an older study in South Australia reported an even more dramatic increase in rates in the period from 1981 (10.1 per 100 000) to 1998 (105.3 per 100 000) [5].
While the dire public health implications of Indigenous suicides are increasingly recognized in Australia, comprehensive assessments of the scope and complexities remain scarce. Reasons for this include inaccurate classification systems (exclusion of equivocal deaths and misclassification of suicides on compassionate grounds to avoid community/familial distress), and incomplete data collection processes (variations in coronial practices and only partial geographical coverage) [2,6,7,8,9]. The lack of quantitative accounts of Indigenous suicide obscure understanding about the size of the burden of suicide, the age groups that might be at particular risks, and the use of suicide methods.
Questionable accuracy of information on ethnicity is a further problem in the Australian context, due to the definition of ‘ethnicity’ being a multi-dimensional concept based on self-perception [10]. This means that population figures and mortality data of Indigenous people rely on the self-attributed identification with an ethnic group. Additionally, the overall degree of incompleteness of Indigenous mortality data has been estimated to be as high as 56% [11]. In regard to suicide deaths, Tatz [2] maintains that actual rates, particularly for Indigenous youths, can be at least two to three times greater than those officially recorded.
The main aim of this paper was to provide information on trends of Indigenous suicide over the period 1994 to 2007 in Queensland, based on data from the Queensland Suicide Register. To the authors’ knowledge, this data source contains comprehensive information on the biggest sample of Indigenous suicide deaths investigated to date in Australia. A further aim was to determine the size of underreporting of Indigenous suicide mortality that occurred in this period due to absence of information about the ethnicity.
Materials and methods
Data were extracted from the Queensland Suicide Register (QSR), an independent database of suicide mortality. This register includes demographic, psychosocial, psychiatric and behavioural aspects of all suicides by Queensland residents from 1990 to present, currently comprising more than 10 000 cases. Information is obtained from police reports (since 1994 including psychological autopsy questionnaires), post-mortem analysis and toxicology reports. Detailed processes behind management of the QSR data have been explained in more detail elsewhere [12].
Sample
In the QSR, ethnicity is recorded as Caucasian, Aboriginal/Torres Strait Islander (TSI), Asian, other or unknown. As this coding system does not differentiate between Aboriginal or Torres Strait Island ethnicity, in this paper the term ‘Indigenous’ was used to define people of Aboriginal and/or Torres Strait Islander origin.
Prior to 1994, when psychological autopsy questionnaires with specific questions on ethnicity were added to the forms used in police investigations, 42.9% of the cases in the QSR did not contain that type of information. Since then, recording of ethnicity has markedly and progressively improved. After 2001, only 1.1% of cases remained of unknown ethnicity.
To avoid gross under-enumeration of the prevalence of Indigenous suicide deaths, only cases between 1994 and 2007 were included in the analysis. During this period the QSR collated 7672 cases of suicide. Of those, 471 (or 6.1%) were of Indigenous ethnicity, 6655 (86.7%) were of Caucasian, Asian or other ethnicities, and 546 (or 7.1%) cases were of unknown ethnicity. The latter group was analysed separately.
Statistical analysis
Suicides rates for Indigenous and non-Indigenous populations were age-standardized using the direct standardization method and WHO world standard population 2000–2025 [13] to adjust for considerable differences in the age distribution of the two groups. Rate ratios for all men and women were calculated by dividing suicide rates of the Indigenous group with those of the non-Indigenous group. Age-specific rates were calculated using the mean of population figures between 1994 and 2007 for Indigenous and non-Indigenous Australians [14,15].
Poisson regression was implemented to assess for time trends of Indigenous and non-Indigenous suicide rates, and for trends of hanging over time.
A tentative estimation of the ethnic composition of the subgroup with unknown ethnicity (546 cases or 7.1% of the total sample) was carried out by canonical discriminant analysis [16]. The following predictors were simultaneously entered into the analysis: age at the time of death, use of hanging as a suicide method, presence of physical illness(es), presence of mental illness(es), unipolar depression, relationship problems, recent unemployment, work or school problems, financial problems, conflict (with friends or family), and pending legal problems. The discriminating functions were used to predict the proportion of cases with unknown ethnicities which were likely to be of Indigenous or non-Indigenous descent; however, only cases with a probability of belonging to the respective group above the average probability were ultimately added to the ‘actual sample’.
Results
Rates and trends of suicide mortality
Trends of age-standardized suicide rates for Indigenous and non-Indigenous men and women are presented in Figure 1. Indigenous suicide rates show considerable fluctuations over the years, ranging in men from the lowest of 32.8/100 000 in 2002 to the highest of 64.1/100 000 in 2000, while in women the lowest rate was 2.2/100 000 in 1994 and the highest 16.6/100 000 in 2007. Results of the trend analysis showed no statistically significant time-trends in either non-Indigenous or Indigenous suicide; in the latter group this was possibly due to large variations in rates between time periods.
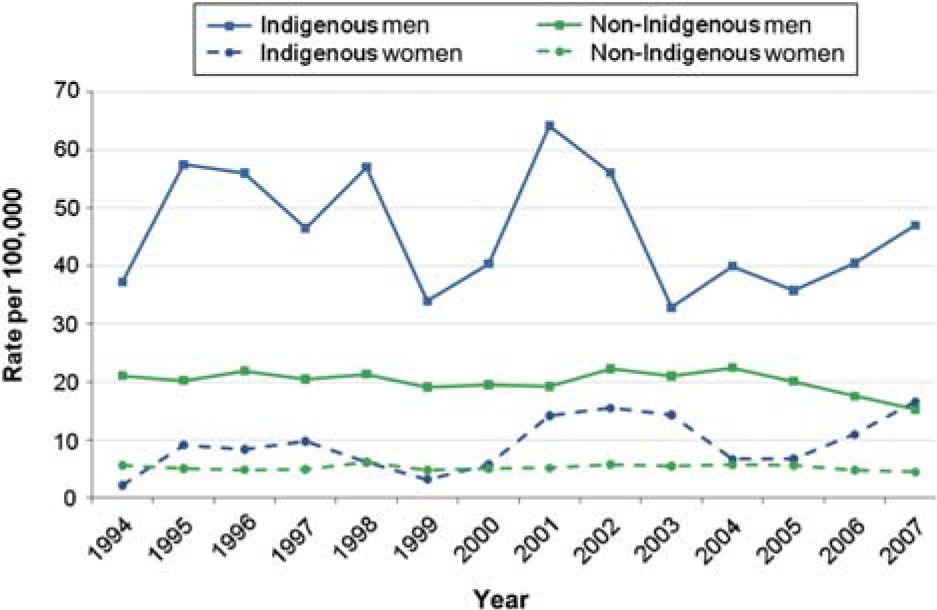
Age-standardized suicide rates, Indigenous and non-Indigenous populations, Queensland, 1994–2007. (Colour version of this figure available online)
Rate ratios of age-standardized suicide mortality between 1994 and 2007 show, on average, 2.2 times higher risk for suicide of Indigenous persons than their non-Indigenous counterparts (27.2 versus 12.6 per 100 000). This ratio was somewhat more pronounced among men (2.3:1; 54.8 versus 21 per 100 000) than in women (1.8:1; 9.4 versus 5.3 per 100 000). Ratio of male versus female suicide mortality for the studied period was higher in Indigenous populations (4.9:1) than in non-Indigenous populations (3.8:1).
Age-specific suicide rates
Age-specific suicide rates for Indigenous and non-Indigenous groups are presented in Table 1. In the Indigenous population, the highest rates were for men and women between ages 15 and 34, with young male rates reaching almost 100 suicides per 100 000 population, while in non-Indigenous people this was observed for age groups 25–34 and 35–44. In comparison to the non-Indigenous counterparts, Indigenous youth had a risk for suicide four times higher in 15–24 year olds and 2.8 times higher in the 25–34 age group. There was almost a ten times greater risk of suicide in Indigenous children (younger than 15 years) compared to non-Indigenous children; however, wide confidence intervals suggest poor precision of this estimate. In individuals older than 55 years, results showed greater rates of suicide mortality in non-Indigenous than Indigenous people; however, there were only six cases of suicide among Indigenous population in this age group (all men).
Gender and age-specific suicide rates, Indigenous and non-Indigenous populations, Queensland, 1994–2007.
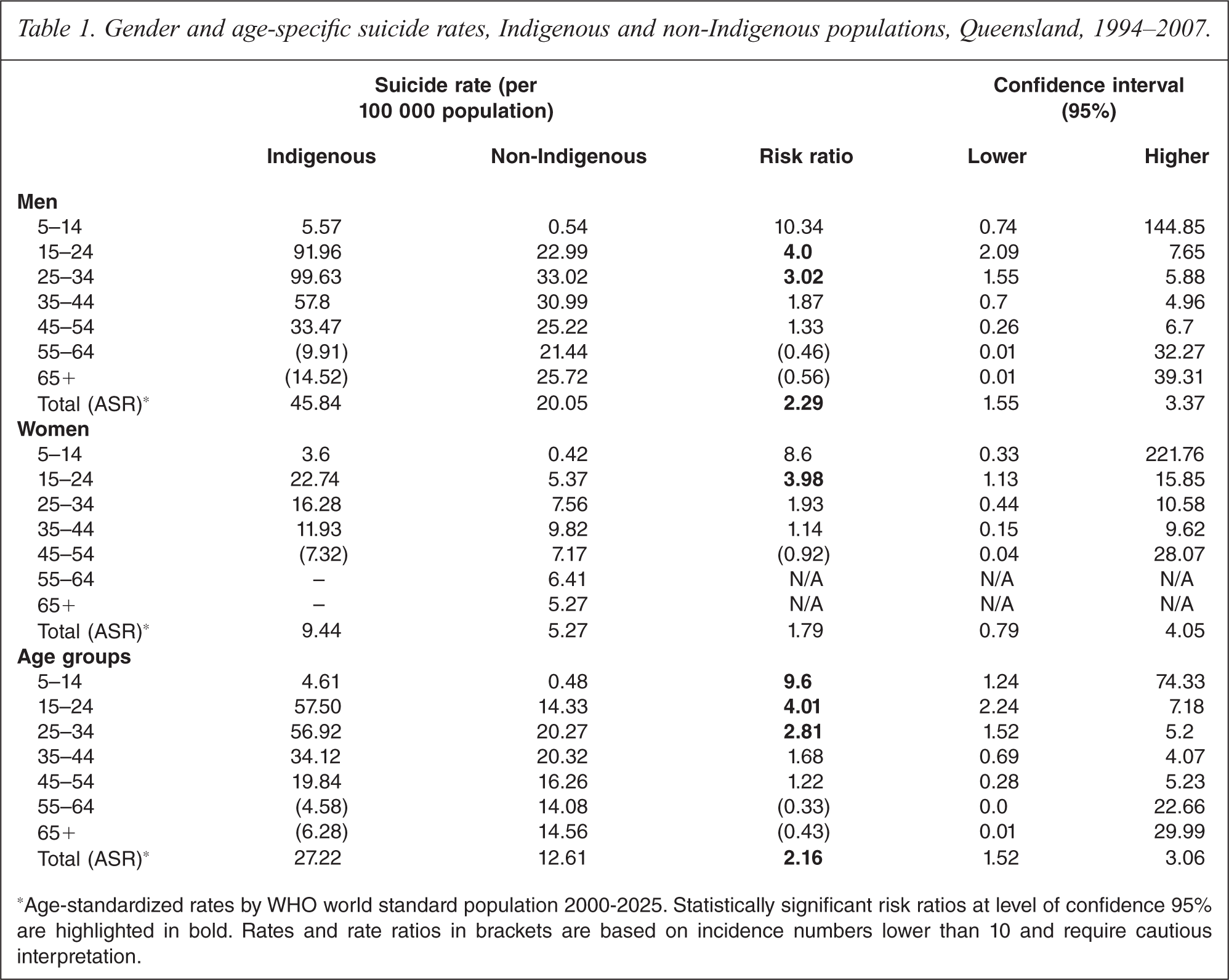
*Age-standardized rates by WHO world standard population 2000–2025. Statistically significant risk ratios at level of confidence 95% are highlighted in bold. Rates and rate ratios in brackets are based on incidence numbers lower than 10 and require cautious interpretation.
Trends of suicide rates by age groups for Indigenous people are presented for ages below 24 years, 25–44 years and over 45 years (see Figure 2). These groups were formed to ensure a sufficient number of cases within each group to allow for calculation of annual rates. Nevertheless, the incidence in young Indigenous women was still very low and warrants cautious interpretations. There was a significant increase in suicide among young Indigenous women aged 24 years and below (p < 0.001) and women aged between 25 and 44 years (p < 0.001). In contrast, there was a significant decrease in young Indigenous men (p < 0.001) over the time period 1994 to 2007. In other age groups there was no observable trend.
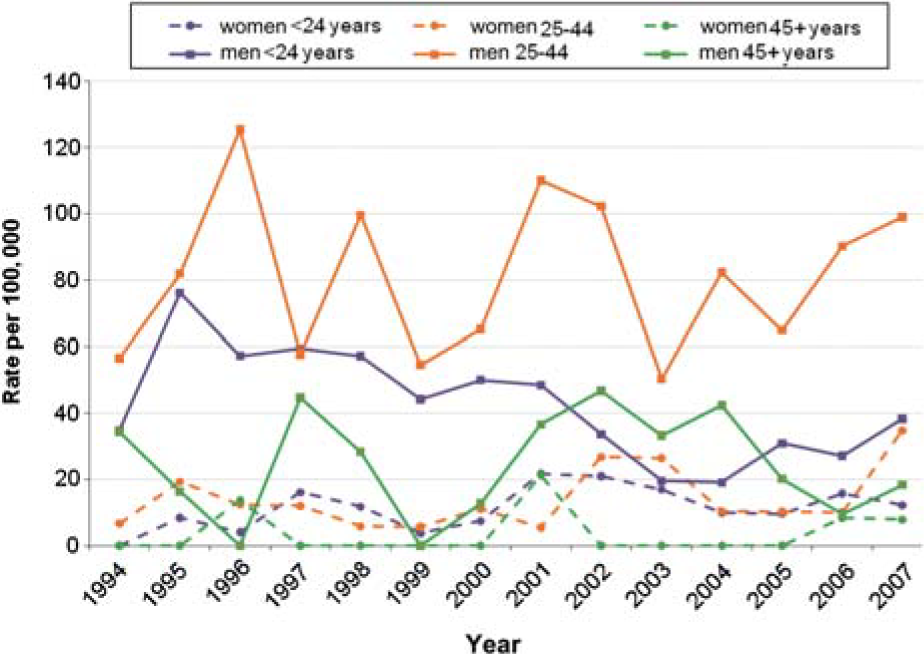
Age-specific crude suicide rates for Indigenous men and women, Queensland, 1994–2007.
Suicide methods
In the Indigenous population, the majority of male and female suicide cases used hanging (Table 2); the rate of using this method was on average 4.6 times higher than in non-Indigenous people (for both genders). Poisson regression revealed no observable trend in use of hanging in suicide by Indigenous persons.
Suicide methods in Indigenous and non-Indigenous populations, Queensland, 1994–2007.
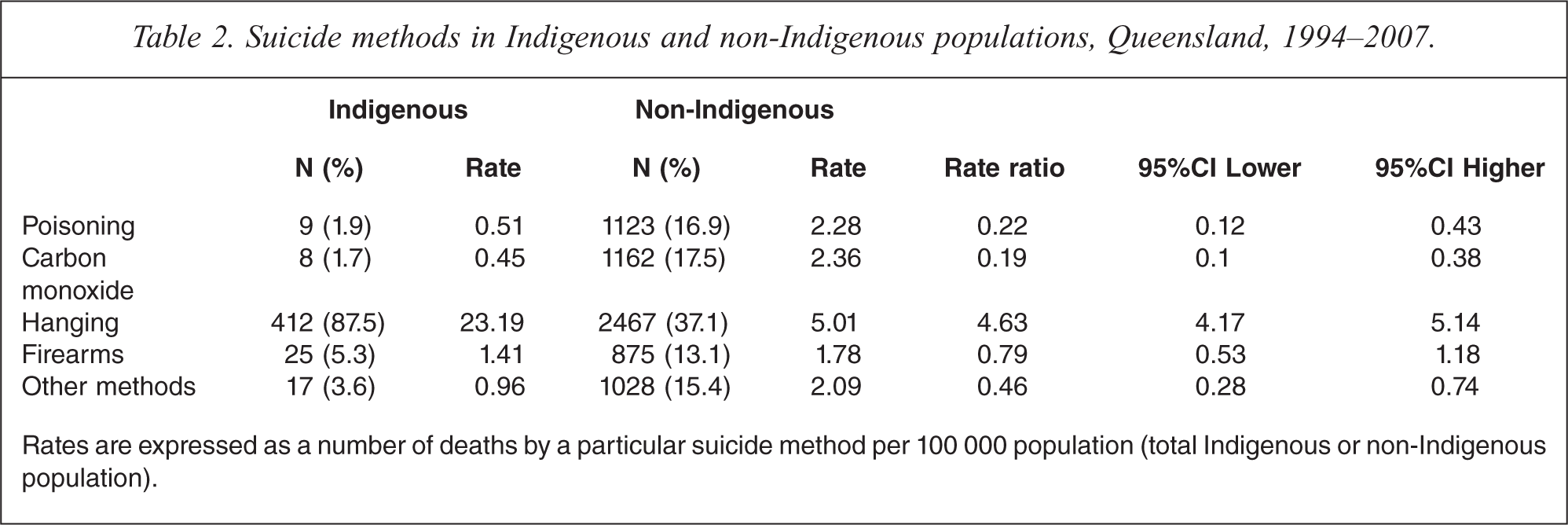
Rates are expressed as a number of deaths by a particular suicide method per 100 000 population (total Indigenous or non-Indigenous population).
Apart from hanging, all remaining methods had very low frequency among Indigenous populations (with the exception of the year 1994 in which five Indigenous suicides occurred by firearms, there have been four or fewer suicides each year utilizing a method other than hanging). This prevented calculation of temporal trends of use of other suicide methods.
An estimate of unreported suicide cases of Indigenous ethnicity
Lack of information about the ethnicity of the deceased in a non-negligible number of suicides (7.1%) has possibly led to under-estimation of Indigenous suicide rates. We conducted discriminant analysis to predict the ethnicity of these cases based on the characteristics of the 471 confirmed cases of Indigenous and all other non-Indigenous suicides. Two canonical functions, both statistically significant (p < 0.001) were found to explain differences between Indigenous and non-Indigenous suicides. As seen in Table 3, the most prominent features of Indigenous suicides were their younger age and the use of hanging as a method (function 1), while all remaining predictors loaded on function 2. Exceeding the average posterior probability of 0.621405, 73 ‘predicted’ Indigenous cases (65 men and 8 women) were added to the ‘actual’ sample of Indigenous suicides.
Results of the discriminant analysis: structure coefficients.
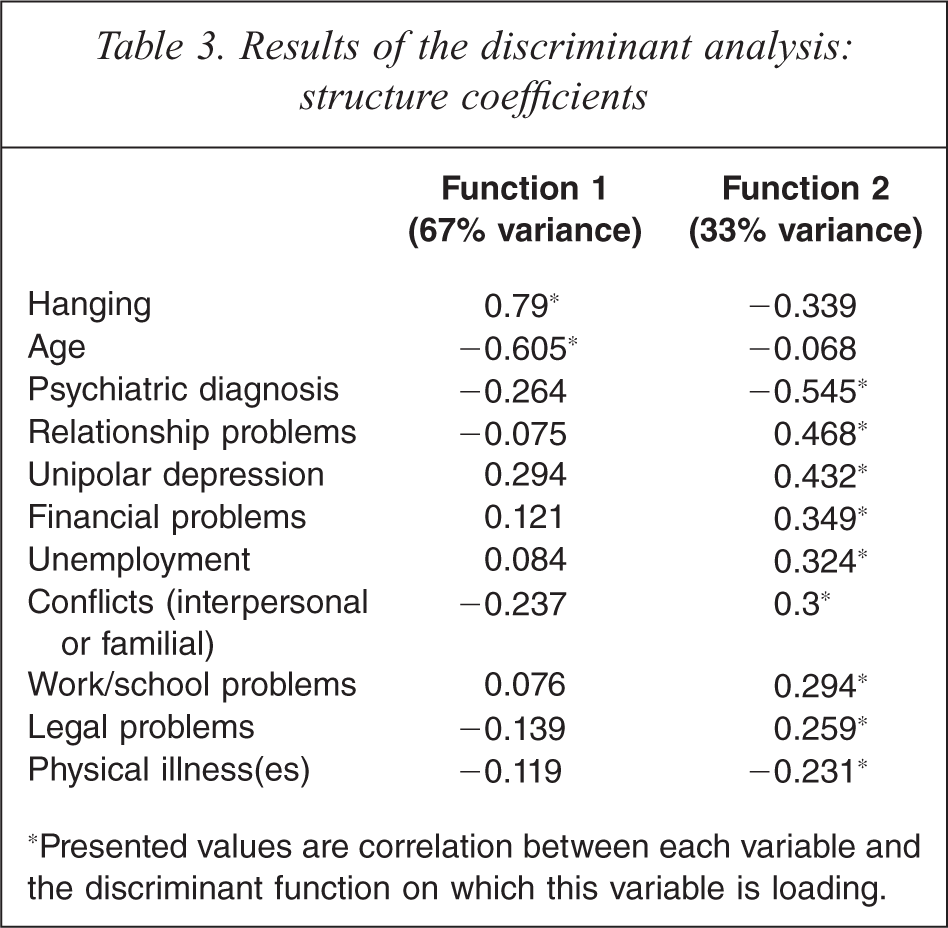
*Presented values are correlation between each variable and the discriminant function on which this variable is loading.
With this technique, inclusion of probable cases of Indigenous ethnicity increased the suicide rates in the period 1994–2007 by 15.4% for men and 9.1% for women (14.4% for both genders). It should be noted, however, that the majority of this under-reporting occurred in the period 1994–2000; after 2001 only around 1% of cases did not carry information about ethnicity. This would correspond to two additional cases, both men, eventually increasing suicide rates by 0.6% for the period 2001–2007.
Discussion
Indigenous people have suicide rates more than double those of non-Indigenous populations. This evidence aligns with a few past reports [4,11,17,18]. Trends of Indigenous suicide showed considerable fluctuations in the period 1994–2007. For example, between 1999 and 2003, numbers of suicides of Indigenous women have gone from 1 to 10 per year (in this same time period, rates for non-Indigenous women increased only by 8%). Another marked change in rates occurred between 2004 and 2007, in which time Indigenous male rates rose by 29%, while non-Indigenous male suicide showed a decrease by 32%. Marked discrepancies between trends of Indigenous and non-Indigenous people suggest that factors influencing suicide mortality of Indigenous people might be different to those affecting suicides in general populations.
Indigenous people aged below 34 years had rates about three times higher than non-Indigenous populations, with young men exceeding 90 deaths per 100 000 population. Notwithstanding the low numbers of suicide deaths in Indigenous children below 15 years of age (21 cases in the period from 1994 to 2007), comparison of their rates with non-Indigenous peers demonstrated 9.6 times higher suicide risk. These high rates of suicide among children represent one of the most alarming features of suicidality in Indigenous people.
To some extent, the much higher burden of suicide among younger Indigenous Australians can be explained by important differences in the age structures between the Indigenous and non-Indigenous groups. In 2006, median age of Indigenous people in the general population was 21 years, compared to 37 years in the non-Indigenous population [19]. Yet, calculation of age-standardized rates was implemented to counter for these influences. Additional explanations for the distinct age-distribution of suicides might include general disadvantages in living conditions, education, and employment [11,20], earlier exposure to alcohol and drug use (two of the most prominent factors increasing risk for suicide) [21], more frequent experiences of deaths by members of the community [22], and effects of ‘suicide contagion’ and clusters of attempted and completed suicides [23,24]. The latter phenomenon might also help explain observed marked fluctuations in suicide rates of Indigenous people.
This study confirms the predominant role of hanging in suicides of Australian Indigenes [2,4]. Between 1994 and 2007, this method was recorded in almost 90% of Indigenous suicides, corresponding to a rate almost five times higher than that of non-Indigenous suicides. A marked increase in the use of hanging as a suicide method has been observed in many countries worldwide [25], including Australia, where hanging now constitutes the most common suicide method and one that continues to grow in frequency, particularly among young men [26]. This phenomenon has been linked to its increased social acceptability following the abolition of judicial hanging [27,28]. Utilization of suicide methods is also believed to be strongly influenced by cultural factors [29], and in the case of Indigenous suicides hanging has been viewed as a form of political protest, expressing anger at historical racism [30]. Alternatively, it could be argued that the predominant choice of hanging (not only in Indigenous but in most populations of western countries) is more reflective of its availability [31]. This could be particularly applicable to Indigenous populations, which may have limited access to a variety of means commonly utilized in suicidal acts (e.g. firearms, drugs and motor vehicle exhaust gases).
Discriminant analysis identified two characteristics of Indigenous suicide that most strongly differentiated them from non-Indigenous suicides: their younger age and predominant use of hanging. This helped to estimate the possible under-reporting of suicide deaths without information on ethnicity: between 1994 and 2007 the rates of Indigenous Australians might in fact have been higher by an average 14.4% than that reported.
Among limitations it should be acknowledged that suicidal deaths may remain unregistered due to inadequate mortality recording systems, remoteness of locations, and frequently itinerant lifestyle of inhabitants of Indigenous communities (presently it is not possible to gauge their proportion). In addition, the often troublesome relationship between Indigenous people and police may affect the thoroughness of investigation of suicidal deaths and increase the odds of their misclassifications. Current unavailability of comparable suicide databanks in other states and territories prevents deliberation about potential generalizability of our findings to the rest of Australia; however, comparative analysis of geographical distributions of suicide mortality in Indigenous populations would be of great relevance for national suicide prevention programmes.
Conclusion
Findings of this study represent a significant contribution to the current knowledge about the dimension of Indigenous suicide mortality in Queensland. Results highlight the need for future research to elucidate the complex associations of suicide risks among Indigenous Australians, particularly in youths, who display a markedly higher suicide rate than other age groups. While considerable advances have recently been made in Australia through advocating for the development of a separate suicide prevention strategy for Indigenous communities [32], it is recommended that such initiatives be driven by evidence-based research.
Footnotes
Declaration of interest
This study was funded by Queensland Health, Mental Health Directorate. The authors alone are responsible for the content and writing of the paper.